
Abstract
Purpose
In modern total knee arthroplasty (TKA), flexion and extension gaps between the femur and tibia are equilibrated before implanting the final components. Uncontrolled intraoperative posterior tibial translation (PTT) could cause an artifactual widening of the flexion gap, which could lead surgeons to alter the femoral component size. We designed an intraoperative posterior sagging control device to prevent intraoperative PTT. In this study, we investigated whether the use of this device could prevent artifactual widening of the flexion gap.
Methods
Twenty-five patients, 21 women and four men, aged 74.2 years, were enrolled in this prospective study. All patients underwent postero-stabilized TKA using a navigation system. Intraoperative PTT, flexion and extension gaps with or without using the posterior sagging control device were measured with navigation system. These measurements were compared with or without the posterior sagging control device and after the final implantation also.
Results
There were significant differences between the measurements performed with or without the posterior sagging control device when compared to the post-implantation measurements. The use of the device reduced the number of patients with a >3 mm increase in flexion gap from 7 (28%) to 1 (4%).
Conclusion
This study suggests that the posterior sagging control device prevents PTT and artificial flexion gap widening. This could prevent an unnecessary increase in component size.
Introduction
Despite successful total knee arthroplasty (TKA), an estimated 20% of patients report dissatisfaction 1 due to unexplained pain and stiffness.2–4 These complications were considered to result from an oversized or overhanging component,5,6 which can lead to soft tissue impingement7,8 or patellofemoral overstuffing.9,10
Soft tissue balancing is an important step in successful TKA, enabling the surgeons to determine the optimal component size.11,12 One of the goals of soft-tissue balancing is to equilibrate flexion and extension gaps while minimizing joint line elevation, thereby guaranteeing optimal knee kinematics and preventing coronal knee laxity. 13
Modified gap technique is one of the most established surgical maneuvers for total knee replacement. In this procedure, the step for making the optimal flexion gap space is most important. Suitable flexion gap assessment should be performed for avoiding both the optimal femoral component sizing and the controlled femoral component rotational positioning. Intraoperative posterior tibial translation (PTT) during ligament balancing in posterior-stabilized (PS) TKA with modified gap technique is reported. This uncontrolled intraoperative PTT can cause an artifactual widening of the flexion gap, 14 which may lead to femoral component oversizing, and in turn, to poor knee kinematics or coronal laxity. 5 The important step before assessing flexion gap is controlling the tibial translational and rotational positionings against the femur.
We have developed a novel posterior sagging-control device (PSCD) for controlling intraoperative PTT during flexion gap assessment with modified gap technique. In this study intraoperative PTT and flexion gap during procedure were measured with navigation system in which with or without PSCD. The hypothesis was that intraoperative PTT and flexion gap would be significantly decreased when using the PSCD, that controlled PTT was working for selecting the suitable femoral component sizing.
Materials and method
Patient inclusion
All patients who underwent primary unilateral TKA for knee osteoarthritis and were operated upon by a single surgeon using the Stryker eNact Precision Knee Navigation System software (Stryker Co., Allendale, NJ, USA) in our hospital between February 2018 and August 2018 were prospectively enrolled in this study. The initial cohort comprised 28 patients, but three patients were diagnosed with rheumatoid arthritis and were excluded from the study. The final study cohort included 25 patients (21 women and four men) aged 74.2 years (52–87 years). All patients received Stryker-cemented Triathlon PS (Stryker Co., Allendale, NJ, USA). The study was approved in advance by the Institutional Review Board, and all patients provided verbal informed consent to participate in the study.
Information about the novel device
The base plate of the PSCD has the same shape as the tibial base plate and is fixed with pins so that the tibial component is placed in the same position as the tibial implant (Figure 1). The PSCD was developed for each size (1–6) of the tibial implant. The central plate that controls posterior tibial sagging has a scale for measuring the flexion gap. The central plate is located at an average distance from the post-cam of the femoral implant, which is compatible with the tibial implant, to the distal femoral resection plane. The maximum error is 1.11 mm, depending on the combination of components of different sizes (Table 1). A removable plate with rotation in 5° increments from 0° to 15° was also developed so that it could be selected according to the patient’s anatomy. The plate with rotation was designed such that the rotation axis and angle of the medial pivot matched. This plate was designed to reproduce the internal tibial rotation during femoral flexion. A motion analysis of the Triathlon (PS) suggested that tibial rotation at 90° knee flexion is approximately 5° internal rotation on average, although there are individual differences.
15
A posterior sagging-control device (PSCD). Pictures of the PSCD from above (a) and side (b). The selection of the rotation angle was bidirectional (0, 5, 10, and 15°) (a). The alignment rod was scaled to allow the evaluation of the flexion gap (b). (c) Showed the diagram how to control the sagging. Error in posterior sagging between post-cam and PSCD in the femur compatible with the tibia (mm).

Surgical procedure
All patients underwent a midline knee incision using the medial parapatellar approach and received Stryker cemented Triathlon PS (Stryker Co., Allendale, NJ, USA). Osteotomies of the distal femur and proximal tibia were performed first, after which osteophytes were resected, and the soft tissue was balanced. We performed resection of the femur at 2° flexion against the mechanical axis and at 3° to the mechanical axis of the tibia. The posterior extension gap was larger than the anterior extension gap when the knee was fully extended.
5
Therefore, we evaluated the extension gap by dividing it into anterior and posterior extension gaps using spacer blocks to determine the appropriate flexion gap. The size and position of the tibial component were then determined using the trial components. The PSCD was then fixed to the planned location of the tibial component with the knee flexed to control sagging of the tibia. The rotation of the tibial component is referred to as the Akagi’s line. Flexion and rotation were adjusted such that the base plate of the PSCD fits the distal femoral resection plane. Then, using lamina spreaders, a spreading force was applied between the tibial resection plane and the posterior femoral condyle. A 5° central plate was used in all cases. The resection line of the posterior condyle was marked (flexion gap) according to the posterior extension gap (Figure 2). The Ranawat block was placed on the marked resection line of the posterior condyle to determine the size and insertion location of the femoral component. The resection line of the posterior femoral condyle was adjusted to match the posterior extension gap because of the posterior translation of the contact area between the femur and the tibia during flexion while determining the flexion gap. The standard polyethylene (PE) insert size is usually 9 mm, although in cases with residual instability, an insert size of 11 mm or more is used to compensate for the flexion gap. Intraoperative picture illustrating the use of the posterior sagging-control device, to determine the resection line (white arrow) of the posterior condyle.
Intraoperative measurements
Intraoperative PTT and flexion gap were evaluated using the Stryker eNact Precision Knee Navigation System software. Posterior tibial translation was defined as the distance between the perpendicular line from the distal femoral articular surface to the proximal tibial articular surface and the tibial axis (Figure 3(a) and (b)). The pre- and post-implantation differences of PTT and Flexion gap were compared between with and without PSCD. Flexion and rotation angles at the time of measurement of each patient were measured using the Stryker eNact Precision Knee Navigation System software. The limb position at the time of measurement was not standardized between patients. Negative values for PTT indicated posterior translation, while positive values indicated anterior tibial translation. Since PSCD was developed based on the mean femoral component size compatible with the tibial component size, there were errors depending on the combination of sizes. Posterior tibial translation (PTT) was defined as the distance between the perpendicular line from the distal femoral articular surface to the proximal tibial articular surface and the tibial axis. We measured the PTT with (Figure 3(a)) and without (Figure 3(b)) the posterior sagging-control device. The white arrow indicates the PTT distance.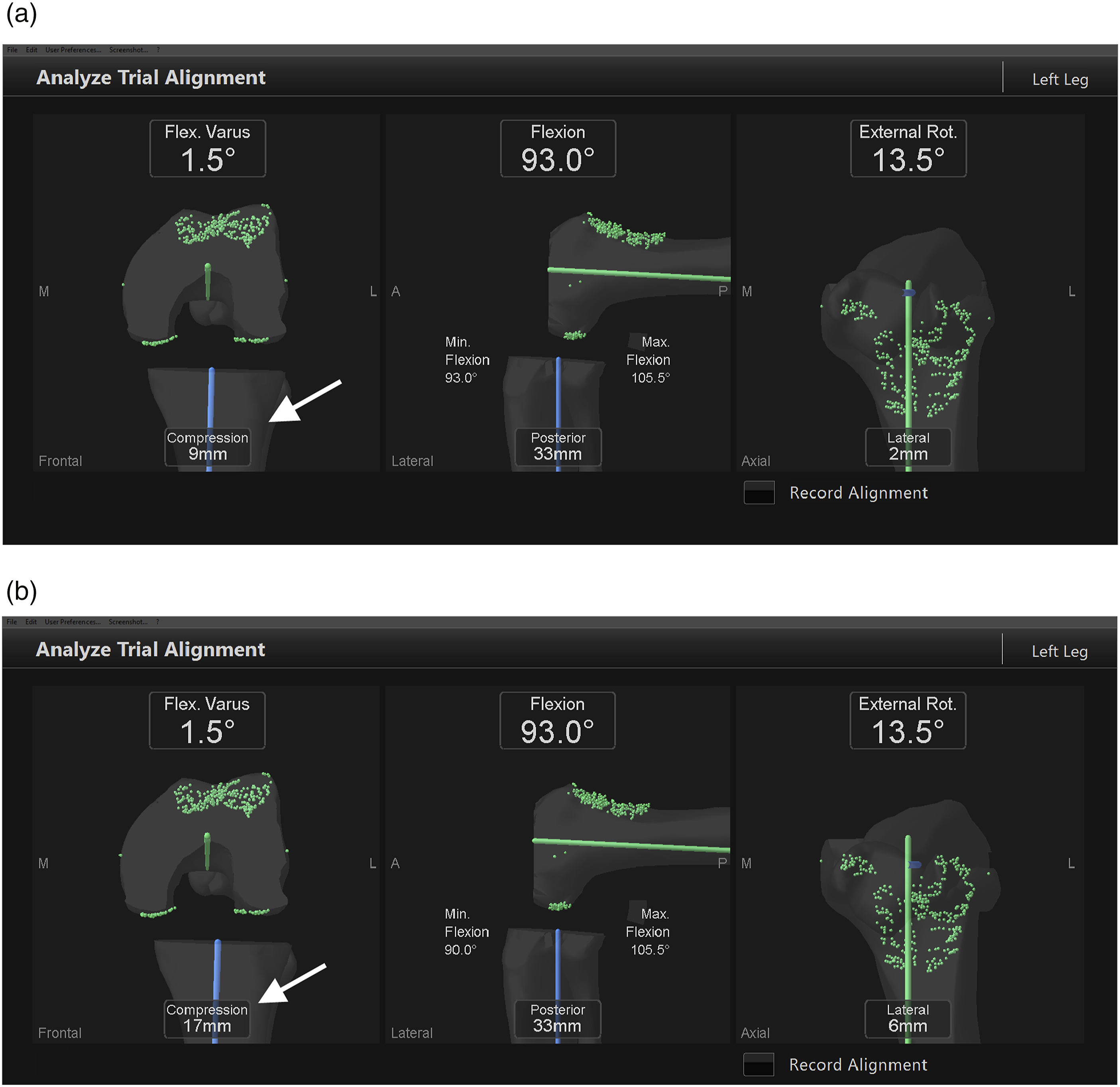
Statistical analyses
Data were analyzed using analysis of Paired t-test. Statistical significance was set at p < 0.05. Measurements for continuous variables are presented as mean ± standard deviation (range), while those for categorical variables are presented as n (%). All statistical analyses were performed using StatView software (version 5.0; Apple Inc., Cupertino, CA, USA). A post hoc Student’s t-test was performed to determine whether the sample size provided sufficient statistical power to detect significant factors. The post hoc power analysis showed that a sample size of 25 achieved a power of 80% and significance level of 5%, which verified the adequacy of the present sample size.
Results
Patient characteristics.

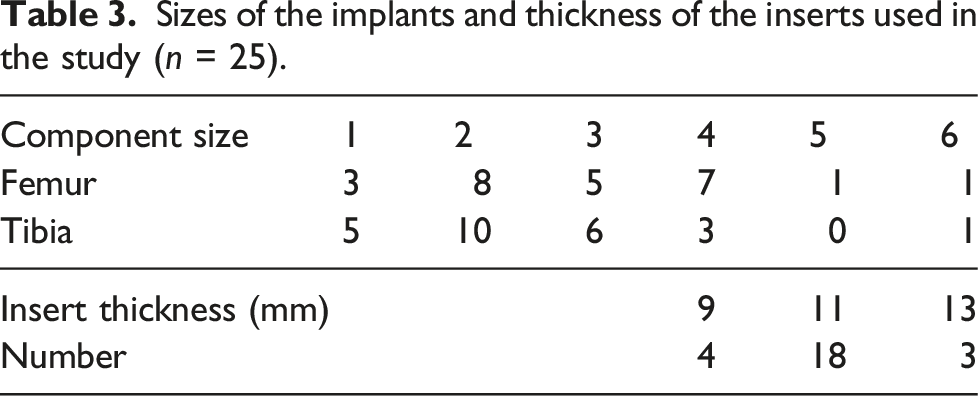
Sizes of the implants and thickness of the inserts used in the study (n = 25).
The mean difference in measured PTT between post-implantation and intraoperative measurements using the PSCD was −0.76 ± 1.42 mm (−4.0 to 2.0 mm). The mean difference between post-implantation and intraoperative measurements without using the PSCD was −6.04 ± 2.68 mm (−11.0 mm to −1.0 mm) (p < 0.0001) (Figure 4(a)). Since the PSCD was developed based on the mean femoral component size compatible with the tibial component size, there were errors depending on the combination of size. The mean difference in measured PTT between post-implantation and intraoperative measurements using the PSCD, after adjusting for errors, was −0.82 ± 1.46 mm (−3.87 to 1.80 mm). The mean difference in measured PTT between post-implantation and intraoperative measurements without using the PSCD, after adjusting for errors, was −6.01 ± 1.93 mm (−10.2 to −1.5 mm). The number of patients with >3 mm PTT was 3 (12%) using the PSCD and 22 (88%) without using the PSCD. (a): Difference (mm) between postoperative measurements of posterior tibial translation (PTT) and intraoperative measurements of PTT. (b): Intraoperative measurements of the flexion gap (mm) when standard insert sizes are used. (c): Intraoperative measurements of the flexion gap (mm) when adapted insert sizes are used. Thinner inserts are used to compensate for the flexion gap when it is overestimated, leading to a compensation mechanism.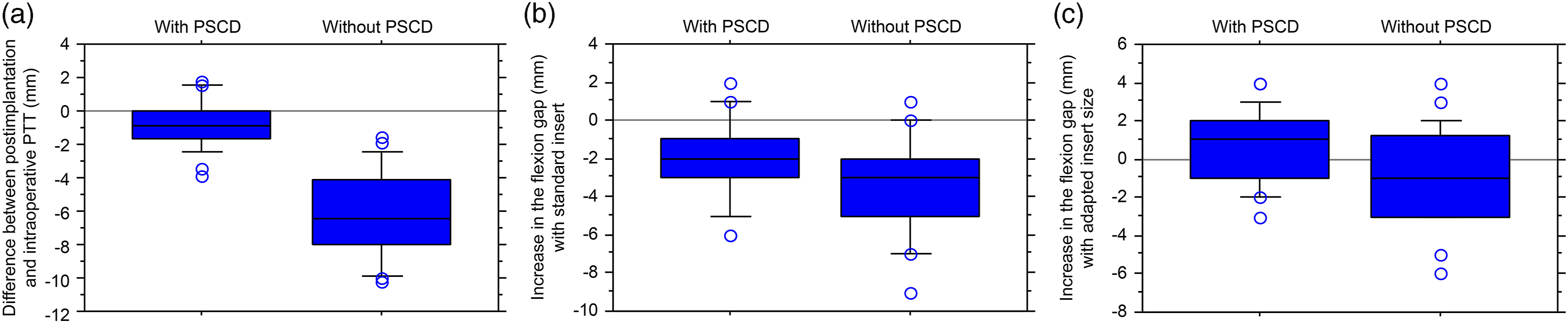
A negative value for the flexion gap indicates an increase, while a positive value indicates a reduction in the gap. The mean difference of flexion gap between post-implantation and intraoperative measurement using the PSCD was −1.96 ± 2.07 mm (−6.0 to 2.0 mm). The mean difference of flexion gap between post-implantation and intra-operative measurement without using the PSCD was −3.44 ± 2.46 mm (−9.0 to 1.0 mm). There was a significant difference between the two groups (p = 0.026) (Figure 4(b)). An increase of >3 mm in flexion gap was found in 10 knees (40%) using the PSCD and in 15 knees (60%) without using the PSCD (p = 0.157). The mean thickness of the selected inserts was 2.56 mm thinner than the distance between the tibial resection plane and resection line of the posterior condyle. When the flexion gap was corrected based on the above results, the mean difference between post-implantation and intraoperative measurements, using the PSCD, was 0.60 ± 1.93 (−3.0–4.0 mm). The mean difference between post-implantation and intraoperative measurements, without using the PSCD, was 0.88 ± 2.52 mm (−6.0 to 4.0 mm) (p = 0.024) (Figure 4(c)). After correction, only one knee (4%) presented an increase of >3 mm in flexion gap using the PSCD, compared to 7 (28%) without using the PSCD. Using the PSCD, the correlation coefficient between the PTT and the increase in the flexion gap was 0.124 (p = 0.5552). Conversely, without the PSCD, there was a weak positive correlation between the two variables (r = 0.412, p = 0.0405) (Figure 5). The correlation coefficient between posterior tibial translation and increase in the flexion gap without posterior sagging-control device.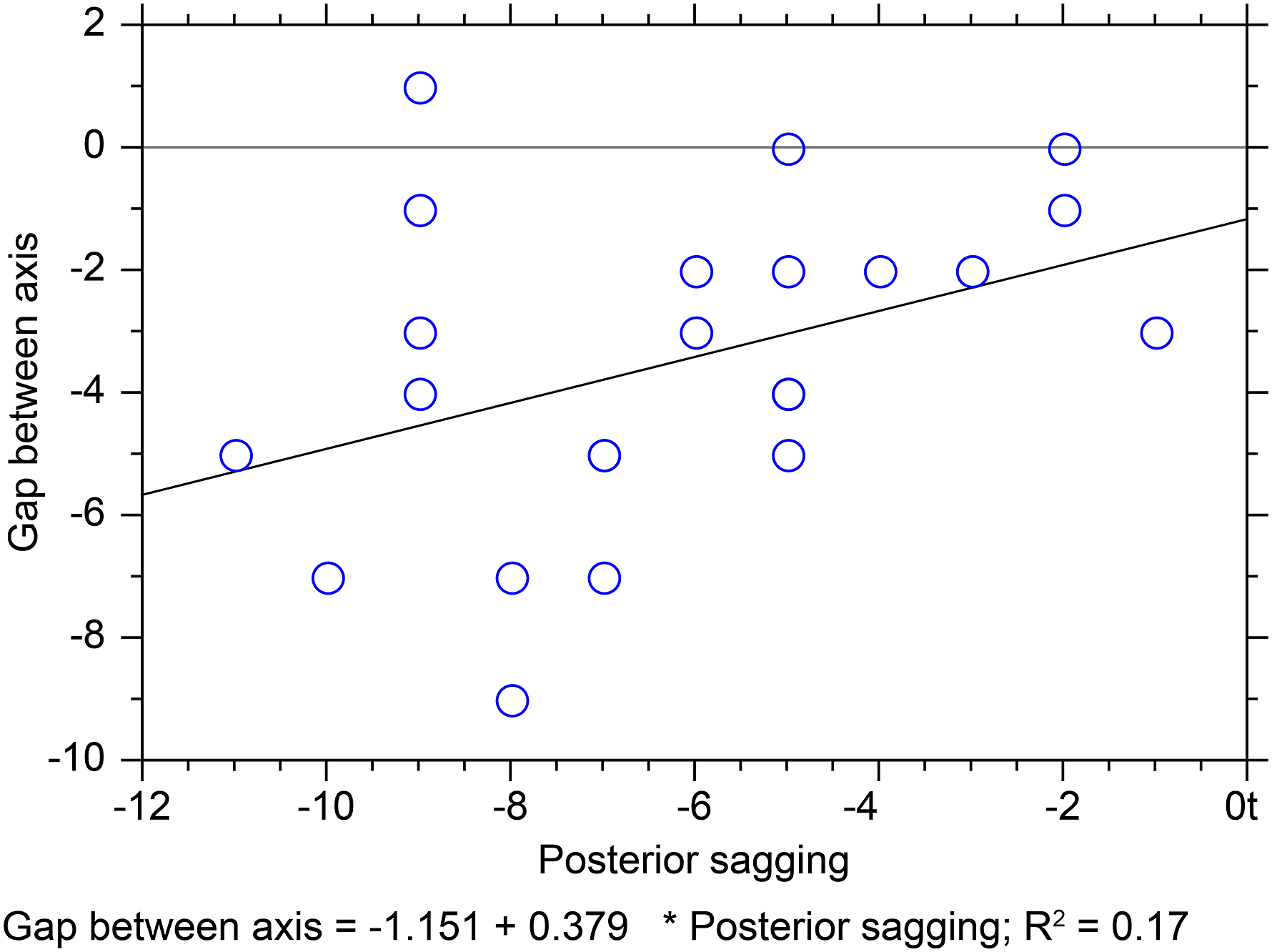
Discussion
The main finding of this study is that the use of the PSCD during ligament balancing reduces the PTT and widening of the flexion gap. When using PSCD, the number of patients with a PTT of more than 3 mm was reduced from 88% to 12%, while the number of patients with a flexion gap increase of more than 3 mm was reduced from 28% to 4%. In our practice, an increase of more than 3 mm in the flexion gap requires an increase in the size of the femoral component. Therefore, up to 28% of the patients could have received oversized femoral components. Moreover, there was a significant positive correlation between PTT and the flexion gap in knees when not using the PSCD, which disappeared when the PSCD was used. Taken together, these results suggest that the PSCD prevents PTT from influencing or affecting the flexion gap, thereby preventing overestimation of the flexion gap during soft tissue balancing and reducing the chance of component oversizing during TKA.
Component oversizing is reported to be a major cause of pain or dissatisfaction after TKA, as this may lead to prosthetic overhang and capsular overstuffing.16–19 The femoral component is particularly subject to oversizing, with reported rates reaching 66%–76%, with a demonstrated role in postoperative pain, stiffness, and poor functional outcomes after TKA.8,18 It is likely that uncontrolled PTT contributes to a significant portion of oversized femoral components. 14 Therefore, the systematic use of a PSCD to control intraoperative PTT could greatly reduce femoral component oversizing in TKA. However, it is important to note that other causes of implant-patient mismatch besides intraoperative PTT have also been reported in the literature. Excessive deformity correction may also lead to oversizing, particularly if under-resections are performed to maintain the joint line.6,20 Furthermore, despite the production of genre-21–23 or ethnic-specific implants, existing ranges fail to cover the polymorphism observed among populations.24–26 Further development of existing ranges, or the advent of patient-specific implants, may be necessary before prosthetic oversizing or overhang can be completely eliminated.
This study demonstrated the efficacy of a novel PSCD designed to prevent intraoperative PTT. The use of this novel device is thought to reduce the number of oversized femoral components during TKA with PS implants. However, this study had several limitations. First, the accuracy of our measurements depends on the navigation system used, and our observations may not translate to all surgical techniques. Second, our findings are based on a system using cemented implants and may not be applicable to uncemented systems. Finally, the device generated minor measurement errors. Depending on the size of the tibia, our PSCD gauges a measurement error of up to 1.11 mm from the post-cam to the distal femoral resection plane with a compatible femoral component. Future studies should address this issue. The use of cement during implantation may have contributed to greater PTT in patients with PSCD than in patients who underwent cementless implantation; moreover, the thickness of the cement was not evaluated in this study. In addition, the accuracy of resection, as well as the measurement accuracy of the navigation system and PSCD fixation on the tibia may have affected the results of this study. An appropriate rotation angle during the evaluation of the flexion gap still needs to be determined in future studies. Indeed, during the evaluation of the flexion gap, rotation and flexion angles may be affected by the severity of soft tissue contracture and the angle and accuracy of the resection (e.g. anterior and posterior inclination). These parameters were not evaluated in this study and will need to be investigated in future research.
Conclusion
This study suggests that uncontrolled intraoperative PTT could result in an overestimation of the flexion gap and an unnecessary increase in component size. The posterior sagging control device effectively controlled the intraoperative PTT, thereby reducing the associated artifactual widening of the flexion gap, and in turn, preventing femoral component oversizing.
Footnotes
Acknowledgements
Editorial support in the form of medical writing was provided by Editage, Cactus Communications.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
This study was approved by the institutional review board of Keijinkai Kawasaki Hospital (IRB No. 2024) and was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Consent to participate
Verbal informed consent for participation was obtained from all patients.
Availability of data and material
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Unblinded statements
All patients who underwent primary unilateral TKA for knee osteoarthritis and who were operated upon by a single surgeon using the Stryker eNact Precision Knee Navigation System software (Stryker Co., Allendale, NJ, USA) in Keijinkai Kawasaki Hospital between February 2018 and August 2018 were prospectively enrolled in this study.