
Abstract
Purpose
Fixed bearing (FB) UKA constituted 63.7% of unicondylar knee arthroplasties in 2020 Australian Registry with the longest UKA survivorship. The significance of patellofemoral joint (PFJ) arthritis, ACL deficiency, post-operative anteromedial pain, radiosclerosis or radiolucency on survivorship of FB UKA is not established. The aim of this study was to analyze the medium-term survivorship of fixed-bearing UKA with no exclusion of PFJ OA and ACL deficiency. Predictors for failure were analyzed.
Methods
FB UKA performed in 2011-17 were reviewed. Cases with PFJ OA or ACL deficiency were not excluded. The effect on survivorship by ACL deficiency, PFJ arthritis, post-operative anteromedial pain and radiological abnormalities were analyzed.
Results
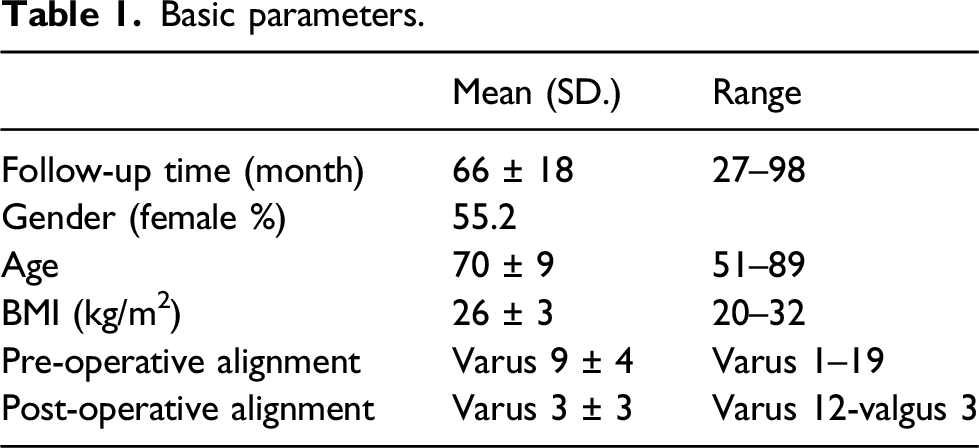
There were 96 UKA with follow-up time of 66 ± 18 months (27–98). The mean age was 70 ± 9 years, BMI 25.8 ± 2.6 kg/m2. Alignment was varus 9° ± 4° pre-operatively and varus 3° ± 3° post-operatively. There were four revisions (4.2%) and 4 deaths (4.2%). Reasons for revisions were loosening (n = 1), persistent pain (n = 2) and lateral compartment disease (n = 1). Estimated survival at 8.3 years was 94.7% (95% CI 91.6–97.7). BMI ≥30 was found to be a significant predictor for failure. The incidence of radiographic abnormalities was 75% for PFJ arthritis, 39% for tibial tray overhang, 14% for radiolucency or radiosclerosis, 5% for ACL deficiency and 5% for edge loading respectively but they were not significantly associated with lower survivorship or anteromedial knee pain. The presence of anteromedial pain after surgery in 36.5% was also not significantly associated with survivorship.
Conclusion
FB UKA with no exclusion of early PFJ arthritis and ACL deficiency has satisfactory medium-term survivorship. BMI ≥30 could have higher risk of all-cause revision. Tibial tray overhang, non-progressive radiolucency or radiosclerosis do not seem to be associated with anteromedial knee pain or poorer medium term survivorship.
Keywords
Introduction
Unicondylar knee arthroplasty has gained popularity in the last decade. It has contributed up to 8% of knee arthroplasty surgeries. 1 Despite the recent enthusiasm in mobile-bearing (MB) UKA, fixed-bearing (FB) UKA still comprised 63.7% of knee arthroplasties in the Australian Registry 2 and 46.7% in the National Joint Registry in 2020. 1 It has consistently produced the longest survivorship according to the latest registries with revision rate of 3.6–4.8% in 5 years and 6.4–8.3% in 10 years.3,4 Several factors might have contributed to the gaining popularity of MB UKA; the first is the wider selection criteria which does not preclude patients with patellofemoral joint (PFJ) arthritis 5 ; the second is the use of non-navigated, non-robotic instrument 6 which could save time and cost; the third is the presence of robust clinical studies in MB UKA suggesting the benign nature of various postoperative conditions which could have affected survivorship such as tibial tray overhang, 7 periprosthetic radiolucency or radiosclerosis 8 and anteromedial knee pain. 9 On the other hand, the integrity of anterior cruciate ligament (ACL) is of larger concern in UKA and could be an advantage for FB UKA in terms of patient selection and survivorship.10,11 Recent studies suggest clinical outcome and survivorship in FB UKA are not affected by pre-existing PFJ arthritis12–15; this might help regain the popularity of FB UKA. More evidence seems necessary to consolidate the role of FB UKA in modern arthroplasty in terms of the three advantages of MB UKA mentioned above.
The aim of this study is to analyze the medium-term survivorship of a FB UKA with the use of a widened Kozinn and Scotts’ patient selection criteria 16 with no exclusion of early PFJ arthritis or ACL deficiency and the use conventional cutting guide (block-technique) without navigation or robotic assistance. The effect on survivorship by preoperative and postoperative factors including ACL integrity, PFJ arthritis, tibial tray overhang, periprosthetic radiolucency and anteromedial pain are analyzed. The clinical significance of anteromedial pain with respect to radiographic abnormalities is also investigated.
Materials and methods
This is a retrospective study. Patients with fixed-bearing medial compartment UKA (ZUK) performed in 2011-17 by the author as surgeon or supervisor were reviewed. Data retrieval was performed with CDARS (Clinical Data Analysis & Reporting System). ICD nine procedure code for retrieval was 81.54 “Unicondylar Knee Arthroplasty” or “Medial Condyle Knee Arthroplasty”. Clinical details were retrieved with CMS (Clinical Management System, Hospital Authority). Cases were selected for surgery according to Kozinn and Scotts criteria 16 with some modifications. Cases excluded for surgery were inflammatory arthritis, lateral compartment disease, flexion contracture >10°, range of motion <90°, uncorrectable varus deformity >15°, tibiofemoral subluxation >5 mm. There was no specific restriction on age, body weight, BMI and ACL integrity. Patients with anterior knee pain, or radiographic PFJ arthritis of Kellgren-Lawrence grading equal or less than two were not excluded for surgery.
Surgery was performed under tourniquet with minimal invasive quadriceps sparing technique using a medial parapatellar incision. Bone cuts were performed with extramedullary guide for tibia and femur (block-technique) using hand-held saw. Tibial cut was kept to minimal (2–4 mm) to preserve tibial bone stock but adequate to allow insertion of liner without excessive soft tissue tension. Small amount of coronal correction was achieved by using appropriate thickness of liner, aiming at restoration of cartilage and bone loss only. No ligament release was performed. No attempt was made to verify the integrity of ACL, PFJ and lateral compartment intraoperatively. Unicompartmental surgery was proceeded according to preoperative assessment. Prostheses used were either Miller-Galante (Zimmer, Warsaw, IN) or Unicompartmental High Flex Knee System (ZUK) (Zimmer, Warsaw, IN). All prostheses were cemented.
The primary outcome was implant survivorship in terms of revision for all causes. Reasons for revision were reviewed. Potential predictors for revision were analyzed. They included age, sex, BMI, perioperative alignment, preoperative PFJ arthritis, ACL integrity, tibial tray overhang, edge loading, radiosclerosis or radiolucency and anteromedial knee pain. Kellgren-Lawrence grading based on preoperative lateral and skyline view was used to assess PFJ arthritis. Preserved posterior joint space in the preoperative lateral radiograph was used as the surrogate for ACL integrity. Postoperative radiographic assessment was performed at 3, 6, 12 months and annually. The occurrence of postoperative periprosthetic radiosclerosis (Figure 1(a)–(c)) or radiolucency (Figure 2) was recorded. Subchondral sclerosis or cement void present immediately after surgery was not counted as significant radiological abnormalities. Tibial tray overhang was defined as extension of tibial tray 1 mm or more beyond anterior or medial tibial cortex (Figure 3). Edge loading was defined as incongruence between the medial lateral edges of femoral and tibial components as seen in the AP radiograph (Figure 4). (a) Anterior tibial tray overhang (1 month post-operation). (b) Same patient with radiosclerosis visible around tibial tray (6 months post-operation). (c) Tibial overhang now covered with new bone, radiosclerosis no longer visible (24 months post-operation). Non-progressive radiolucency beneath tibial tray. Medial tibial tray overhang. Edge loading.



The secondary outcome was the incidence of anteromedial knee pain after surgery. It was defined as occurrence or persistence of localized non-progressive anteromedial pain more than 3 months after surgery. The severity was graded as mild, moderate or severe. It was analyzed both for prediction of revision and for any association with radiographic abnormalities.
Data analysis was performed using the statistical software SPSS 20 (IBM, Armonk, NY). T-test was used to assess the difference in numerical outcome. Chi-square test was used to assess categorical outcome. Kaplan-Meier survival analysis was performed to estimate survivorship of UKA. Log-rank test was performed to assess potential predictors for survival. p-value of <0.05 was considered statistically significant.
Results
Basic parameters.
Outcome at 1 year.
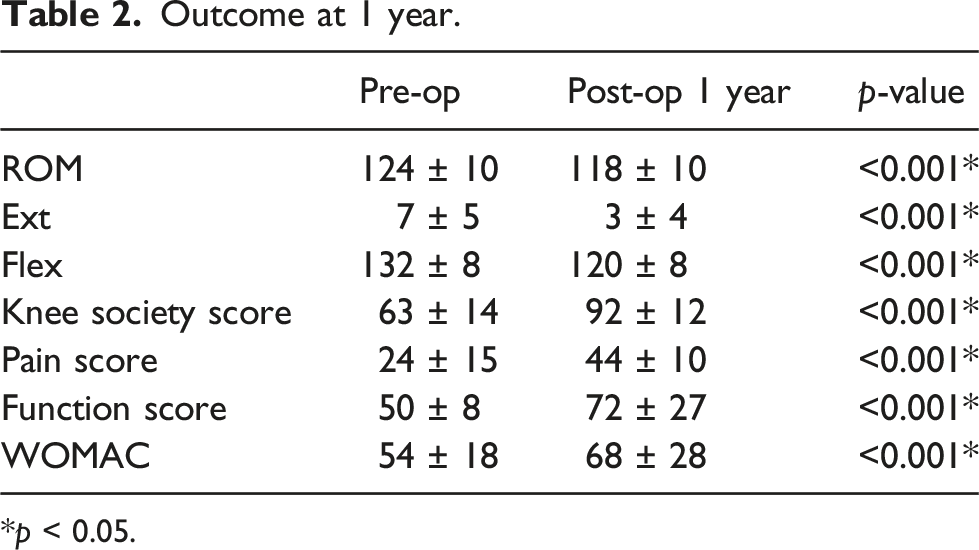
*p < 0.05.
Revision cases.

OA: Osteoarthritis.
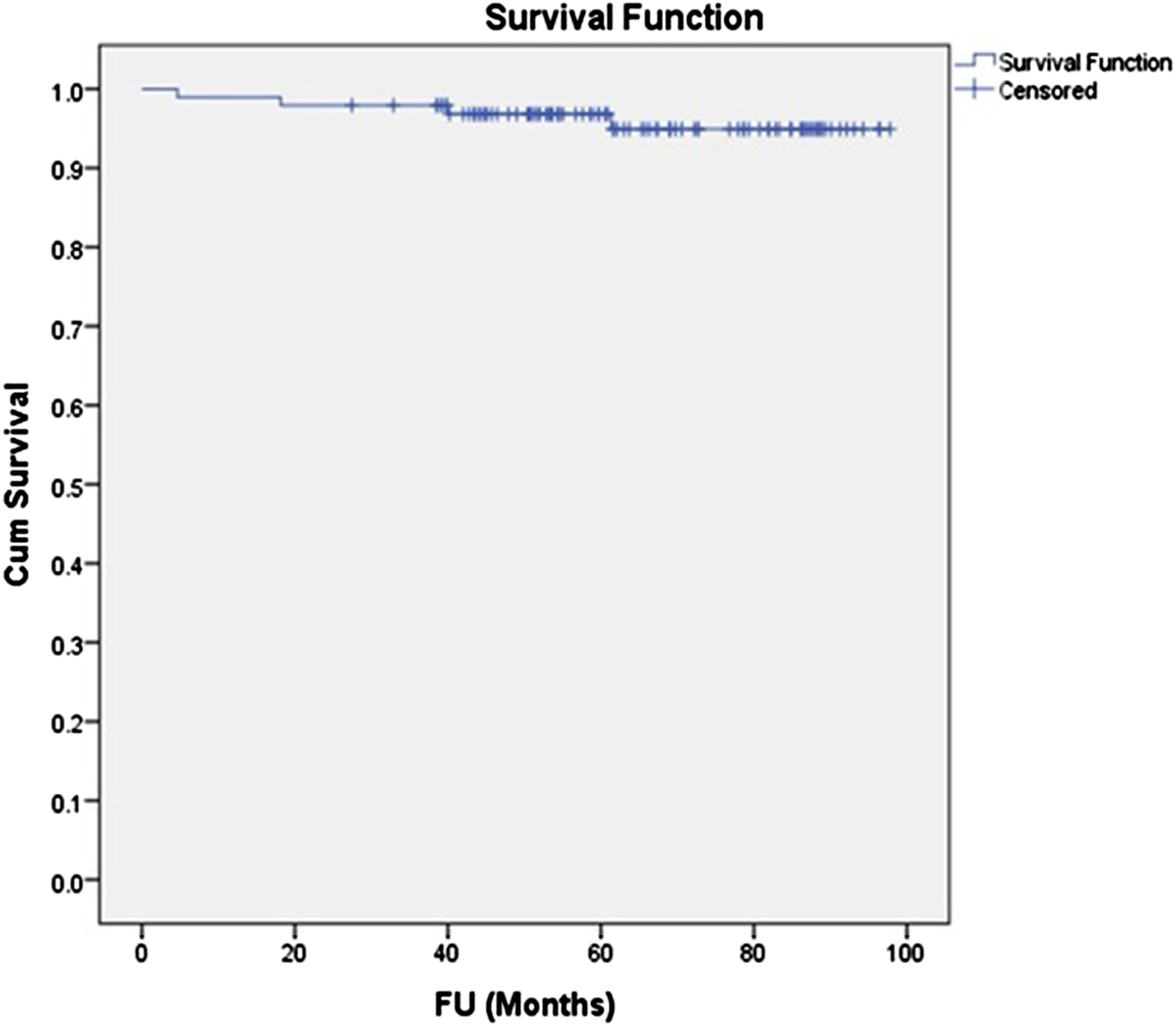
Kaplan Meier survival plot.
Potential predictors for survivorship.

*p < 0.05.
Anteromedial knee pain and radiographic abnormalities.

aFisher exact test.
Discussion
The results of the present study suggested a good medium term survivorship of FB UKA using a widened Kozinn and Scotts criteria with no exclusion of early PFJ arthritis or ACL deficiency. This was possible even in the context of non-navigated non-robotic surgery. The expected survivorship of 94.65% in 8.3 years using such criteria and surgical technique was comparable with latest registry data (91.7–93.6% in 10 years),1,2 large cohort study17,18 and metaanalysis.3,4 However, selection criteria were heterogeneous in registries and meta-analysis such that their survivorship results could not differentiate between those with different selection criteria. de Grave 17 reported the estimated survival of a 460 cohort to be 97.2% and 94.2% at 5 and 10 years but selection criteria excluded cases with pre-existing PFJ OA and clinical ACL deficiency. Gill 18 did not exclude patients with asymptomatic radiographic PFJ OA in a study on 466 FB UKA and found a medial implant survivorship of 97.9% at 10 years. However, the incidence of PFJ OA in the cohort was not reported.
In the present study, a comparable survivorship was seen in the presence of PFJ arthritis (Kellgren-Lawrence grading 1–2) in 75% and ACL deficiency in 5%. This has confirmed the recent evidences on wider patient selection criteria for FB UKA. Berger 13 compared survivorship from all-cause revision at 4 years for FB UKA with PFJ OA versus those without in 308 patients and showed no significant difference between two (98 vs 95%). 26% of his cases had patellofemoral OA of at least moderate severity (ICRS three or 4). Lim 15 reported 15.6% radiologically significant patellofemoral disease in a cohort of 263 FB UKA and found no difference in 10 years survival rate between those with or without PFJ OA (97.6% vs 94.6%). In the present study, despite a very high incidence (75%) of early PFJ OA in our cohort, survivorship was comparable with the latest published data and PFJ OA was not found to be a significant predictor for revision surgery.
The evidence of the effect of ACL deficiency on FB UKA is less. Engh and Ammeen 10 studied on 76 UKA with ACL deficiency and reported a similar 6 year survivorship to those without ACL deficiency (94 vs 93%). Suero et al. 11 found a 5 mm decrease of Lachmann test with 8° of tibial slope leveling. The finding suggested that the function of ACL could be partly compensated by the change in tibial slope. Echoing these findings, the presence of ACL deficiency in 5% of our cohort did not seem to affect the overall 8 years survivorship. None of the revised cases were ACL deficient.
While robotic assistance has been shown to improve survivorship in FB UKA, 2 majority of UKA are still performed with conventional cutting guide. Comparing with MB UKA, superior 15 years’ survivorship has been demonstrated in FB UKA even with conventional technique.3,4 There are other good reasons to stick to conventional technique. The first is higher cost and time associated with robotic surgery, second is the higher infection rate. 2 The cost-effectiveness of robotic assisted UKA in the context of higher risk of periprosthetic infection requires vigorous research before it will become a usual practice.
Other than PFJ OA and ACL deficiency, the clinical significance in terms of survivorship and knee pain of various radiological abnormalities has been studied in detail in MB UKA.7–9 This is less so in FB UKA. The present study suggested that they are not uncommon. There were 39% of tibial tray overhang, 14% of non-progressive radiolucency or radiosclerosis and 5% of edge loading respectively. They were neither associated with anteromedial knee pain, nor poorer survivorship. Goh et al. 19 reported 17% of female had medial tibial overhang of more than 2 mm, but the presence of overhang was not associated with poorer outcome or survivorship. Berger et al. 20 reported a rate of 49% of non-progressive radiolucency or radiosclerosis in FB UKA which was much lower than that reported for MB UKA of 75–96%.8,9 The present study showed an even lower incidence. Such low incidence of “physiological radiolucency” in other reports and FB designs has been attributed to the failure of taking radiographs tangential to the plane of the tibial plate. However, one may argue that the chance of missing these radiographic abnormalities at all time points is quite low and it is fair to believe that the rate of these non-progressive radiographic changes are design specific and might represent true difference between FB and MB UKA. Further studies on these different radiological abnormalities are required to explore in detail their specific clinical significance. As suggested by the present study, these radiological findings seem to be benign, as in the case of MB UKA.
Another finding of the present study was that non-progressive mild anteromedial knee pain is common after FB UKA (36.5%). The onset could be any time from 1 months after surgery and the mean duration of pain is around 1 year. This is similar to the finding in MB UKA by Gulati 9 which showed 54.1% of knee pain and 41.6% of mild pain after UKA. The present study did not look into the causes of pain but it was not associated with radiographic abnormalities or poorer implant survival. This echoed with the finding by Gulati that the pain was mostly transient and not related to implant survival.
Lastly, BMI ≥30 kg/m2 was found in the present study to be a significant predictor of poorer survivorship. This echoed with the finding by Xu et al. 21 who also reported an inferior survivorship at 10 years with BMI ≥30 kg/m2. In contrast, Venkatesh and Maheswaran 22 reported no difference in survivorship between high and low BMI at 5.6 years in metal-backed FB UKA; Cavaignac et al. 23 also reported no influence of BMI on 10 years survivorship in all-poly FB UKA. Similarly, Murray et al. 24 found no significant difference in 5 years survivorship in MB UKA for patients with different BMI. More data seems necessary before conclusion could be made on this issue.
There are several limitations in the present study. First, the number of subjects involved in the present study was small such that it might not be adequately powered to investigate the effect of different potential predictors on survivorship. However, our data may add to the pool of relevant studies such that future meta-analysis is possible. Second, although the mean follow-up time was 66 months, there was 40% of cases with follow-up time of less than 5 years. Third, the degree of overhang, radiolucency or edge loading might affect survivorship to various degree, which was not explored in the present study.
Conclusion
FB UKA based on a widened Kozinn and Scotts criteria with no exclusion of early PFJ arthritis or ACL deficiency using conventional cutting guide could produce satisfactory medium term survivorship. Patients with BMI ≥30 could have higher risk of all-cause revision. Tibial tray overhang, non-progressive radiolucency or radiosclerosis are not uncommon radiological findings but they seem not to be associated with anteromedial knee pain or poorer medium term survivorship.
Footnotes
Author contributions
QJ Lee analyzed, interpreted data and wrote up the manuscript; WY Chang charted scores and data; YC Wong contributed ideas in whole manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
Approval from IRB have been obtained for the study. (YCH REC). Consent from individual patient not required due to retrospective, blinded data collection with no sensitive items.
Consent for publication
The manuscript is not under consideration by another journal, and that it has not been previously published. In consideration of the Knee Surgery and Related Research reviewing and editing our submission, the authors convey all copyright ownership to the Knee Surgery and Related Research.
Availability of data and material
The data that support the findings of this study are available from but consent have not been obtained for sharing to public or third party.