
Abstract
Objectives
We developed a new standardized procedure for lateral unicompartmental knee arthroplasty (UKA) to maximize the benefits and minimize the risks of surgery in patients with osteoarthritis (OA).
Methods
This retrospective study recruited patients who underwent lateral UKA at our hospital between January 2014 and January 2016. Demographic characteristics and preoperative and postoperative American Knee Society (AKS) clinical scores (including pain, clinical, and knee mobility scores) were collected.
Results
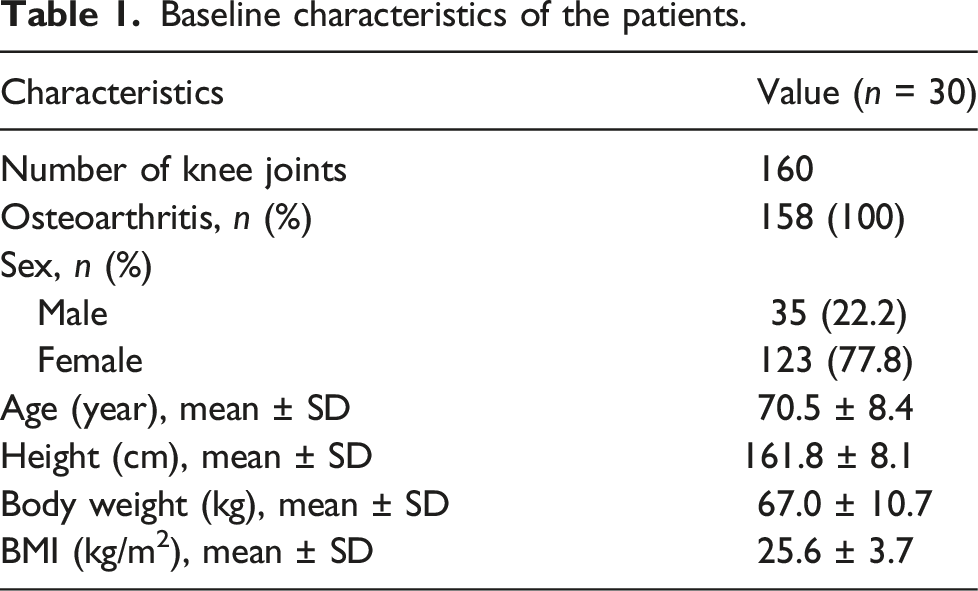
A total of 158 patients (35 male and 123 female) who underwent 160 lateral UKAs were analyzed. Their AKS clinical scores (0–100 points) improved from 53.1 ± 4.1 (range 45–62) preoperatively to 97.0 ± 1.7 (range 92–99) (p < 0.001) postoperatively with additional improvements of 9.1 ± 1.8 (range 3–14) to 47.3 ± 1.5 (range 45–49) (p < 0.001) for pain, 49.7 ± 9.7 (range 35–70) to 97.1 ± 4.1 (range 90–100) (p < 0.001) for function, and 105.0 ± 4.4° (equivalent to ∼100–115°) to 125.5 ± 5.3° (∼110–135°) (p < 0.001) for a range of motion (ROM). No patients required reoperations or revisions. Two patients were readmitted within 60 days due to severe knee swelling.
Conclusion
The lateral UKA protocol was reproducible and the patients had a good postoperative outcomes. Yet, large-scale, multi-center, prospective studies are needed to further confirm our findings.
Keywords
Introduction
Unicompartmental femorotibial osteoarthritis (OA) usually affects the medial compartment of the knee, but the lateral compartment is primarily involved in up to 10% of cases. 1 Unicondylar replacement for medial or lateral compartments began in the 1970s. For a patient with single-compartment OA, unicondylar arthroplasty offers faster recovery and better functional recovery than total knee arthroplasty (TKA).2,3 In addition, a significant amount of bone is preserved, making it possible to conduct a complete knee revision if later necessary.4,5 Historically, there was a high failure rate (up to 17%) for lateral unicompartmental knee arthroplasty (UKA) for the treatment of lateral compartment OA.6–10 Therefore, some surgeons believed that total knee arthroplasty was the only effective treatment for lateral compartment OA. 11
Nevertheless, technological innovations, including improvements in implant prostheses and tools, along with strict screening of patients, has enabled 10-years survival rates for prostheses to exceed 90% among patients undergoing lateral UKA.12–15 However, due to kinematic and anatomical differences, lateral unicompartmental replacement is technically more challenging and less reproducible than medial unicompartmental replacement .16–18 As such, lateral UKA is less widely practiced than medial UKA. 18
Despite the hesitance of surgeons to carry out lateral UKA, this procedure offers many benefits over TKA. As previously stated, lateral UKA is less invasive than TKA, with lower morbidity, bone loss, blood loss, and risk of infection. Moreover, it is reported that patients who underwent lateral UKA have a more natural gait than TKA due to the preservation of bone. 19 Despite a slightly higher revision rate than TKA, many consider lateral UKA to be a definitive procedure with comparable long-term results to TKA, while being more cost effective at less than half the price of TKA. 20
Herein, we developed a new standardized procedure for lateral UKA to maximize the benefits and minimize the risks of surgery in clinical work. Furthermore, we demonstrated that this procedure could be performed in a replicable manner to provide good outcomes.
Methods
Study design and patients
This retrospective study included patients who underwent lateral unicompartmental arthroplasties at the department of Joint Surgery of our hospital between January 2014 and January 2016. The Ethics Committee of our hospital authorized this study. All patients or their families gave informed written consent before surgery and provided consent to publish and report individual clinical data.
Inclusion criteria were: (1) painful isolated osteoarthritis and osteonecrosis; (2) significant loss of joint space in the lateral compartment on radiographs (Ahlbäck grade II or worse), (3) with intact medial compartment articular cartilage, and (4) valgus deformity had to be corrected by varus stress. Exclusion criteria were the following: (1) significant femoropatellar dysfunction such as a patellar subluxation or dislocation, (2) all forms of inflammatory arthritis were absolute contraindications for lateral UKA.
Standard preoperative evaluation
During the clinical examination of a lateral UKA knee joint, the surgeon evaluated the mobility and ROM of the joint. We required a flexion of 100° with normal extension. If the patient experienced pain in the front of the knee, then an assessment of the patellofemoral joint was required. The stability of the sagittal and coronal joints was carefully evaluated. Assessment of the anterior cruciate ligament (ACL) required prior notification. Assessment of knee joint pain and swelling axial displacement tests were limited. As previously mentioned, valgus deformation had to be assessed as correctable upon varus stress. 21
X-ray images were collected for the anteroposterior, lateral, Rosenberg, and stress-in-flexion views (varus and valgus-stress in flexion by hands of the examiner) of the knee for each patient. Internal and external stress-bearing X-rays were taken with the patient in a supine position, with the knee bent when varus and valgum stresses were applied by the intraoperative C-arm machine. This view was essential to assess cartilage loss in the medial compartment and if any present valgus deformity was correctable. In addition, lateral radiographs were used to assess whether displacement of the tibial plateau of the knee was >10 mm, and whether wear of the tibia was present in the front, middle or rear of the knee to assess the integrity of the ACL. A skyline radiograph was mainly used to confirm the lack of stenosis in the patellofemoral joint space. If the status of the ACL could not be determined by X-ray imaging, then magnetic resonance imaging (MRI) or arthroscopy was used to assess the ACL.
Standard operative procedure
A single senior surgeon conducted all procedures on each patient using an identical surgical technique. The procedure was performed through a lateral parapatellar approach. The intercondylar osteophytes were removed to prevent ACL damage. The small sulcus delineated the anterior border of the femoral component on the anterior part of the lateral condyle. For cases where it was difficult to locate the small sulcus, we also marked the front contact points of the lateral condyle and the tibial plateau, which are optimal anterior borders for the femoral component (Figures 1(a) and (b)). According to the lateral compartment’s anatomy, the tibial cut’s width was tested by a tibial prosthetic test tool, available in three sizes (45, 50 and 55 mm). The sagittal cut line was drawn by electrocautery between the medial border of the lateral femoral condyle and the lateral intercondylar eminence. The tibial guide was placed on the anterior edge of the tibia, 11 mm below the lateral condyle (Figure 1(C)). The 11 mm cutting height corresponds to the plateau (9 mm), plus a 2 mm laxity safety margin. The saw was internally rotated 15° relative to the vertical line of the front edge of the tibial guide to carry out a sagittal cut through the previously marked points (Figure 1(D)). The cortex of the anterior and posterior tibia was protected as much as possible so as to avoid posterior subsidence of the implant and prevent tibial fracture. As such, the reclining angle was generally set according to the tibial guide (normally between 0 and 3°). Some surgical teams recommend vertical tibial resection through the patellar tendon split. However, we preferred tendon retraction. During the operation, we observed the impact of the femoral condyle and intercondylar eminence caused by a drop in the joint line due to the tibial cut (Figure 1(E)). Surgical procedure. (a, b) The width of the tibial cut are tested using a tibial prosthetic test tool, sagittal cut line is drawn with the electrocautery between the medial border of the lateral femoral condyle and the lateral intercondylar spine; (c, d) The tibial cutting guide is placed so that its upper edge is flush with the marked point on the front lower side of the tibial plateau. The saw blade is internally rotated 15° relative to the vertical line of the front edge of the tibial cutting guide and is used to cut vertically through the previously marked points. Horizontal cut can be performed; (e) During the operation, observe the impact of the femoral condyle and the intercondylar spine caused by the drop of the joint line after cut of the tibia; (f, g) The parallel lines on the parallel tibial test model are used for cut to remove the hardened subchondral bone; (h) The midline of the femoral prosthesis was consistent with that of the tibial plateau prosthesis, first marked on the femoral condyle with an electric knife; (i–k) The femoral test model and special limit device are used for the drilling test. Drilling must be done by aligning the midline of the femoral model with the marking line on the femoral condyle, drilling at approximately 30° to the posterior cortex of the femur; (l) The lateral compartment flexes 90°. The joint clearance should be about 2 mm larger than the knee extension clearance.
After the tibial cut, appropriate sizes for the test models (LINK Orthopaedics China Co, Ltd, Beijing, China) were selected according to the tibial plateau test results. The appropriate test models were then placed into the lateral space to restore normal alignment of the knee joint. Next, we conducted a cut parallel to the marked line on the tibia test model and removed the subchondral bone to avoid the valgus and varus during the femoral cut (Figures 1(F) and (G)). The midline of the femoral condyle prosthesis was the femoral condyle that corresponds to the midline marking line on the tibial plateau test model (Figure 1(H)). First, the femoral condyle was marked using an electric knife. The tibial test model was removed and the hip and knee joint were extremely flexed. A femoral drilling test model and special limit device were used for drilling tests to ensure that the midline of the femoral model coincided with the marker line on the femoral condyle; The drill was carefully placed at about 30° to the posterior cortex of the femur to avoid an overly large femoral prosthesis (Figures 1(i) to (K)). We used a cut depth of 1–2 mm below the cartilage to avoid a step between the femoral prosthesis and the patella. Consequently, a femur drilling guide was precisely positioned to avoid internal or outer rotations, prevent impingement to the tibial spine eminence in extension, and minimize contact with the patella. Once the femoral condyle cut was completed, the test model was removed. We removed osteophytes from the posterior femoral condyle and soft tissues occupying the posterior space to improve knee flexion and prevent the impact of the polyethylene prosthesis in high-flexion positions. After placing the prosthesis, the knee was bent at 45° and placed a 2-mm insert into the gap. The insert was removed after the bone cement dried. The joint space of the lateral compartment was about 2 mm larger than the straight clearance when flexing the knee at 90° (Figure 1(L)). The sizes of prosthesis used in this case were: the femur 46, the tibia (width, thickness) 50 mm, 9 mm. Preoperative and postoperative x-rays are detailed in Figure 2. (a, b) Preoperative frontal and lateral radiographs showing lateral femorotibial osteoarthritis. (c, d) Postoperative frontal and lateral radiographs show good prosthesis position.
Our methods have several advantages, which help to avoid the collision of the femoral prosthesis with the tibial intercondylar spine during the knee extension. When bending the knee, the femoral prosthesis should be rotated laterally. 22 The results of our study suggest that the midline of the femoral prosthesis should be aligned with tibial prosthesis’s midline to prevent internal and external rotation of the femoral prosthesis and ensure that the femoral prosthesis is placed outside the femoral condyle.
The femoral prosthesis drill limit device we designed can simplify the operation. It is designed with a slot in the midline of the tibial prosthesis, the size of which matches the protrusion in the midline of the femoral drilling test model. When the knee is bent at 90°, the median surfaces of the femoral and tibial prosthesis are aligned with each other. Intraoperative observations have shown that impact forces between the medial edge of the lateral femoral condyle and the tibial intercondylar spine only occur in patients with narrow lateral compartments, and after the height of the lateral articular surface is restored during the operation, the impact forces disappear. 23 Therefore, our method can effectively avoid impact forces and further joint damage by restoring the joint line. In addition, the width of the normal intercondylar concave is sufficient to prevent impact between the femoral condyle and the tibial intercondylar spine during locking.
Data collection
Patients’ demographic characteristics, preoperative and postoperative AKS functional scores (including pain, clinical, and knee mobility scores) data were collected. Postoperative AKS functional scores were collected at 6 weeks, 3 months, half a year, 1 year, 2 years, and 3 years post-operation, and the last scores were used for this statistical analysis.
Statistical analysis
The statistical analyses were performed using SPSS 22.0 (IBM, Armonk, NY, USA). Quantitative data are presented as the mean ± standard deviation with the paired t-test used for comparison. Qualitative data are presented as n (%). p < 0.01 was considered statistically significant.
Results
Baseline characteristics of the patients
Baseline characteristics of the patients.
Postoperative outcomes
American knee society scores and activity results before and after operation.

Data were expressed as means ± standard deviations.
Discussion
Our retrospective analysis indicates that the described standardized procedure for lateral unicompartmental knee arthroplasty (UKA) is a safe and effective treatment for lateral unicompartmental osteoarthritis (OA). Postoperative American Knee Society (AKS) clinical scores were significantly improved compared to preoperative values, with a postoperative reduction in knee pain and increased range of motion (ROM).
The dislocation rate of the lateral mobile gasket for UKA was reported to be 10%, with a 5-years prosthesis failure rate of 21%. 24 Indeed, femoral rollback during knee flexion is important for lateral knee compartment functioning, which can lead to the observed early failure of UKA using mobile gaskets. Others report that as long as patients were screened appropriately, lateral UKA achieved good clinical outcomes. 22
Recent reports further suggest that patient selection for lateral UKA prosthesis is essential for prosthesis survival.25,26 None of the cases in our study have been reoperated, in accordance with Smith et al, 27 in which the short- and mid-term clinical effects of lateral UKA were satisfactory. However, some suggest that patient selection is more important when surgeons are facing a high caseload, and as such selection criteria may be surgeon dependent. 25
A retrospective study by Ernstbrunner et al 28 reported that the main causes of lateral UKA failure included OA progression (30%) and aseptic loosening (22%), followed by instability (7%), unexplained pain (5%), infection (5%), polyethylene gasket wear (5%) and gasket dislocation (5%). Gasket dislocation was the most common cause of early failure (29%) and the most common cause of overall failure (27%) for patients with a mobile gasket prosthesis. Among the mid- and late-stage failure cases, OA progression led to the highest failure rates (59% and 78%, respectively).
In order to avoid complications, our study provides evidence for these guidelines: (1) strict compliance with the above surgical indications to screen patients, avoiding possible complications caused by improper indications; (2) use of a fixed gasket prosthesis, thus effectively avoiding the occurrence of gasket dislocation; (3) overcorrection should be avoided; and (4) use of standardized surgical methods to reliably replicate the operation between patients, thus ensuring reliable and consistently positive postoperative outcomes.
Although the effectiveness of our surgical technique was demonstrated in this article with the LINK prosthesis, it could be applicable to other fixed-platform prostheses. For example, for determining the width of the tibial prosthesis, for determining the anterior edge of the femoral prosthesis, for aligning the femoral prosthesis with the midline of the tibial prosthesis, and for making the joint gap 2 mm wider at 90° of knee flexion than an extension.
The present study has a few limitations. This is a single-center retrospective study with a small sample size and relatively short follow-up time. Also, we applied a less widely practiced surgical method in this study. Nevertheless, short-term follow-up showed good results.
Conclusion
The lateral UKA protocol was reproducible, and the patient had a good postoperative outcome. However, large-scale, multi-center, prospective studies are needed to further confirm our outcomes.
Abbreviations
anterior cruciate ligament
magnetic resonance imaging
osteoarthritis
patellofemoral joint
unicompartmental knee arthroplasty
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Science and Technology Commission of Shanghai Municipality (21Y11911600).
Ethical approval
This study was performed in accordance with the Declaration of Helsinki as revised in 2008 and was authorized by the Ethics Committee of our hospital. All patients or their families signed the informed consent form before surgery and provided consent to publish and report individual clinical data.