
Abstract
Purpose
This study aimed to confirm the usefulness of surgery that avoids the cervicothoracic junction (CTJ) by comparing the clinical and radiographic outcomes after posterior cervical fusion at C5/6 with those at C7/T1.
Methods
Patients who underwent laminectomy and posterior cervical instrument fusion for cervical spondylotic myelopathy (CSM) from 2012 to 2019 were retrospectively reviewed and divided according to whether the end level was at C5/6 (group 1) or C7/T1 (group 2). Demographic variables and incidence of distal junctional kyphosis (DJK) were compared between the groups. Clinical outcomes (visual analog scale [VAS] score for arm and neck pain and the Neck Disability Index value) and radiologic outcomes (T1 slope, cervical lordosis, segmental lordosis, C2-7 sagittal vertical axis, T1 slope-cervical lordosis mismatch) were compared over time.
Results
Sixty-seven patients were included. There were 32 patients in group 1 and 35 in group 2. The VAS score for neck pain was significantly lower in group 1 than in group 2 at 2 years after surgery (p = 0.03). The C2-7 sagittal vertical axis was significantly larger in group 2 than in group 1 at 1 year and 2 years postoperatively (p = 0.04). The incidence of DJK was higher in group 2 than in group 1 (28.57% vs 9.37%, p = 0.04).
Conclusion
This study found that when CTJs are included in the posterior cervical long fusion surgery, although it would be better than preoperation, postoperative kyphosis and consequent neck pain may progress. The results of this study advocate the concept of avoiding CTJ fusion if possible.
Brief introduction
In the aging society, the number of patients with degenerative cervical disease has increased rapidly in recent decades.1,2 A considerable number of patients with cervical spondylotic myelopathy (CSM) are undergoing posterior cervical decompression and fusion.3,4 The cervicothoracic junction (CTJ) is often included in multilevel posterior cervical fusion surgery. The CTJ has several unique biomechanical and structural properties. The cervical spine maintains lordosis, whereas the thoracic spine maintains kyphosis. The cervical spine has greater mobility in flexion, extension, and lateral bendings than the thoracic spine due to articulation of the ribs and bony ligament structures of the thoracic spine.5–7 This non-physiological load may increase the risk of implant failure or disc degeneration at adjacent levels. Previous studies have aimed at guiding the surgeon through extension to the upper thoracic vertebrae in selecting the most appropriate caudal level of fusion but have not yielded definitive results.8–11 Recommendations for a caudal “end level” in posterior cervical fusion surgery vary, and few studies have investigated the benefits of routinely avoiding “extension” to the CTJ in posterior cervical fusion surgery. This study compared the clinical and radiologic outcomes of fusion ending at C5/6 and fusion extending to C7/T1 to determine the effect of avoiding the CTJ by fusion of only the cervical spine, unlike the existing method of extending fusion to the upper thoracic spine.
Materials and methods
This study was approved by the Institutional Review Board of our institution.
Study population
We retrospectively reviewed a series of patients with degenerative CSM (age ≥18 years) who underwent laminectomy and posterior cervical instrument fusion at a single surgeon and center between January 2012 and February 2018. The inclusion criteria were multilevel (≥3) posterior cervical fusion without adding a C1 screw or occipital plate and screw fixation below T2. Patients with trauma, tumors, infection, or prior cervical spinal surgery were excluded, as were those who had undergone non-fusion surgery, such as unilateral or bilateral open-door laminoplasty, posterior lamina decompression, posterior laminectomy, discectomy, and those who had been followed up for less than 24 months. In addition, patients with ossification of posterior longitudinal ligament, whose alignment change after posterior fusion surgery would not be distinct, were excluded.
Patients were divided into groups according to whether fusion surgery ended at C5/6 (group 1) or C7/T1 (thereby including the CTJ, group 2). We decided on the lower instrumented level according to the presence of stenosis. We decided to include CTJ when there were C6-7-T1 lesions, such as myelopathy, severe stenosis, or severe arthropathy with or without cord signal change.
Differences in demographic and clinical variables, including age, sex, smoking history, body mass index, hypertension, bone mineral density (T-score), and diabetes, were compared between the two groups. The number of fusion levels was also compared between the groups.
Clinical outcomes
All patients were assessed preoperatively, immediately after surgery, and 24 months postoperatively. Clinical outcomes were evaluated using a visual analog scale (VAS) for neck and arm pain and the neck disability index (NDI). We also assessed pain intensity and its impact on disability and quality of life using VAS scores and responses to NDI and satisfaction with treatment questionnaires. When patients had difficulty completing a written questionnaire, the clinical outcomes were investigated by telephone.
Surgical procedure
A freehand cervical pedicle screw (CPS) fixation technique was performed in all patients. The safety and efficacy of CPS placement have been validated previously.12–16 The CPS fixation technique was performed as follows. First, Computed tomography (CT) was performed along with preoperative spinal angiography in all patients. CPS insertion using the freehand technique was considered when the pedicle diameter was >3.0 mm on the axial CT image, and there was no vertebral artery malformation.
17
The entry point of the screw was determined at the level of the notch in the sagittal plane and medially at the outer border of the superior process by 1/4 of the width in the axial plane. A small pilot hole was made with a 1.8 mm diameter match head type burr at a predetermined entry point. Screw diameter and length were based on preoperative measurements of axial CT images. Vertex pedicle screw system (Medtronic Sofamor Danek, Memphis, TN) used diameters ranging from 3.5 to 4.0 mm. A more detailed technical description of this technique has been previously published.12,13,17,18 Although cervical pedicle screw placement using a freehand technique was considered, there were some cases of lateral mass screw fixation conversions or screw skipping.19,20 Decompressive laminectomy was done en bloc, and posterolateral fusion was done with local bone chips after exposing cancellous bone on the lateral mass (Figure 1).
21
Intraoperative photo of (a) posterior cervical pedicle screw insertion and (b) decompression laminectomy with lateral fusion using local bone chips after exposing cancellous bone on the lateral mass.
Following screw insertion and decompression, the position of the patient’s head was extended using remote-controlled table head segments. Correct screw positioning and lordotic cervical alignment were confirmed on portable anteroposterior and lateral radiographs. 22
Radiologic evaluation
Radiographic measurements were obtained using lateral cervical radiographs before surgery, immediately after surgery, and 3 months, 1 and 2 years postoperatively. Cervical lordosis (CL), C2-7 sagittal vertical axis (SVA), T1 slope, segmental lordosis (SL), and T1-CL mismatch were measured. CL was defined as the sagittal Cobb angle between the C2 and C7 vertebrae. The T1 slope was defined as the angle at which the line tangential to the upper end plate of T1 and the horizontal reference line intersect. C2-C7 SVA was defined as the distance between C2 and C7. SL was defined as the angle between the cranial and caudal endplates of the upper and lower vertebrae in the affected segment (Figure 2). Measurement of cervical parameters on standard lateral cervical radiographs. Abbreviations: CL, C2 to C7 cervical lordosis (C2-7); SL, segment lordosis; SVA, sagittal vertical axis.
The incidence of distal junctional kyphosis (DJK) between the two groups was also investigated. DJK was defined as a change in angle of −10° or less at the distal disc level from the end of the fusion construct between baseline and final follow-up. 23
Statistical analysis
Continuous variables were described as mean ± standard deviation, and categorical variables were expressed as frequencies or percentages. Additionally, Student’s t-tests, chi-square test, and Fisher’s exact tests were used to confirm the statistical significance of differences in radiological and clinical outcomes. All statistical analyses were performed using SPSS Statistics for Windows, Version 17.0 (IBM Corp., Armonk, NY, USA). A p-value <0.05 was considered statistically significant.
Results
Demographic characteristics
Patient demographics in each study group.

DJK, distal junctional kyphosis; SD, standard deviation.
Clinical outcomes
Clinical outcome for each period in both study groups.

NDI, Neck Disability Index; VAS, visual analog scale.
Radiologic outcomes
Comparison of radiologic parameters between the two groups.
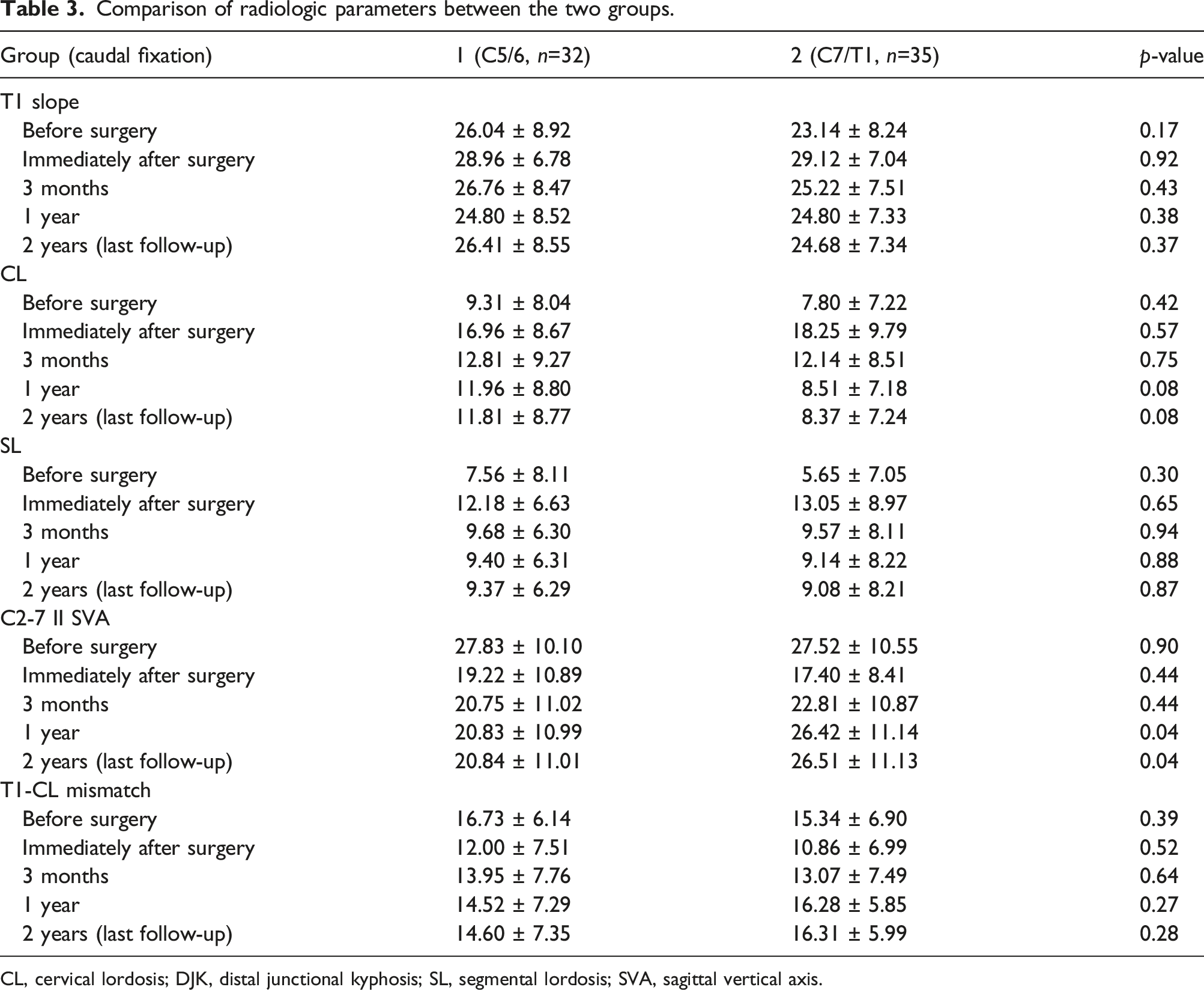
CL, cervical lordosis; DJK, distal junctional kyphosis; SL, segmental lordosis; SVA, sagittal vertical axis.

Continuous graphs showing the C2-7 SVA (mm) in each group before surgery, immediately after surgery, and 3, 12, and 24 months after surgery. Abbreviations: SVA, sagittal vertical axis.
Illustrative case
A 74-year-old woman presented with weakness and pain in her left arm; she had weak left elbow flexion/extension (2/5) and hand grip (3/5). Preoperative MRI showed severe spinal canal stenosis and spinal cord compression in C3-7 with myelopathy. The patient underwent posterior fusion and decompression at C3-7. Immediately after surgery, the weakness and pain in the left upper extremity improved. However, 15 months after the operation, she came to the hospital with progressively increasing posterior cervical pain (VSA 0 → 3), and distal junctional kyphosis was observed during the examination (Figure 4). Case. A 74-year-old woman confirmed that C7-T1 distal junctional kyphosis developed comparing (a) immediately after surgery and (b) at the final follow-up.
Discussion
Although laminectomy and multilevel fusion are standard CSM techniques, there is still debate about whether or not to connect the CTJ to reduce or avoid complications. In long instrument vertebral fusion surgery of the thoracolumbar spine, some studies recommend extending the highest instrumented vertebra to the level of the upper thoracic vertebra or at least T10 or higher to avoid proximal junctional kyphosis.24,25 Similarly, to solve the problem of the CTJ, several studies9,26 have recommended bridging the CTJ, but there were also contradicting reports.27,28
Therefore, we considered a method to terminate fusion above the CTJ in multilevel cervical fusion and compared the postoperative cervical parameters and clinical outcomes between patients whose fusion was completed at C5/6 and those whose fusion was completed at CTJ.
Radiographs showed that the C2-7 SVA was increased 1 year after surgery in group 2, including the fusion of the CTJ. This finding confirmed that kyphosis was greater after surgery involving the CTJ. The CTJ presents a challenging biomechanical environment because it is where the lordotic and mobile cervical vertebrae transition into a kyphotic and relatively immobile ribbed thoracic vertebra. 9 Therefore, there are significantly greater flexion and translational forces in this area of the spine than at other levels, and these vulnerabilities are exaggerated after surgery.29,30
A higher incidence of DJK was observed when fusion ended at CTJ compared to when it was extended to the C5/6 level (28.5% vs 9.3%). This study confirmed that the involvement of C7 affects the progression of DJK after cervical fusion and found that muscle degeneration at the C7 level affects cervical kyphosis and balance, as noted in the Tamai et al. 31 study. The thoracolumbar junction also shows a relationship between the muscles of the thoracolumbar region and PJK. 32 Furthermore, the CTJ is subjected to unique biomechanical stresses, and postoperative instability in this region is thought to be caused by DJK. 30
Regarding clinical outcomes, the VAS score for neck pain was significantly higher in group 2. Riew et al. 33 mentioned that muscle attachment and the spinous processes at C7 are postoperatively associated with increased neck pain. Moreover, it is thought that the occurrence of DJK may affect the clinical outcome. The incidence of DJK was high in group 2, and Passias et al. 23 reported an association between neurological symptoms and DJK.
In this study, DJK and kyphosis occurred because of the destruction of the unique mechanical structure and muscle degeneration at the CTJ after the extension of fusion to C7/T1, which is thought to exacerbate postoperative neck pain (Figure 5). Process of kyphosis and clinical complications in patients who underwent posterior cervical fusion that included the CTJ. Abbreviations: DJK, distal junctional kyphosis; CTJ, cervicothoracic junction.
Some studies10,34,35 have shown that crossing the CTJ prevents kyphotic collapse, ongoing neck pain, and symptomatic adjacent segment degeneration. According to the results of this study, CTJ should be avoided if possible; if CTJ must be included, fusion extension up to T2-4 can be considered.
This study had two major limitations. First, it contained a small number of patients, including only five and two patients in the C5 and T1 lower instrumented vertebra. Second, this study was performed retrospectively.
Conclusion
This study confirms that when CTJs are included in the posterior cervical long fusion surgery, although it would be better than preoperation, postoperative kyphosis and consequent neck pain might progress. The findings of this study support the concept of avoiding CTJ fusion as much as possible. Surgeons should remember that CTJ stop in the posterior cervical long fusion surgery can accelerate the degeneration of distal uninstrumented level during long-term follow-up.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB approval
The Institutional Review Board of Asan Medical Center (IRB No. GNAH 2021-11-009).