
Abstract
Background
One in five patients with mechanical alignment (MA) after total knee arthroplasty (TKA) was reportedly dissatisfied. As constitutional varus knees are common, restoring the patients’ natural residual varus (RV) alignment is as an appealing alternative to neutral MA. This meta-analysis aimed to evaluate the effects of RV alignment on the functional outcomes compared with those of MA in TKA for the knees with varus osteoarthritis.
Methods
The MEDLINE/PubMed, Cochrane Library, and EMBASE databases were comprehensively searched for papers comparing the effects of RV alignment and MA on the functional outcomes from the time of inception of the databases to July 2020. Studies comparing the functional outcomes in the knees subjected to TKA with RV alignment (case group) and MA (control group) were included. The Knee Society knee and functional scores (KSKS and KSFS, respectively), Western Ontario and McMaster University Osteoarthritis Index (WOMAC), Oxford knee score (OKS), and forgotten joint score (FJS) were compared.
Results
Seven studies were finally included; all studies showed a low risk of selection bias and provided detailed demographic data. The pooled mean difference in the KSKS (0.06, 95% confidence interval [CI]: −0.14 to 0.27; p = 0.55) and KSFS (0.08, 95% CI: −0.08 to 0.35; p = 0.56) between RV alignment and MA did not significantly differ. The pooled mean differences in the WOMAC (−0.25, 95% CI: −0.57 to 0.07; p = 0.12), OKS (0.06, 95% CI: −0.15 to 0.27; p = 0.56), and FJS (0.41, 95% CI: −0.18 to 1.00; p = 0.18) between the groups were not significant.
Conclusion
The beneficial effects of RV alignment on the functional outcomes are limited compared to those of MA in TKA for varus osteoarthritis to date. Currently, TKA with neutral MA should be considered as the gold standard.
Introduction
Total knee arthroplasty (TKA) has been widely established as a successful treatment for advanced osteoarthritis of the knee joint in terms of pain relief and functional improvement.1–3 An immense burden on health care systems is predicted with the increased volume of primary and revision TKA.2–4
Neutral mechanical alignment (MA) is a long-held tenet in TKA, as a stable and neutrally aligned knee evenly distributes the compartment constraints and guarantees long-term prosthesis survival.5–7 However, approximately one in five patients with TKA was reportedly still dissatisfied. 8 Furthermore, the reduction in outliers from MA after advancements in computer navigation has not led to improvements in the clinical and functional outcomes after TKA. 9
Evidences demonstrated that constitutional varus knees (≥3° varus alignment of the mechanical femorotibial angle [FTA]) are more common than previously thought.10–12 Systematically achieving MA may affect the normal anatomy and gait biomechanics of multiple joints including knee, ankle and subtalar joints especially in patients with constitutional varus knees.10–16 Therefore, restoring the patients’ natural residual varus (RV) alignment has been proposed as an appealing solution of patients’ dissatisfaction following TKA with neutral MA.
Leaving RV alignment is associated with the advantages of avoiding the excessive medial soft tissue release and restoration of the constitutional knee anatomy; consequently can contribute to the feeling of a natural joint.10,17,18 However, there are controversies regarding the effects of leaving varus alignment on the functional outcomes and quality of life.19–21 Randomized controlled studies or large-scale cohort studies have not been published to date. It is still questionable whether leaving RV alignment can improve the clinical outcomes of TKA. To the best of our knowledge, previous meta-analyses have not investigated the evidence supporting the effect of RV alignment in TKA. Therefore, this meta-analysis aimed to evaluate the effect of RV alignment by comparing the functional outcomes reported in studies that directly compared MA TKA and TKA with RV alignment.
Materials and methods
This meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. 22 Patient consent and ethical approval were not required since this study is a meta-analysis based on studies published. Two independent reviewer authors performed the literature search, inclusion, data extraction, and quality assessment. Disagreements were resolved by consensus with a third reviewer.
Search strategy
The following databases were searched in 3 August 2020 to obtain all relevant articles: MEDLINE/PubMed (1950‒July 2020), Cochrane Library (July 2020 Issue 7), and EMBASE (1974‒July 2020). The following keywords, Medical Subject Headings (MeSH) terms and their combinations were searched in the [Title/Abstract] field of the search engines: “total knee replacement” OR “total knee arthroplasty” OR “arthroplasty, replacement, knee” [MeSH term] AND “remain” OR “remaining” OR “remnant” OR “remained” OR “residual” OR “residue” OR “leaving” OR “left” OR “leave” OR “allowing” OR “allowance” OR “allow” OR “accepting” OR “acceptance” OR “accept” OR “under-correction” OR “undercorrection” OR “under-correct” OR “undercorrect” OR “under-corrected” OR “undercorrected” OR “natural” OR “constitutional” OR “native” OR “nature” AND “varus” OR “varus-type.” No other restrictions were applied, including language restrictions. The references of included articles were manually reviewed to identify additional eligible articles.
Eligibility criteria and study selection
The articles were reviewed by two independent reviewers. During the first stage of screening, duplicated publications were removed and the reviewers manually checked all the relevant articles based on the title and abstract. The full text of the articles was reviewed in the second stage of the screening process to select articles that met the inclusion criteria. The inclusion criteria were, as follows: (i) studies including knees with preoperative varus lower-limb alignment, (ii) case–control analyses comparing MA (−3° ≤ FTA ≤ 3°; positive values indicated a varus alignment, whereas negative values indicated a valgus alignment) and RV alignment (3° < FTA) during TKA, and (iii) studies reporting the clinical outcomes comparable to those of other studies. The exclusion criteria were as follows: (i) non-original research (e.g. review article, technical notes and survey articles), (ii) case-series studies and (iii) studies not eligible for the inclusion criteria following the second stage of the screening process.
Data extraction
The data were extracted according to the following descriptive information provided in the included trials: (i) study characteristics, such as author names, year of publication, study design, level of evidence, and journal; (ii) patient demographic characteristics, such as number of cases, average age, and sex; (iii) mean follow-up period; (iv) composition of the case and control groups; and (v) outcome measures of interest. The outcomes of interest were the following functional outcomes: Knee Society knee and functional scores (KSKS and KSFS, respectively), Western Ontario and McMaster University Osteoarthritis Index (WOMAC), Oxford knee score (OKS), and forgotten joint score (FJS). 23
Quality assessment
The methodological quality of the case–control studies was assessed using the Newcastle–Ottawa assessment scale, which comprises three main domains (selection, comparability, and outcome), with four categories in the selection domain, one category in the comparability domain, and three categories in the outcome domain.24,25 A study was awarded a maximum of one star for each item in the selection and outcome domains. A maximum of two stars was assigned for comparability.
Statistical analysis
All data from the included studies were extracted into an Excel spreadsheet (Microsoft Corporation, Redmond, WA). The clinical outcomes were statistically compared between the case and control groups using R version 3.1.1 (The R Foundation for Statistical Computing). A p-value of <0.05 was the threshold for statistical significance. In the case of a comparative study on knees with various overall alignments, such as mild varus (3° < FTA ≤ 6°) or severe varus (6° < FTA) alignment, data other than those for mild varus alignment were discarded.
The data needed to be standardized for analyzing the intergroup comparisons of the outcomes because the materials and methods used in the included studies were heterogeneous. The standardized mean difference (SMD) was defined as the difference in the mean outcomes divided by the standard deviation of the difference in the outcome. The SMD and associated 95% confidence intervals (CIs) were determined for patient-reported outcomes. The I2 statistic was calculated to present the percentage of total variation attributable to the heterogeneity among the included studies. The random-effects model was used because most studies were heterogeneous and described several uncontrolled variables. 26 Forest plots were used to graphically present the results of individual studies and the respective pooled estimate of the effect size.
Results
Study selection
Electronic searches of the PubMed (MEDLINE), EMBASE, and Cochrane Library databases yielded 398, 441, and 44 studies, respectively. Two additional publications were identified through manual searching. After removing 449 duplicated studies, we obtained 436 studies. Of these, 394 were further excluded after reading the abstracts and full-text articles. An additional 35 studies were excluded owing to unusable information and inappropriate group comparisons. After applying these criteria, seven studies were finally included in the meta-analysis20,21,27–31 (Figure 1). PRISMA flow chart. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analyses.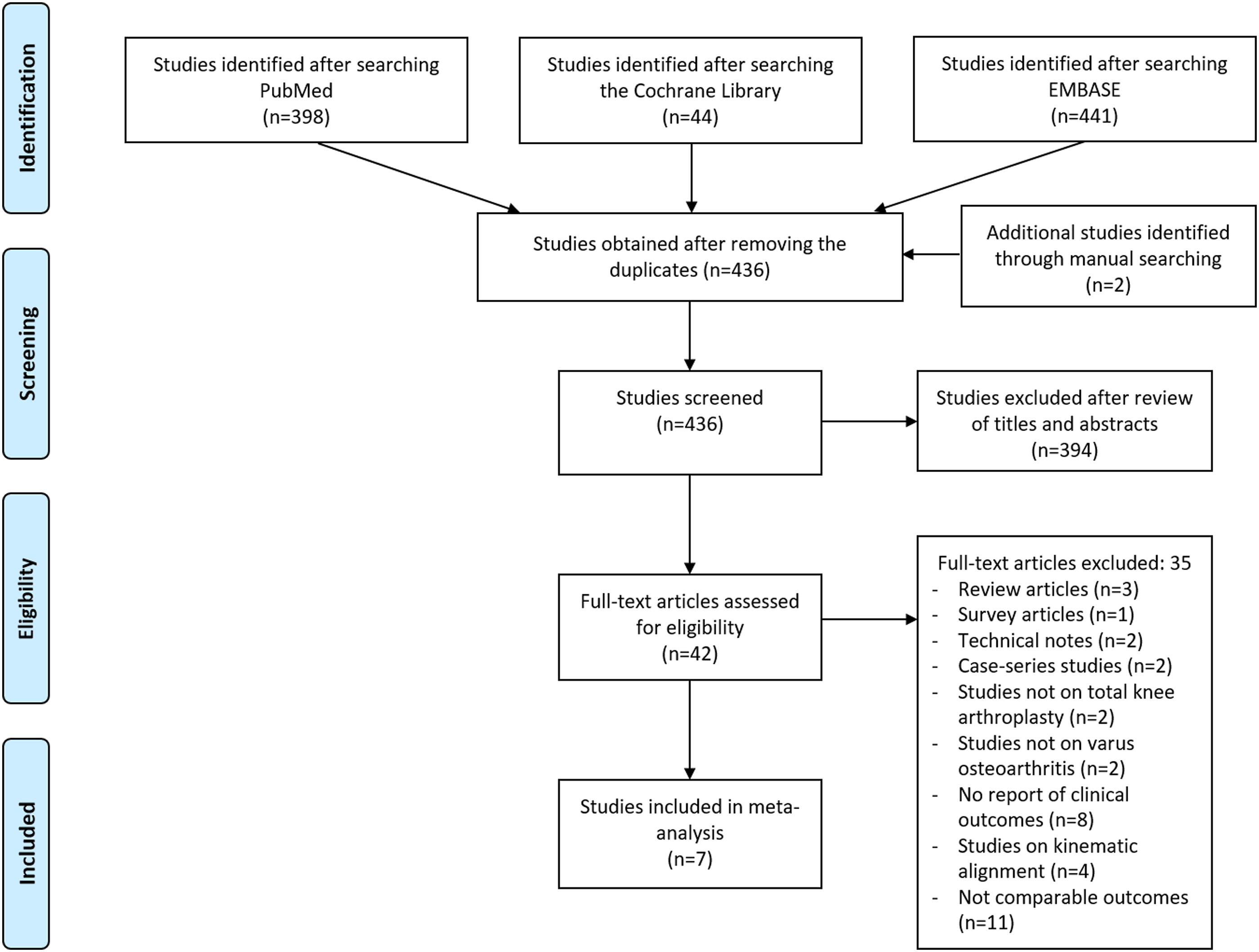
Study characteristics and quality assessment
Baseline characteristics of the included studies.
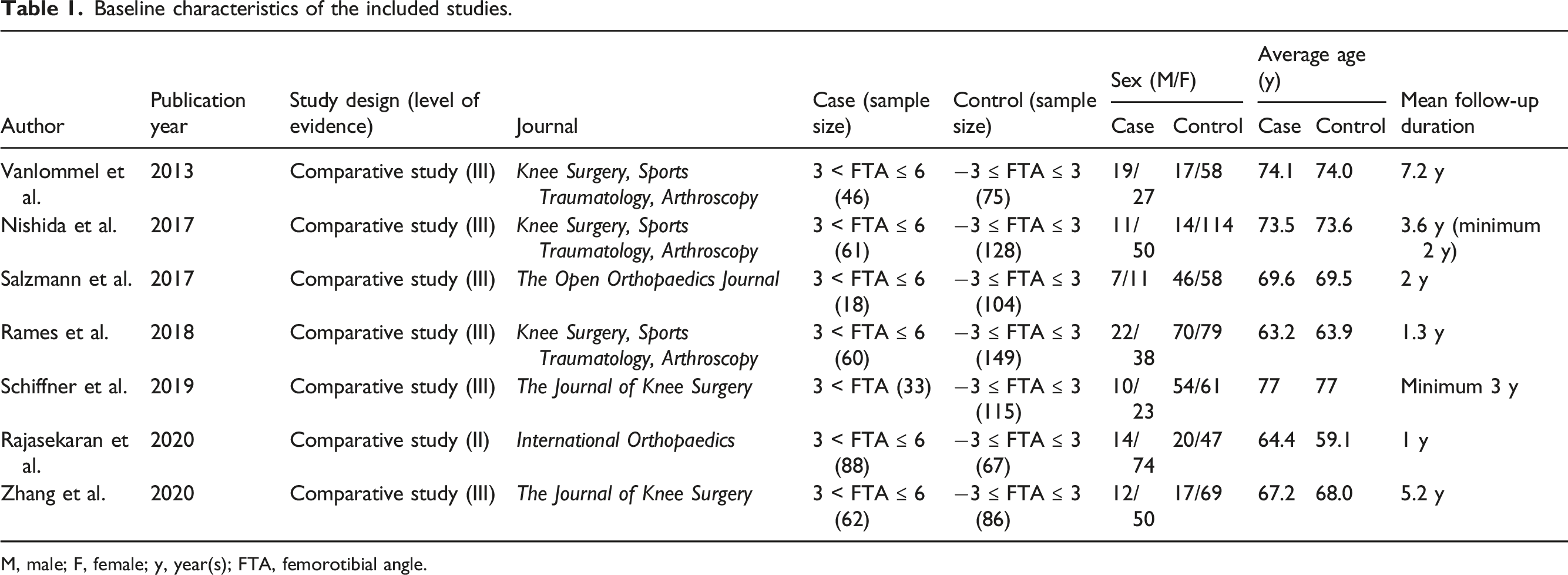
M, male; F, female; y, year(s); FTA, femorotibial angle.
Quality assessment of the included studies.

Knee Society knee and functional scores
Functional results of the included studies.

n.s: not significant; KSS: Knee Society score; KSKS: Knee Society knee score; KSFS: Knee Society functional score; WOMAC: Western Ontario and McMaster University Osteoarthritis Index; ADL: activities of daily living; FJS: forgotten joint score; HFKS: high flexion knee score; SF-12: 12-Item Short Form Health Survey; PCS: physical component score; MCS: mental component score; KOOS: knee injury osteoarthritis outcome score.

Forest plots showing intergroup comparisons of the postoperative knee society knee score. CI, confidence interval; MA, mechanical alignment; RV, residual varus; SD, standard deviation; SMD, standardized mean difference.

Forest plots showing intergroup comparisons of the postoperative knee society function score. CI, confidence interval; MA, mechanical alignment; RV, residual varus; SD, standard deviation; SMD, standardized mean difference.
Western ontario and mcmaster university osteoarthritis index
Four studies provided results for the postoperative WOMAC, with three studies showing similar results in both groups and one study suggesting better results for TKA with RV alignment21,27,30,31 (Table 3). However, the pooled results did not reveal any statistical differences between MA TKA and TKA with RV alignment (SMD: −0.25; 95% CI: −0.57 to 0.07; p = 0.12; Figure 4). Forest plots showing intergroup comparisons of the postoperative Western Ontario and McMaster University Osteoarthritis Index. CI, confidence interval; MA, mechanical alignment; RV, residual varus; SD, standard deviation; SMD, standardized mean difference.
Oxford knee score
Three studies compared the OKS between MA TKA and TKA with RV.28–30 All three studies did not show significant intergroup differences with respect to the OKS (Table 3). The pooled results indicated no differences in the OKS between the two groups (SMD: 0.06; 95% CI: −0.15 to 0.27; p = 0.56; Figure 5). Forest plots showing intergroup comparisons of the postoperative Oxford knee score. CI, confidence interval; MA, mechanical alignment; RV, residual varus; SD, standard deviation; SMD, standardized mean difference.
Forgotten joint score
Two studies provided results for the postoperative FJS, with one study showing similar results in the two groups and one study suggesting better results for TKA with RV alignment27,28 (Table 3). However, the pooled results showed no statistically significant intergroup differences with respect to the FJS (SMD: 0.41; 95% CI: −0.18 to 1.00; p = 0.18; Figure 6). Forest plots showing intergroup comparisons of the postoperative forgotten joint score. CI, confidence interval; MA, mechanical alignment; RV, residual varus; SD, standard deviation; SMD, standardized mean difference.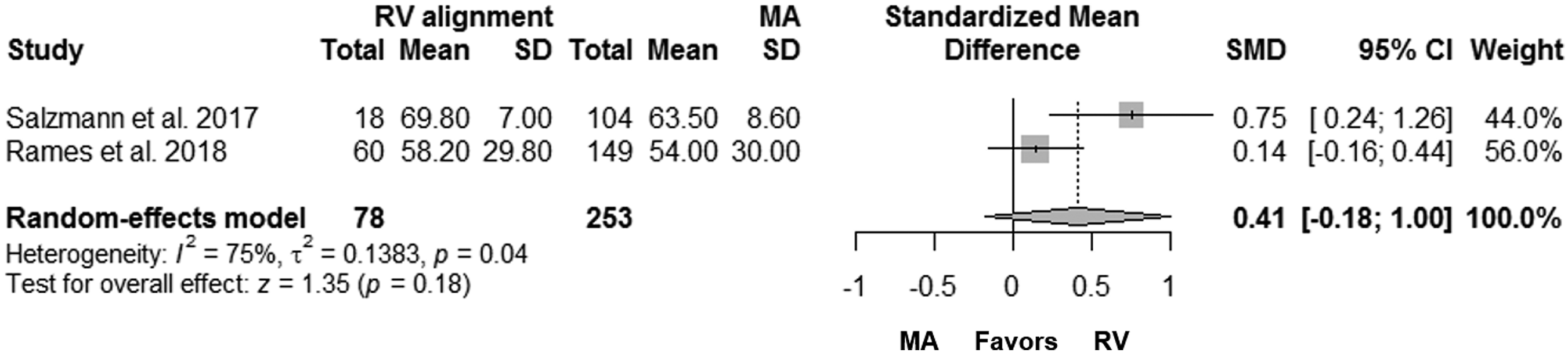
Discussion
The principal finding of the present meta-analysis is that RV alignment does not improve the postoperative functional outcomes with respect to KSKS, KSFS, WOMAC, OKS and FJS compared with MA in TKA for varus osteoarthritis.
Achieving MA has been emphasized as one of the key requisites to create a biomechanically friendly prosthetic knee.5–7 However, some evidence suggests that implant survivorship at 15 years is equivalent among the neutral, varus, and valgus aligned knees, with advancements in prostheses.32,33 Furthermore, with the recent advancements in computer-assisted navigation, surgeons can perform component positioning with greater precision. 9 With an increased recognition that the incidence of dissatisfaction is reportedly over 20% in patients after TKA and constitutional varus knees are more common, there is speculation validity of the long-held tenet that neutral MA is a requisite for the success of TKA.8,10–12 As achieving MA is not to restore the constitutional alignment and can affect the gait biomechanics, leaving RV alignment has been proposed as an alternative in patients with constitutional varus alignment10–16.
Nevertheless, it is still controversial in the available literature, and surgeons remain uncertain regarding the effects of leaving RV alignment in TKA for varus osteoarthritis.19–21 Therefore, the present meta-analysis reviewed the available comparative studies to clarify the beneficial effects of RV alignment compared with those of MA in TKA for varus osteoarthritis. The present meta-analysis showed that RV alignment did not lead to significant improvements in the functional outcomes compared with MA in TKA for varus osteoarthritis. Several studies comparing TKA with RV alignment and MA TKA were excluded from the present meta-analysis owing to comparability issues. Consistent with the results of the present study, Magnussen et al. 34 and Saragaglia et al. 35 reported similar functional outcomes with respect to the International Knee Society score and OKS. Meneghini et al. 19 and Kuroda et al. 36 also showed no intergroup differences in the patient-reported scores, such as the 2011 Knee Society score and University of California Los Angeles activity-level scores. Furthermore, Hatayama et al. 37 and Ro et al. 38 concluded that postoperative RV alignment did not lead to improvements in patient function. Therefore, to date, there is only weak evidence supporting that RV alignment confers significant advantages in terms of functional outcomes compared with MA in TKA.
With respect to achieving successful TKA, the longevity of prostheses should be considered a higher priority than achievement of an alternative alignment other than MA. Despite recent reports showing equivalent long-term survivorship among the neutral, varus, and valgus aligned knees,32,33 a large amount of evidence is available that indicates that malalignment is associated with increased strain and higher failure rates. Varus malalignment of the tibial component alters the distribution of tibial loading with a posteromedial hotspot of concentrated strain, which can lead to increased failure rates.6,39–43 Femoral component malalignment of >8° or <2° valgus relative to the anatomical femoral axis is reportedly associated with an increased failure rates.44,45
Furthermore, there is concern regarding the reproducibility of component positioning aimed at achieving “mild” varus lower limb alignment. Although the advancements in technology have significantly mitigated human errors, 4–9% of outliers in overall lower limb alignment and femoral and tibial components remain even with computer-assisted navigation. 46 Therefore, to date, RV alignment may not be recommended without conclusive evidence of functional improvement and long-term survival because the principal objective of TKA is achievement of a well-functioning and importantly “durable” joint.
Nevertheless, one remaining issue is that previous studies have not investigated the knees in which RV alignment was intentionally retained.20,21,27–31 This intention may be important for selecting RV alignment as an alternative to MA because an individualized limb alignment analysis is required to determine the relative contributions of the phenotypes of the tibia and femur towards constitutional alignment.47,48 Given that femoral and tibial phenotypes vary widely, an individualized approach with an individualized limb alignment analysis and determination of phenotypes of the tibia and femur, not unintentional retention of RV alignment, but may be essential for achieve RV alignment. Recently, favorable or improved functional outcomes through individualized alteration of alignments.49,50 However, this issue should be reevaluated and the necessity of RV alignment should be reconsidered in the future, based on studies with higher levels of evidence on longevity of the prosthesis and functional benefits of the procedure.
To the best of our knowledge, this is the first meta-analysis to verify whether leaving RV alignment after TKA leads to improvements in the functional outcomes compared with MA. With respect to the included studies, only case–control studies comparing TKA with RV alignment and MA TKA for the knees with varus osteoarthritis were selected. Therefore, it was possible to make a qualified conclusion.
The limitations of this review should also be noted. First, and perhaps the most important limitation, the study design differed among the included articles. Most of the studies included in this meta-analysis were observational studies with variable methodological quality; hence, the possibility of inherent heterogeneity cannot be disregarded. Nevertheless, all included studies showed similar and strict inclusion and exclusion criteria for the selection of the case and control cohorts. Second, different scoring systems were used for the assessment of the functional outcomes among the studies. Therefore, it was difficult to perform a pooled analysis of each individual item. Although Salzmann et al. 27 and Schiffner et al. 29 suggested better functional outcomes with respect to the high flexion knee scores and knee injury osteoarthritis outcome scores in TKA with RV alignment, these results were not included in the pooled analyses. Further, the ceiling effects for various methods of outcome measurements may have affected the results. The absence of ceiling effects may be essential for precisely analyzing the effect of RV alignment. Third, we could not draw a definite conclusion based on our analyses, owing to the lack of long-term survival results after TKA with RV alignment. Therefore, well-organized comparative studies with long-term follow-ups and larger sample sizes are required to establish a definite conclusion about the necessity of RV alignment in TKA for varus osteoarthritis. Fourth, publication bias could not be evaluated using funnel plots, and the possibility of publication bias is acknowledged. Tests for publication bias should be used only when a meta-analysis includes at least 10 studies because the power of the tests would be too low to distinguish between chance and real bias when less than 10 studies are included. 51
Conclusion
The beneficial effects of RV alignment on the functional outcomes are limited compared to those of MA in TKA for varus osteoarthritis to date. Currently, TKA with neutral MA should be considered as the gold standard.
Footnotes
Authors’ contribution
Conception and design: SB Han, KH Shin
Data collection: SB Han, JH Kim, KM Jang, KH Shin
Analysis and interpretation: SB Han, KM Jang, SB Kim, KH Shin
Writing the article: KH Shin, SB Han
Critical revision of the article for intellectual content: KH Shin, SB Han, SB Kim
Final approval of the article: KH Shin, SB Han, KM Jang, JH Kim, SB Kim
Statistical analysis: KH Shin
Obtained funding: Not applicable
Overall responsibility: KH Shin.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Aproved from the institutional review board of Anam Hospital of Korea University Medical Center.