
Abstract
Purpose
To thoroughly compare the outcomes between exposed and buried Kirschner wires (K-wires) in fixation for pediatric supracondylar humerus fractures.
Methods
We examined patients who underwent surgery at our institution between January 2007 and June 2021. We investigated their age, sex, fracture pattern, number of K-wires used, whether they were exposed or buried, operative time, postoperative complications, number of outpatient visits, duration from surgery to K-wire removal, total length of hospitalization, and perioperative radiographic parameters. After propensity score matching, intergroup comparisons were performed to assess the differences in postoperative complication rate, number of outpatient visits, duration from surgery to K-wire removal, total length of hospitalization, and loss of reduction.
Results
Propensity score matching resulted in 43 pairs in both groups. Although more patients complained of skin irritation in the buried K-wire group, there was more backing out of the K-wire in the exposed K-wire group (p < 0.01). There were no significant differences in other complications. There were more outpatient visits in the buried K-wire group (p < 0.01). The duration from surgery to K-wire removal and the total length of hospitalization were significantly longer in the buried K-wire group (p < 0.01). There was no significant difference in the loss of Baumann’s angle (p = 0.61), tilting angle (p = 0.48), or the development of rotation (p > 0.99) between groups.
Conclusion
More outpatient visits and longer lengths of hospitalization in the buried K-wire group may lead to increased costs and burden on parents.
Introduction
Displaced pediatric supracondylar humerus fractures (PSHFs) are usually treated with reduction and percutaneous pinning.1, 2 In fixation for PSHFs, Kirschner wire (K-wire) ends may be exposed over the skin or buried beneath the skin according to the surgeons’ discretion. Exposed K-wires may theoretically pose as entry points for infection. Although a reduction in the time to K-wire removal may reduce the risk of infection, a short duration of fixation may not be adequate for secure bone union to occur. 3
Although a few studies have compared exposed and buried K-wires in fixation for lateral condyle fractures of the humerus in children, no study has performed a detailed comparison between exposed and buried K-wires in fixation for PSHFs. Furthermore, to the best of our knowledge, none of the aforementioned studies adjusted for potential confounding factors between the two groups, resulting in a major problem in intergroup comparisons.4–7 Therefore, there is currently no clear evidence as to whether K-wires should be exposed or buried in fixation for PSHFs.
To test the hypothesis that exposed K-wires are superior to buried K-wires, we conducted this retrospective cohort study using propensity score matching analysis to thoroughly compare the outcomes between the two groups.
Materials and Methods
Study design
This retrospective cohort study used propensity score matching analysis to compare study outcomes between exposed and buried K-wires in fixation for PSHFs. The study was conducted with the approval of the appropriate institutional review board (No. 1249). Informed consent was obtained in the form of an opt-out on the website in accordance with domestic regulations.
Study setting and participants
The sample size was determined based on the number of cases at our institution during the study period. We examined consecutive patients aged 1–13 years with PSHFs who were surgically treated at our institution between January 2007 and June 2021. First, a computerized search of the administrative database was performed to identify potential cases. Second, patients were screened according to the inclusion criterion (Figure 1), i.e., surgically treated PSHF patients who had been followed up at our institution until K-wire removal. We excluded patients with open and ipsilateral fractures and those who underwent surgical techniques other than cross-pinning. Cases of open reduction were excluded because the previous indications for open reduction at our institution were ambiguous. Patients with a history of contralateral supracondylar humerus fractures were also excluded to accurately evaluate the quality of reduction. Patient inclusion criteria.
Data source and variables
A data form was created to record information about the patients included in the study. The final form included the following information: age, sex, fracture pattern, number of K-wires used, whether the K-wire was exposed or buried, operative time, postoperative complications, number of outpatient visits, duration from surgery to K-wire removal, total length of hospitalization on first and second operation, and perioperative radiographic parameters.
To determine the fracture pattern, we used the modified Gartland classification for extension-type fractures: type I injuries are nondisplaced, type II injuries are displaced anteriorly (anterior humeral line anterior to capitellum) but have posterior humeral cortical contact, and type III fractures are displaced with no cortical contact. 8
The potential postoperative complications included ulnar nerve palsy; compartment syndrome; superficial infection; deep infection, such as osteomyelitis and septic arthritis; skin irritation, including perforation; backing out of the K-wire (Figure 2); unexpected K-wire removal; and nonunion, as reported in a previous study.
9
Perioperative radiographic parameters were measured using software on our digital imaging system (EV Insite; PSP Corporation, Tokyo, Japan). For radiographic parameters, the postoperative Baumann’s angle (BA) and tilting angle (TA) were measured in X-ray images acquired immediately after surgery. The BA and TA were also measured immediately before K-wire removal, and the difference in the values measured postoperatively and immediately before K-wire removal was calculated. Each parameter was measured three times by the first author, and average values were used for statistical analyses. Rotatory alignment was also analyzed by assessing the symmetry of reduction of the bilateral column in the coronal plane and the presence of an anterior spike in the sagittal plane. Postoperative X-ray images were compared with those immediately before K-wire removal to investigate the development of rotational deformity. Example of backing out of the K-wire. Left: postoperative X-ray, Right: Three weeks after the surgery.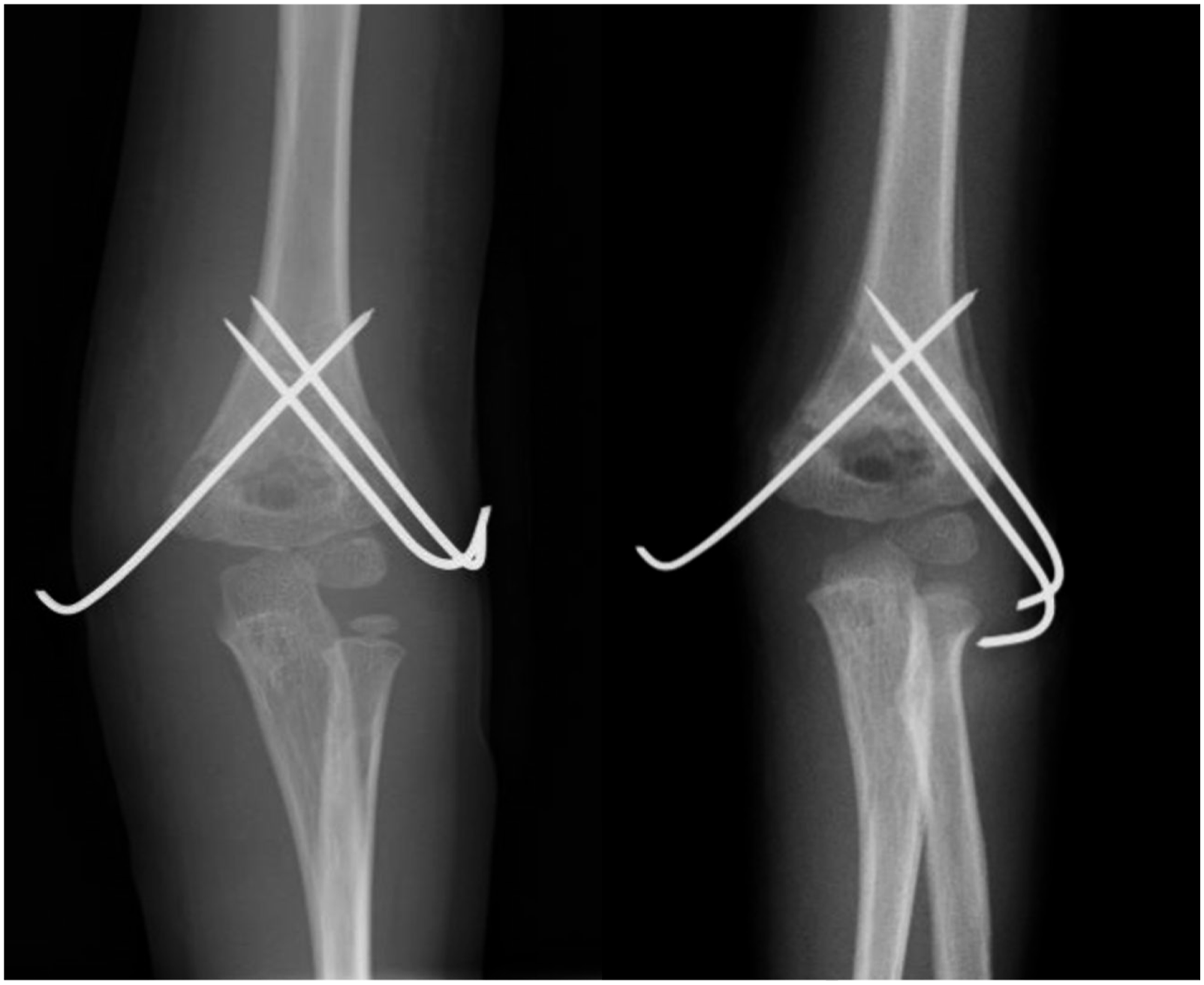
Surgical technique and postoperative follow-up
General anesthesia was administered to all patients during surgery. After induction of general anesthesia, cefazolin sodium was administered at a dose appropriate for the weight of each patient at the start of surgery. At least one senior consultant participated in all the surgeries. Closed reduction was attempted in all patients. We performed reduction referencing the BA and anterior humeral line under a biplane image intensifier. After acceptable reduction was achieved, cross-pinning was performed for fixation using two or three K-wires at the surgeon’s discretion. In fixation using three K-wires, two were first inserted from the radial side and one from the ulnar side. In ulnar-side pinning, the elbow was extended to no less than 45 degrees of flexion to avoid ulnar nerve subluxation. 10 As previously reported, we preferred to pierce the skin directly rather than make skin incisions for K-wire insertion. 4 Sufficient bicortical fixation was done for all K-wires. In burying the K-wire ends, they were cut at a length of 10–20 mm depending on the physique and bent on the cortical bone at 130–150 degrees. A long-arm cast was applied postoperatively.
Patients were required to visit the outpatient clinic every 1–2 weeks until bone union. During the patient visits, the surgical wound and biplane X-ray images were assessed. If a superficial infection was suspected, oral antibiotics were administered. Generally, exposed K-wires were removed in outpatient settings after confirmation of sufficient bone union. Buried K-wire removal generally required a second operation under general anesthesia with hospitalization.
Statistical analyses
Baseline characteristics of the study population.
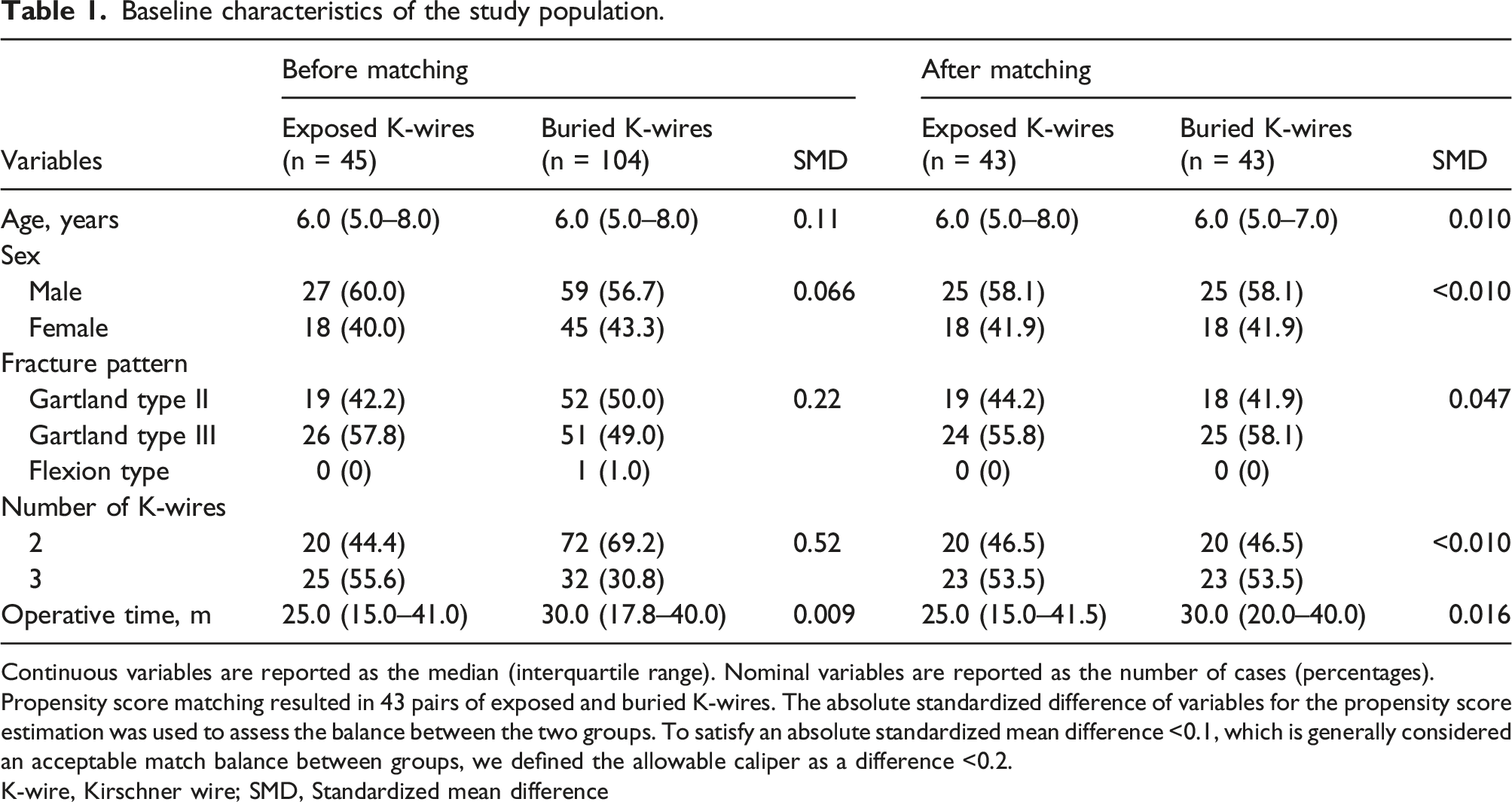
Continuous variables are reported as the median (interquartile range). Nominal variables are reported as the number of cases (percentages).
Propensity score matching resulted in 43 pairs of exposed and buried K-wires. The absolute standardized difference of variables for the propensity score estimation was used to assess the balance between the two groups. To satisfy an absolute standardized mean difference <0.1, which is generally considered an acceptable match balance between groups, we defined the allowable caliper as a difference <0.2.
K-wire, Kirschner wire; SMD, Standardized mean difference
The intergroup comparison involved assessing differences in the postoperative complication rate, number of outpatient visits, duration from surgery to K-wire removal, total length of hospitalization, and loss of reduction. Differences between continuous variables were calculated using the Mann–Whitney U test. Differences between nominal variables were determined using Fisher’s exact tests. For all statistical inference tests, differences were considered significant at p < 0.05.
Data analyses were performed using EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan). 12 Missing values were dealt with using the available case analyses.
Results
Baseline characteristics of the study population
In this study, 192 potential patients were identified from the administrative database (Table 1). Forty-three patients were excluded because they did not meet the inclusion criteria. Thus, 149 patients were included in the study. Propensity score matching resulted in 43 pairs of patients with exposed and buried K-wires.
Postoperative complications
Postoperative complications between the propensity score-matched groups.

Variables are reported as the number of cases (percentages).
There was no incidence of ulnar nerve palsy, compartment syndrome, deep infection, or nonunion. According to Fisher’s exact test, more patients complained of skin irritation or perforation in the buried K-wire group (p < 0.01). However, there was more backing out of the K-wire in the exposed K-wire group (<0.01) than in the buried K-wire group. There was no significant difference in superficial infection (p > 0.99), unexpected K-wire removal (p > 0.99), and total complication rate (p = 0.66). *p < 0.05.
K-wire, Kirschner wire
Number of outpatient visits, duration from surgery to K-wire removal, and total length of hospitalization
Number of outpatient visits, duration from surgery to K-wire removal, and total length of hospitalization of the propensity score-matched groups.

Variables are reported as the median (interquartile range).
According to the Mann–Whitney U test, the number of outpatient visits (p < 0.01), duration from surgery to K-wire removal (p < 0.01), and total length of hospitalization (p < 0.01) were significantly greater in the buried K-wire group.
✢ Data were missing for five patients with exposed and two with buried K-wires. *p < 0.05.
K-wire, Kirschner wire
Loss of reduction
Loss of reduction between the propensity score-matched groups.

Continuous variables are reported as median (interquartile range). Nominal variables are reported as the number of cases (percentages).
According to the Mann–Whitney U test, there was no significant difference between the two groups regarding the loss of BA (p = 0.61) and TA (p = 0.48). According to Fisher’s exact test, there was no significant difference in the development of rotational deformity (p > 0.99).
There were no missing data.
K-wire, Kirschner wire; BA, Baumann’s angle; TA, tilting angle
Discussion
This study has some notable findings. First, although significant differences in skin irritation and backing out of the K-wire were found between the two groups, no significant difference was noted in other complications. Second, there were more outpatient visits in the buried K-wire group than in the exposed group, and the duration from surgery to K-wire removal and total length of hospitalization were significantly longer in the buried K-wire group than in the exposed K-wire group. Finally, we did not find a significant difference in loss of reduction between the two groups.
Postoperative complications
There were no incidences of ulnar nerve palsy, compartment syndrome, or nonunion. The risk of infection in exposed K-wires is thought to be higher because of bacterial tracking along the K-wire. Wormald et al. evaluated the association of infection rate with exposed or buried K-wires in upper extremity fracture fixation, 13 but this systematic review revealed the lack of evidence to support decision-making regarding burying or not burying K-wires in the upper extremities. However, as various factors, such as fracture site and pattern and whether immobilization is applied postoperatively, potentially affect the risk of infection, we believe that not all upper extremity fractures should be placed in the same category for the investigation of the infection rate. In this study, no significant difference in superficial infection was noted between the two groups in fixation for PSHFs. All patients with infection in the buried K-wire group complained of previous skin irritation and perforation, which may have led to the equivalence in the infection rate between the two groups. In this study, six (14.0%) patients with buried K-wires experienced skin perforation. The proportion of skin irritation in buried K-wires is consistent with that reported in a previous study on lateral condyle fractures of the humerus. 5 We believe that skin irritation and perforation are the greatest disadvantages of burying K-wires in fixation for PSHFs. In this study, more cases of K-wire backing out occurred in the exposed K-wire group. This result was expected as there was a higher likelihood of directly touching the ends of exposed K-wires compared to buried K-wires; however, the backing out of the K-wire did not lead to a greater loss of reduction in exposed K-wires, as described later.
Number of outpatient visits, duration from surgery to K-wire removal, and total length of hospitalization
Compared with burying of K-wires, the exposure of K-wire ends may theoretically lead to more frequent outpatient visits for surgical wound care. However, in this study, there were more outpatient visits in the buried K-wire group. We believe that this was due to complaints of skin irritation and perforation. In cases of skin irritation, there were many unexpected outpatient visits because all parents had trepidation regarding their children’s complaints of pain. In addition, once skin irritation led to perforation and superficial infection, surgical wound care became more complicated and frequent compared with that seen in cases with exposed K-wires. The duration from surgery to K-wire removal and the total length of hospitalization were significantly longer in the buried K-wire group. All patients with buried K-wires required a second operation under general anesthesia during removal. Therefore, buried K-wire removal had to be planned, taking into consideration other scheduled surgeries at the institution, which increased the duration from the first surgery to K-wire removal. The necessity of general anesthesia in K-wire removal also led to longer hospitalization. The most important factor is that more outpatient visits and longer lengths of hospitalization may lead to increased costs. Previous studies have reported that exposed K-wires are possibly superior to buried K-wires regarding cost-effectiveness in fixation for lateral condyle humerus fractures,4,5,7 which is consistent with the results of this study on PSHFs. More outpatient visits, longer duration from surgery to K-wire removal, longer length of hospitalization, and increased financial implications may also be inconvenient for the parents of the patients.
Loss of reduction
The distal epiphysis of the humerus has limited potential for remodeling. Posteromedial rotational displacement particularly results in a higher BA, indicating a cubitus varus deformity. 14 Therefore, it is important to achieve accurate anatomical reduction and stable fixation of PSHFs. Although complications, such as backing out of the K-wire or unexpected K-wire removal, can affect the maintenance of reduction, no studies have thoroughly assessed the influence of K-wire exposure or burial on loss of reduction after fixation for PSHFs.
In this study, both coronal and sagittal alignments were maintained. No significant difference in the loss of BA and TA was found between the two groups. Moreover, no significant difference in the development of rotational deformity was observed between the two groups. Thus, whether the K-wire was exposed or buried did not affect the loss of reduction.
Limitations
This study had several limitations, mainly owing to its retrospective design. First, this was a retrospective cohort study performed in a tertiary referral center; thus, selection bias could not be avoided. Second, there might have been measurement bias because the measurements of radiographic parameters were not blinded. Third, data collection was limited because this was a single-center study, which may have led to a lack of power. Fourth, the data were accumulated over a long period, from 2007 to 2021, when many different surgeons performed the operations. This could lead to heterogeneity in the surgical technique. Finally, institution-specific factors may limit the generalizability of these findings. For these reasons, further studies should consider the use of multiple centers to provide larger sample sizes.
Conclusions
There were more outpatient visits when the K-wires were buried. The duration from surgery to K-wire removal and the total length of hospitalization were significantly greater in the buried K-wire group. These results may lead to increased costs and burden on parents, which is a significant disadvantage of buried K-wires. We believe that exposed K-wires are more reasonable than buried K-wires in fixation for PSHFs.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.