
Abstract
Objective
This study aimed to investigate the minimum effective concentration (MEC90, defined as effective in 90% of patients) of ropivacaine during the combined procedure of adductor canal block (ACB) and infiltration between the popliteal artery and capsule of the posterior knee (IPACK) block for patients undergoing total knee arthroplasty.
Methods
This double-blind, randomized dose-finding trial was based on a biased coin up-and-down sequential design, where the concentration of ropivacaine administered to a given patient depended on the previous patient’s response. Before surgery, the first patient received 20 mL of 0.2% ropivacaine for ACB and again for IPACK. If the block failed, the next subject received a 0.025% higher ropivacaine concentration; otherwise, the next subject received either a 0.025% smaller dose (probability of 0.11) or the same dose (probability of 0.89). The primary outcome was whether the block was successful. Block success was defined as the patient did not suffer significant pain and did not receive rescue analgesia within 6 h after surgery. MEC90 was estimated by isotonic regression, and the 95% confidence interval (CI) was calculated by bootstrapping. Secondary outcomes were numerical rating scale (NRS) pain scores at postoperative 24 h and 48 h, postoperative morphine consumption, and time to hospital discharge. Secondary outcomes were compared between patients whose blocks succeeded with those which failed.
Results
Based on analysis of 52 patients, the MEC90 was 0.247% (95% CI 0.227–0.271%), MEC95 was 0.260% (95% CI 0.244–0.282%) and MEC99 was 0.272% (95% CI 0.260–0.291%). In contrast, four of nine trials in a recent systematic review reported ropivacaine concentrations below 0.247%. Patients whose blocks succeeded (n = 45) had significantly lower NRS pain scores, lower morphine consumption, and shorter hospitalization than patients whose blocks failed (n = 7).
Conclusions
Our small trial suggests that 0.247% ropivacaine in 20 mL respectively can provide successful ACB + IPACK block in 90% of patients. However, given that many published trials have used lower concentrations, our findings should be verified in larger studies.
Keywords
Introduction
Total knee arthroplasty is one of the most common surgical procedures for patients with end-stage knee degenerative diseases, 1 but it is associated with moderate to severe postoperative pain in more than 60% of patients.2,3 Inadequate pain management can delay recovery and reduce patient satisfaction.4,5 Multimodal pain protocols and regional anesthesia have substantially mitigated pain after total knee arthroplasty and shortened the associated hospitalization.6,7 For example, peripheral nerve block is a widely used technique of multimodal pain protocol,8,9 and extensive studies have explored the analgesic efficacy of combining adductor canal block (ACB) and infiltration between the popliteal artery and capsule of the posterior knee (IPACK) block in order to block only sensory nerves.10–16 In fact, ACB + IPACK block is recommended by some researchers for postoperative analgesia in enhanced recovery protocols after total knee arthroplasty.1,10,17,18
The optimal concentration of ropivacaine for ACB + IPACK block is unclear. Previous studies have reported concentrations from 0.2% to 0.5%.10,15,16,19,20,21 Since the dose should be optimized to minimize risk of systemic toxicity, 22 we conducted a double-blind, randomized dose-finding trial in order to determine the minimum effective concentration (MEC90, defined as effective in 90% of patients) of ropivacaine for ACB + IPACK block in patients undergoing total knee arthroplasty.
Methods
This study was approved by the Clinical Trials and Biomedical Ethics Committee of our institution, and written informed consent was obtained from all subjects.
Patient recruitment
To be enrolled in this study, patients had to older than 18 years, diagnosed with osteoarthritis, and scheduled for primary unilateral total knee arthroplasty under general anesthesia. Patients also had to have an American Society of Anesthesiologists functional status of I–III, as well as normal quadriceps strength.
Patients were excluded if they presented with any of the following: knee flexion deformity ≥ 30°, varus-valgus deformity ≥ 30°, known allergies to the drugs used in this study, history of open knee surgery or knee infection, drug addiction, or neuromuscular disorder. Patients were also excluded if they were unable to communicate verbally.
Study design
This trial was a double-blind, randomized study to estimate MEC90 for ultrasound-guided, single-injection ACB + IPACK block in patients undergoing total knee arthroplasty. Drug concentration was assigned using a biased coin up-and-down sequential design, where the concentration of local anesthetic administered to a given patient depended on the previous patient’s response. The first patient to be recruited received 20 mL 0.2% ropivacaine (AstraZeneca, London, England) for ACB and 20 mL 0.2% ropivacaine for IPACK. If the block was successful in the first patient, the next patient was randomized to receive either the same ropivacaine dose (at a probability of 0.89) or a 0.025% lower dose (at a probability of 0.11). If, however, the block failed in the first patient, the next patient received a 0.025% higher concentration. The maximum concentration was set at 0.5%. If the block failed in a patient who received this maximum concentration, the next patient did not receive a higher concentration. The assessment criteria for block success were shown in the outcome section.
The sequential allocation of biased coin up-and-down sequential design was carried out using a computer-generated list of random numbers prepared by a statistician with Microsoft Excel (Redmond, WA, USA). Investigator 1 accessed the list and prepared the corresponding syringes of ropivacaine in the central pharmacy, adding epinephrine (CrandpharmaCo.Ltd., Wuhan, China) (2.0 μg/mL) to all ropivacaine formulations. Then Investigator 1 carried the syringes to the operating room. In this way, the patient, anesthesiologist, surgeon, and postoperative caregiver were blinded to concentration allocation.
Analgesic procedures
One anesthesiologist performed all ACB and IPACK procedures in the operating room for all patients 30 min before general anesthesia. After subcutaneous infiltration with 1 mL of 2% lidocaine, ACB and IPACK block were performed with the patient in the supine position. For ACB (Figure 1), a high-frequency linear-array ultrasonic transducer (Anesus ME7, Mindray, Shenzhen, China) was used to scan the middle of the thigh, halfway between the inguinal crease and patella, in order to identify the adductor canal, superficial femoral artery, sartorius, adductor longus, and adductor magnus. The site of injection was chosen as the anterolateral hyperechoic structure of the artery (saphenous nerve and nerve to vastus medialis). Once the site was located, a 21-gauge, 100-mm needle (Pajunk, Geisingen, Germany) was introduced in-plane in a lateral to medial direction. Correct needle placement was confirmed using 3 mL of isotonic saline, then 20 mL of ropivacaine was injected. Ultrasound-guided adductor canal block. AL, adductor longus; FA, femoral artery; SM, sartorius muscle; SN, saphenous nerve; VM, vastus medialis; line, needle insertion point.
Infiltration between the popliteal artery and capsule of the posterior knee was performed using the same ultrasonic transducer mentioned above (Figure 2). The anesthesiologist identified the popliteal artery at the popliteal crease and moved cephalad just beyond the femoral condyles, to where the condyles merged with the shaft of the femur. The tibial and peroneal nerves superficial to the popliteal artery were located, and when the space between the femur and popliteal artery was located, the needle was inserted in-plane in a medial to lateral direction. The tip was positioned at the middle of the femur, near the lateral border near the periosteum. Then 5–10 mL of ropivacaine was injected to ensure adequate spread to the lateral end of the femur. As the needle was withdrawn, the rest of the ropivacaine was injected along the femur, such that 5 mL infiltrated incrementally into the area between the artery and femur, ending at the medial end of the femur. Altogether 20 mL of ropivacaine was injected during IPACK. Ultrasound-guided infiltration between the popliteal artery and capsule of the posterior knee block. FB, femoral bone; PA, popliteal artery; SN, saphenous nerve; line, needle insertion point.
Surgery and concomitant medication
On the day before surgery, celecoxib (200 mg) was administered twice as a preemptive analgesic. Patients were instructed to fast for 8 hours before surgery and to drink 100 mL of a clear, pure carbohydrate liquid 2 hours before surgery. All surgeries were conducted under general anesthesia. After pure oxygen inhalation, the following anesthetics were administered intravenously: Midazolam, 2 mg/kg; Propofol, 2 mg/kg; Sufentanil, 0.3 μg/kg; and Cis-atracurium, 0.2 mg/kg. Patients were then intubated and given an inhaled anesthetic (Sevoflurane, 1–1.5 MAC). Flurbiprofen (50 mg) was administered 20 min before the end of the surgery to prevent postoperative pain, along with Tropisetron (5 mg) to prevent postoperative nausea and vomiting. At present, there is no definitive clinical evidence to support that the addition of local infiltration analgesia to ACB + IPACK block can improve analgesic outcomes. To avoid interference between the efficacy of ACB + IPACK block and local infiltration analgesia, thus we did not perform local infiltration analgesia during surgery.
After regaining consciousness, patients were sent to the post-anesthesia care unit, where Investigator 2 (postoperative caregiver) administered an opioid add-on to the multimodal pain treatment whenever the pain score at rest exceeded 3, in accordance with routine procedures at our hospital. The patients whose pain score exceeded 3 simultaneously received intravenous Sufentanil (5 μg).
After awakening from anesthesia, patients were sent to the bed ward, and an ice compress was applied around the incision. Patients did not receive any oral analgesics within 6 h after surgery. After postoperative 6 h, oral celecoxib (200 mg) and pregabalin (150 mg) were administered twice daily to control postoperative pain. If the patient was unable to tolerate the pain, a further 5 mg of morphine hydrochloride as rescue analgesia was injected subcutaneously.
Outcome assessment
The primary outcome was whether the block was successful. Block success was defined as the patient did not suffer significant pain and did not receive rescue analgesia within 6 h after surgery. The assessments were performed by Investigator 2 (postoperative caregiver), who was blinded to concentration allocation. Pain at rest was assessed in the post-anesthesia care unit, at 2 h, 4 h, and 6 h after surgery. If the pain score at rest exceeded 3 in a numerical rating scale 23 (NRS) from 0 to 10 at any time point, the patient was recorded as experiencing block failure. Pain during motion (flex the knee as much as possible) was assessed at 2 h, 4 h, and 6 h after surgery. If the pain score during motion exceeded 5 at any time point, the patient was recorded as experiencing block failure. In addition, if the patient received rescue analgesia (received Sufentanil in the post-anesthesia care unit or morphine hydrochloride in the bed ward) within 6 h after surgery, the patient was recorded as experiencing block failure.
Secondary outcomes included NRS pain scores at rest and during motion at postoperative 24 and 48 h, postoperative morphine consumption, and time to hospital discharge. The discharge criteria of patients included: adequate pain control on oral pain medication, independent transfer, ambulation alone for at least 200 feet, and the ability to climb stairs. These outcomes were compared between patients whose blocks succeeded with those which failed. In addition, any adverse events that occurred during surgery or postoperative recovery in hospital were recorded. Secondary outcomes were assessed by Investigator 2 (postoperative caregiver) who was blinded to concentration allocation.
Statistical analysis
Based on previous studies,24,25 we estimated that we would need to observe at least 45 successful ACB + IPACK blocks in order to estimate MEC90. Thus, we decided to recruit patients until we had achieved this.
Minimum effective concentration was analyzed statistically using R statistical software (R Foundation for Statistical Computing, Vienna, Austria). MEC90 was calculated using isotonic regression, and the 95% confidence interval (CI) was derived by bootstrapping.26,27 Similar procedures were used to estimate the minimum effective concentrations to produce a successful block in 95% or 99% of patients (MEC95, MEC99). 28 We used the dose estimator μ3, defined as the interpolated dose whose probability of effect was estimated to be 0.9.
Secondary outcomes were analyzed statistically using SPSS 26.0 (IBM, Chicago, IL, USA). The normality of data was assessed using histograms and quantile-quantile plots. Continuous data were presented as means and standard deviations. Inter-group differences in normally distributed data were assessed for significance using Student’s t test; differences in skewed and ordinal data, using the Mann-Whitney U test. Differences were considered significant if p < .05.
Results
Patient characteristics.

Values are n (%), or mean ± SD.
ASA, American Society of Anesthesiologists.

Graph of successful ( ) and failed ( ) blocks with different ropivacaine concentrations. The horizontal line is the calculated minimum effective concentration of ropivacaine providing successful ACB + IPACK block in 90% of patients (MEC90); error bars represent 95% confidence interval.
Observed response rates.

Values are n or percentage.
Secondary outcomes.
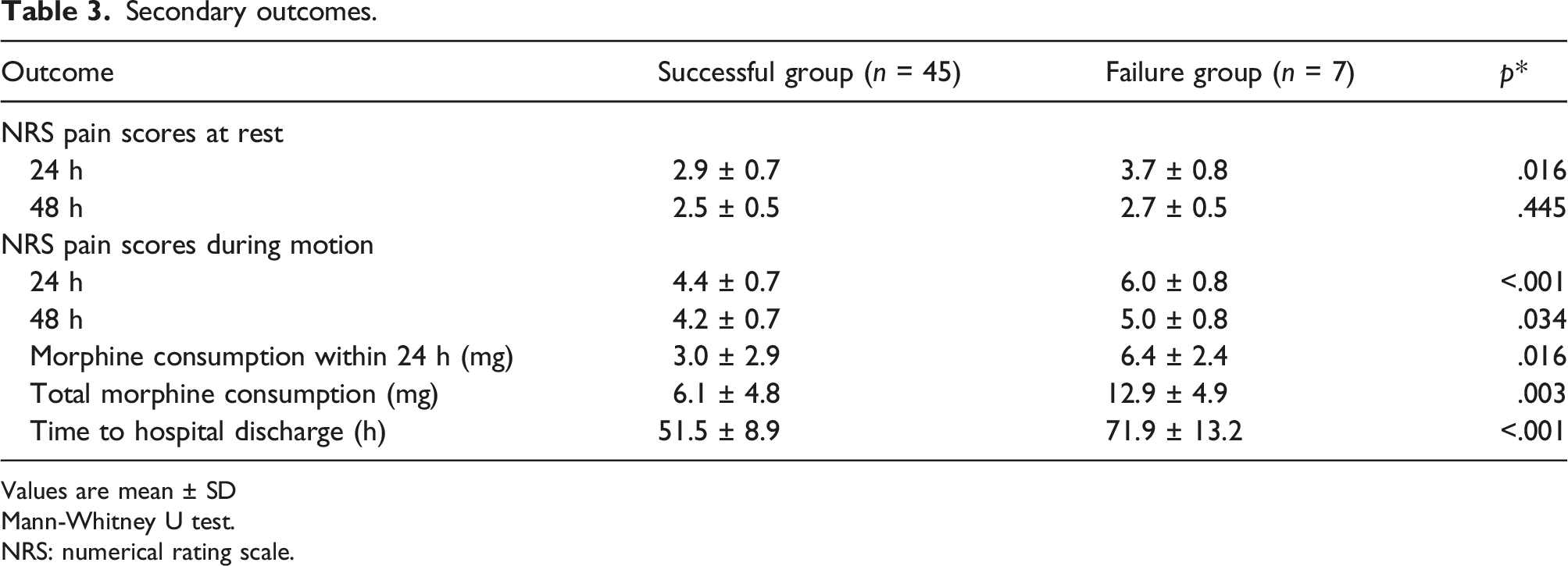
Values are mean ± SD
Mann-Whitney U test.
NRS: numerical rating scale.
During the nerve block, no events of vascular puncture were observed; after nerve block, none of the patients suffered nausea, vomiting or dyspnea before general anesthesia. After surgery, none of the patients suffered diminished quadricep strength, residual paresthesia, or residual neural deficits. None of the patients showed signs of local anesthetic intoxication during the trial.
Discussion
The characteristics of studies which comparing ropivacaine-induced ACB + IPACK block with ACB alone.

ACB: adductor canal block.
IPACK: infiltration between the popliteal artery and capsule of the posterior knee.
LIA: local infiltration analgesia.
The discrepancy about analgesic efficacy of ACB + IPACK block may reflect the use of different doses of local anesthetic, highlighting the need for the present dose-finding study. To our knowledge, we provide the first estimate of MEC90 for ropivacaine in ACB + IPACK block. We calculated a MEC90 of 0.247% (95% CI 0.227–0.271%). No adverse effects were observed during the study, suggesting that this MEC90 is safe.
Ropivacaine is a long-acting amide local anesthetic which produces less suppression of motor fibers and has a significantly higher threshold for cardiovascular and central nervous system toxicity than bupivacaine.32,33 We added epinephrine to our ropivacaine formulations because epinephrine modulates the sympathetic nervous system, which can increase analgesic potency and duration. 34 We chose 0.2% as the initial concentration in the present trial because previous studies using ropivacaine for ACB + IPACK block have used concentrations from 0.2% to 0.5%.10,15,16,19,20,21 Based on the drug instructions of ropivacaine (AstraZeneca, London, England), the action time for peripheral nerve block is about 6 h. Therefore, we chose postoperative 6 h as the endpoint of primary outcome. In the present study, we also provided some secondary outcomes to verify whether the nerve blocks were successful (primary outcome). Our results showed that patients whose blocks succeeded had significantly lower NRS pain scores, lower morphine consumption, and shorter hospitalization after surgery. These results suggested that the criteria for successful block were feasible.
We opted to estimate the MEC90 because the classic parameter of median effective dose (ED50) offers little clinical relevance. 35 To estimate MEC90, we applied a biased coin up-and-down sequential design, which can directly determine higher quantiles (ED90 and ED95) than the classical Dixon and Massy approach to estimate ED50. In addition, the biased coin up-and-down sequential design has the advantage of allocating concentrations in a sequential, interactive way, such that patients are randomized to doses more likely to be effective without causing toxicity.24,36
Our MEC90 estimate for ropivacaine, 0.247%, is higher than the concentration of ropivacaine reported in four of nine trials in a recent systematic review of analgesic procedures in ACB + IPACK block. 21 The variation in concentrations in these trials may help explain divergent results about efficacy. To obtain more reliable results, it may be worthwhile to express ropivacaine doses in terms of the MEC90 that we determined here. In this way, our MEC90 may help guide future clinical and investigational work aimed at optimizing ACB, IPACK and promoting an opioid-sparing multimodal pain management for total knee arthroplasty.
Anesthesiologists proposed IPACK to improve the defect that ACB blocks only the anteromedial sensory nerve but not the posterior or lateral sensory nerves. 11 Therefore, ACB and IPACK block were often used in combination in clinical practice. 21 In this study, we explored the minimum effective concentration of this combination, so it is difficult to prove that any effect is due to ACB or IPACK block because the effect and distribution of local anesthetic of IPACK is variable among patients. 37 Future studies are needed to explore MEC90 for ACB and IPACK block separately.
Like most previous studies on ACB + IPACK block (Table 4),15,19,20,29–31,38,39 local infiltration analgesia was not used in this study. It is not clear whether the analgesic efficacy of ACB + IPACK block combined with local infiltration analgesia is better, or whether the MEC90 for ACB + IPACK block was the same as ACB + IPACK block combined with local infiltration analgesia. Further studies are needed to explore these concerns in the future.
In this study, we set up a series of inclusion and exclusion criteria to recruit a homogenous group of patients. For example, we included patients with the same diagnosis (osteoarthritis) and we excluded patients with severe deformities or a history of knee surgery. However, it is hard to keep some characteristics such as preoperative pain or deformity very similar in all patients. This may increase the difference of individual patient’s response to postoperative pain because pain is highly subjective. The success or failure of the ABC + IPACK depends on the previous patient’s response, and the preoperative pain or deformity are not strictly controlled. This could directly affect the results and conclusions drawn from this study. This is the major limitation of this study.
In addition, our study presents several other limitations. First, the study is of relatively small size. Second, we estimated MEC90 for the case of a single injection of ropivacaine during ACB and then again during IPACK, so our results may not generalize to the case of continuous administration. 31 Third, we did not assess the effects of volume on MEC90, injecting always the same total volume of 40 mL based on previous studies.10,15,19,29,30,31,39 Other volumes of local anesthetic have been reported for ACB and IPACK block,20,38,40,41 so it is unclear whether our results can generalize to other volumes. Future work should address these limitations, as well as verify and extend our findings for a range of multimodal pain regimens.
Conclusions
Under the conditions of the present study, our biased coin up-and-down sequential design-based trial provides evidence that ultrasound-guided single injection of 0.247% ropivacaine in 20 mL respectively (containing 2.0 μg/mL of epinephrine) can provide successful ACB + IPACK block in 90% of patients undergoing total knee arthroplasty. However, given that many published trials have used lower concentrations, our findings should be verified in larger studies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was funded by 1.3.5 Project of Sichuan University West China Hospital. Grant ID: ZYJC18040.
Ethical review committee statement
This study was approved by the Clinical Trials and Biomedical Ethics Committee of Sichuan University West China Hospital, and written informed consents were obtained from all participants. The clinical trial registration number was ChiCTR2100048757 (Date of registration: 16 July 2021). This trial was prospectively registered.