
Abstract
The aim of this study is to investigate the mid-term results of 29 hips in 26 patients who underwent acetabular reconstruction using a Kerboull-type acetabular reinforcement device and impaction with hydroxyapatite (HA) granules. The acetabular bone defects were AAOS type II for six hips and type III for 23 hips. The mean Merle d’Aubigné clinical scores were significantly improved after operation. Six hips developed implant migration and breakage, and five of six hips were revised after an average of 5.5 (range 2.0–8.8) years. All hips with thickness of the grafted HA less than 10 mm were stable. As the HA became thicker, the failure rate were significantly increased. The Kaplan–Meier survival rates at 10 years were 73.2%, with 100% and 67.0% for AAOS type II and III defect respectively as the end point was failure condition. Reconstruction using a Kerboull-type acetabular reinforcement device and impaction with HA granules was an alternative method in the absence of adequate allografts.
Introduction
Total hip arthroplasty (THA) achieves excellent clinical results. 1,2 With advances in hip prostheses, the number of THAs and revision THAs has been increasing. 3,4 However, acetabular bone defects remain a major problem in revision THAs. Cemented or cementless acetabular components with morselized cancellous bone grafts that fill cavitary defects have achieved excellent results. 5 Failure of acetabular revision surgery using bulk allografts without support was previously reported, 6,7 whereas good results using morselized allografts with a reconstruction device were demonstrated by many studies. 8 –12
Revision THA with impacted bone allografts and a Kerboull-type acetabular reinforcement device (Kerboull cross plate) for large acetabular bone defects achieved excellent results. 12 Several techniques of acetabular reconstruction using cross plates with morselized bone, structural bone or artificial bone substitutes for bone defects have been proposed. 12 –15 Excellent clinical results of revision THA with HA impaction and Kerboull cross plate and KT plate were reported. 15 We previously performed revision THAs using Kerboull cross plates and impaction with hydroxyapatite (HA) granules instead of human bone grafts between 2002 and 2011. However, we observed breakage of cross plates in several of our patients. Thus, we evaluated clinical and radiological outcomes including thickness of grafted HA after surgery in patients who received revision THA using Kerboull cross plates and HA impaction to examine the failure factors.
Materials and methods
Patients
This cross-sectional, retrospective study was approved by the Institutional Review Board. We retrospectively reviewed 29 hips replaced consecutively in 26 patients (26 patients, 23 females and 3 males) who had undergone acetabular reconstruction using Kerboull cross plates and KT plates with HA granules for American Academy of Orthopaedic Surgeons (AAOS) type II or III bone defects between 2002 and 2011. 16 The mean age at revision THA was 68.6 (range 45–79) years. The mean follow-up period was 10.7 (range 7.0–15.4) years. Inclusion criteria ware failed THA, failed hemiarthroplasty with AAOS type II and III osteolysis.
The initial diagnoses were osteoarthritis secondary to acetabular dysplasia in 20 hips, rheumatoid arthritis (RA) in 4 hips, osteonecrosis of the femoral head (ON) in 3 hips, femoral neck fracture in 2 hips.
The revision surgery using Kerboull cross plates and KT plates with HA granules was undertaken for aseptic loosening of cemented cup in nine hips, aseptic loosening of cementless cup in nine hips, osteolysis and wear of the PE liner with fixed cementless cup in three hips and migration of a hemiarthroplasty in eight hips. The mean period for revision surgery was 14.4 years.
Surgical technique
All surgeries were performed by experienced surgeons under general anaesthesia, and either a posterolateral or a lateral approach was used. Specifically, failed acetabular component was exposed and removed, and underlying soft tissue membrane was cleared. The bone defect was filled and impacted with HA granules (PENTAX; Tokyo, Japan), which were a mixture of 100–300 µm, 0.9–1.2 mm and 3.0–5.0 mm granules at a ratio of 10:45:45. 17 Kerboull cross plate was placed with screws, and finally, a conventional polyethylene liner was cemented onto the plate and grafted HA (Figure 1). An original Kerboull cross plate (STRATEC Medical, Oberdorf, Switzerland) was used for initial 7 cases and KT plate (Kyocera Medical; Osaka, Japan) was used 22 cases. In 10 of 29 hips with large wall defects, reconstruction of medial, superior and posterior wall defects with autologous iliac bone grafts or allografts was performed before impaction with HA granules.
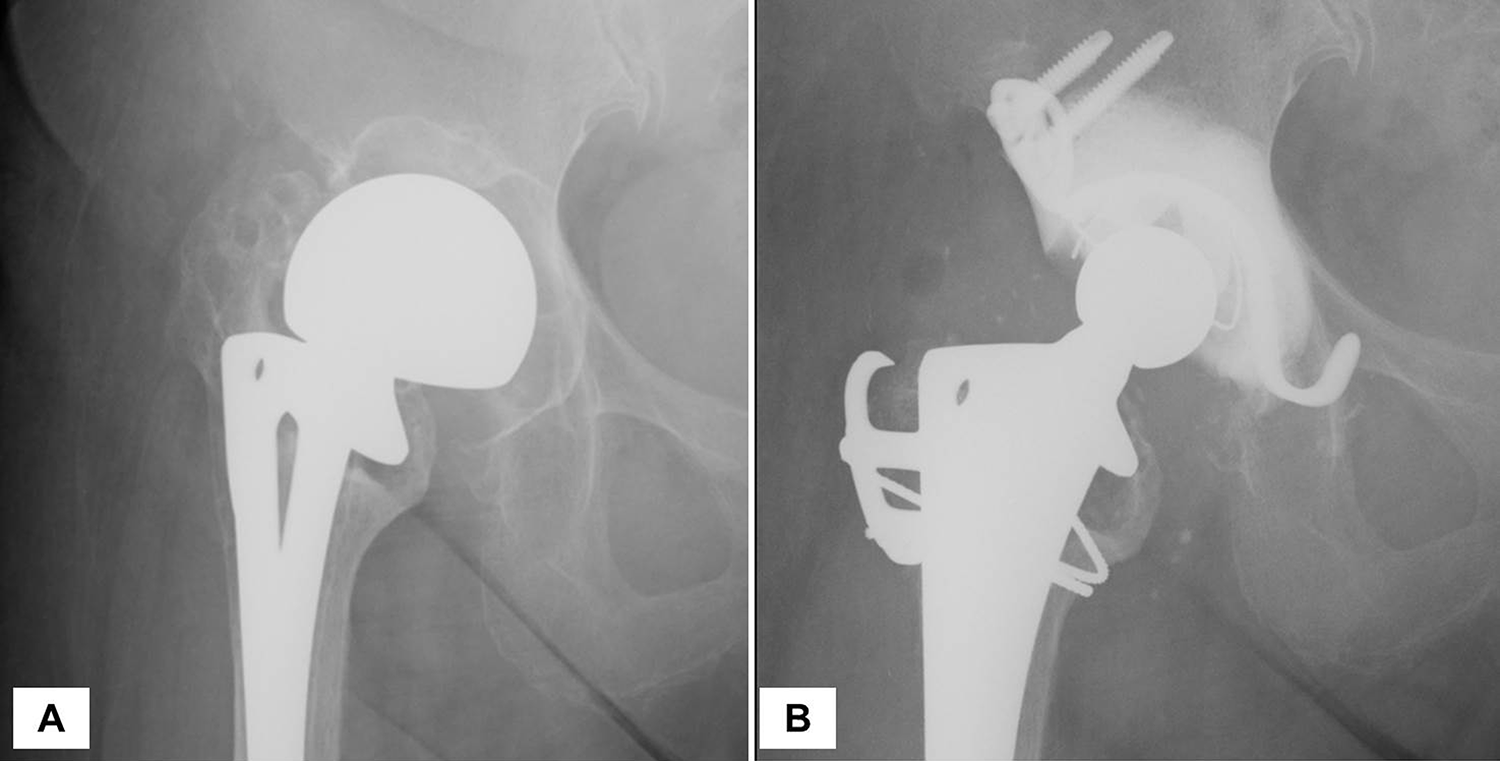
Radiographic images of representative case. (A) Failed hemiarthroplasty with acetabular bone defect. (B) The bone defect was filled and impacted with HA granules, Kerboull cross plate was placed with screws, and finally, a conventional polyethylene liner was cemented.
Outcome evaluation
Clinical outcomes were evaluated using the Merle d’Aubigné clinical score that was obtained preoperatively, at 1 year after operation and last follow-up or further acetabular revision. 18 All peri- and postoperative complications were also recorded.
Radiological parameters were evaluated using anteroposterior radiographs of the pelvis, including both hips, that were obtained at 6 months and 1 year postoperatively and annually thereafter. Migration, breakage of cross plates and changes in cup inclination were evaluated by examining vertical migration (the distance between the inter-teardrop reference line and centre of the femoral head), horizontal migration (the distance between a perpendicular reference line drawn through the teardrop and centre of the femoral head) and the angle of inclination of the acetabular device. Substantial migration was defined as a change in the angle of inclination of >3° or migration of >3 mm. 12 The maximum thickness of the grafted HA was evaluated on postoperative radiographs as the distance between the top of the margin of HA and top of the ring. 19 All parameters were adjusted for inner head size using the Image J software package (http://imagej.nih.gov/ij/). 20,21
The failed group was defined as implant breakage or migration of plate or change in plate angle. The successful and failed groups were compared with respect to patient background characteristics, radiological parameters and clinical results. The survival rate analysis was performed using the Kaplan–Meier method with the failed acetabular joint as the end point.
Statistical analysis
Statistical analyses were performed using the JMP Pro 12 (SAS Institute; Cary, NC). The comparisons of continuous variables were compared with the Mann–Whitney U test. Wilcoxon signed-rank test were used to compare the preoperative and postoperative Merle d’Aubigné score. Fisher’s exact test was used to compare demographic data. Cox regression analysis was used to assess the relationship between the thickness of grafted HA and implant survival. The cumulative probabilities of the radiographic signs were estimated with the Kaplan–Meier product-limited method, as the end point was failure condition. The significance level was set at P = 0.05.
Results
A total of 23 hips had no loosening, no implant migration and breakage at final follow-up (successful group), whereas six hips failed. In the failed group, implant breakage developed after migration in 4 hips and Kerboull cross plate gradually migrated, then breakage developed in two hips. Five of six failed hips were revised at an average of 5.5 (range 2.0–8.8) years. One hip were not revised because of low activity of daily life and poor general condition to have re-operation.
The mean Merle d’Aubigné clinical scores were significantly improved from 8.4 ± 1.7 preoperatively to 13.7 ± 1.4 at 1 year after operation (p < 0.001). At final follow-up total score were12.8 ± 0.4 (range 10–18) and 9.5 ± 0.5 (range 9–12) in the success and failed groups, respectively (p = 0.001). There were no significant differences in age at the time of surgery, height, weight, body mass index and wall defect reconstruction between two groups (Table 1).
Comparison of radiographic parameters between success and failed groups.
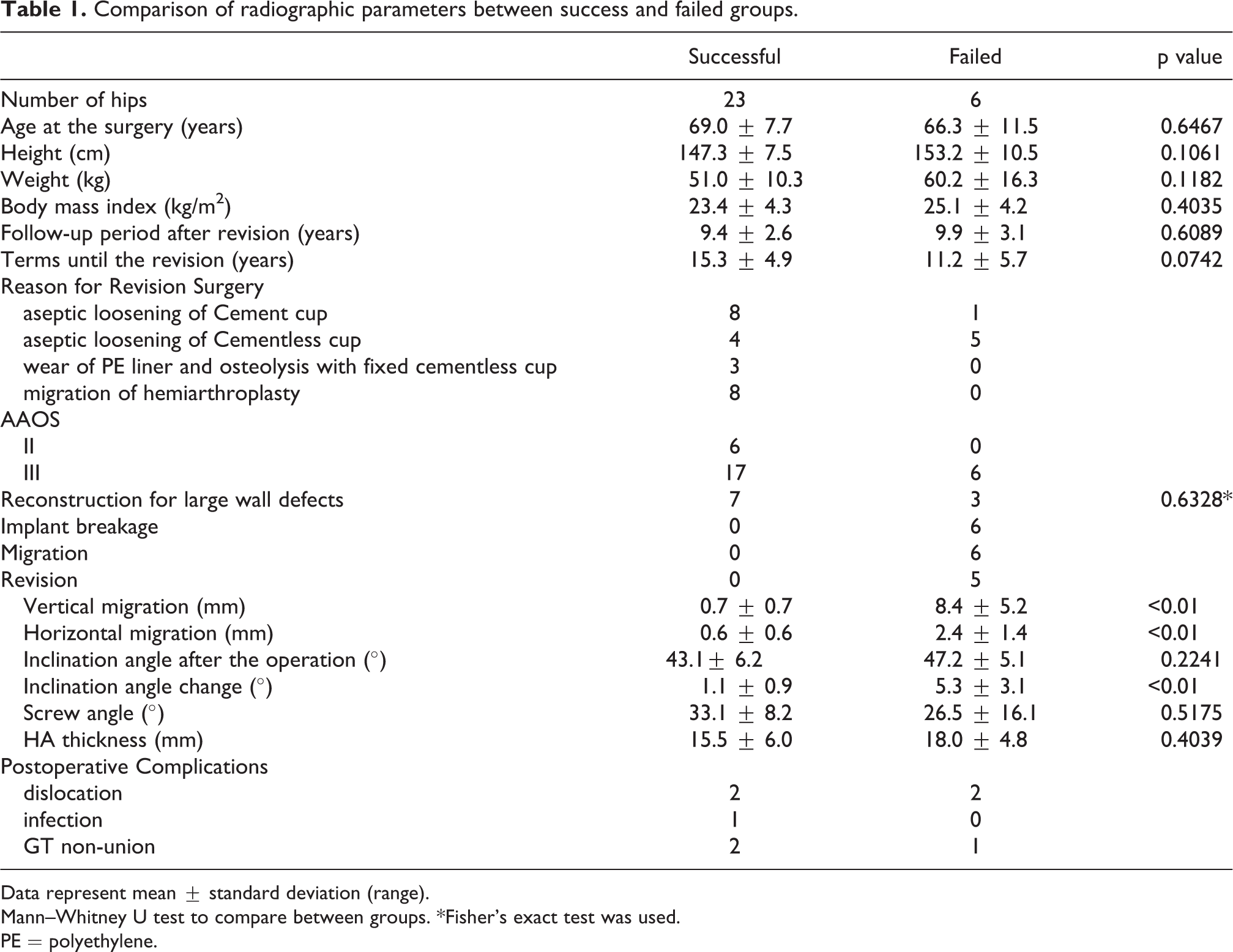
Data represent mean ± standard deviation (range).
Mann–Whitney U test to compare between groups. *Fisher’s exact test was used.
PE = polyethylene.
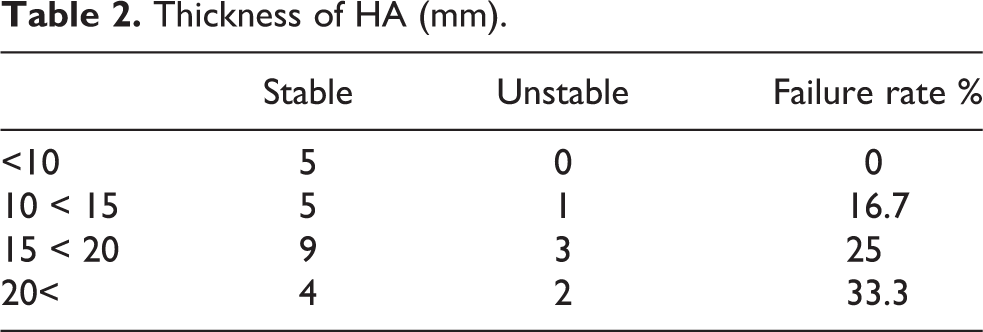
No significant differences in HA thickness, inclination angle after surgery and inserted screw angle were observed between the groups (Table 1). However as the HA became thicker, the failure rate was increased (Table 2). There were significant differences between survival rate and thickness of the grafted HA (hazard ratio, 1.191; 95% CI, 1.012–1.403; p = 0.035). There were significant differences in vertical migration, horizontal migration and inclination change (Table 1). Complications occurred in eight cases; four patients suffered postoperative dislocation, one developed a deep infection and three demonstrated greater trochanteric non-union.
Thickness of HA (mm).
The Kaplan–Meier survival rate at 5 years was 93.1% (95% CI, 83.9–100), at 10 years was 73.2% (95% CI, 54.3–92.1) as the end point was failure condition, with 100% and 67.0% (95% CI, 34.7–89.2) at 10 years for AAOS type II defect and AAOS type III defect cases, respectively (Figure 2).
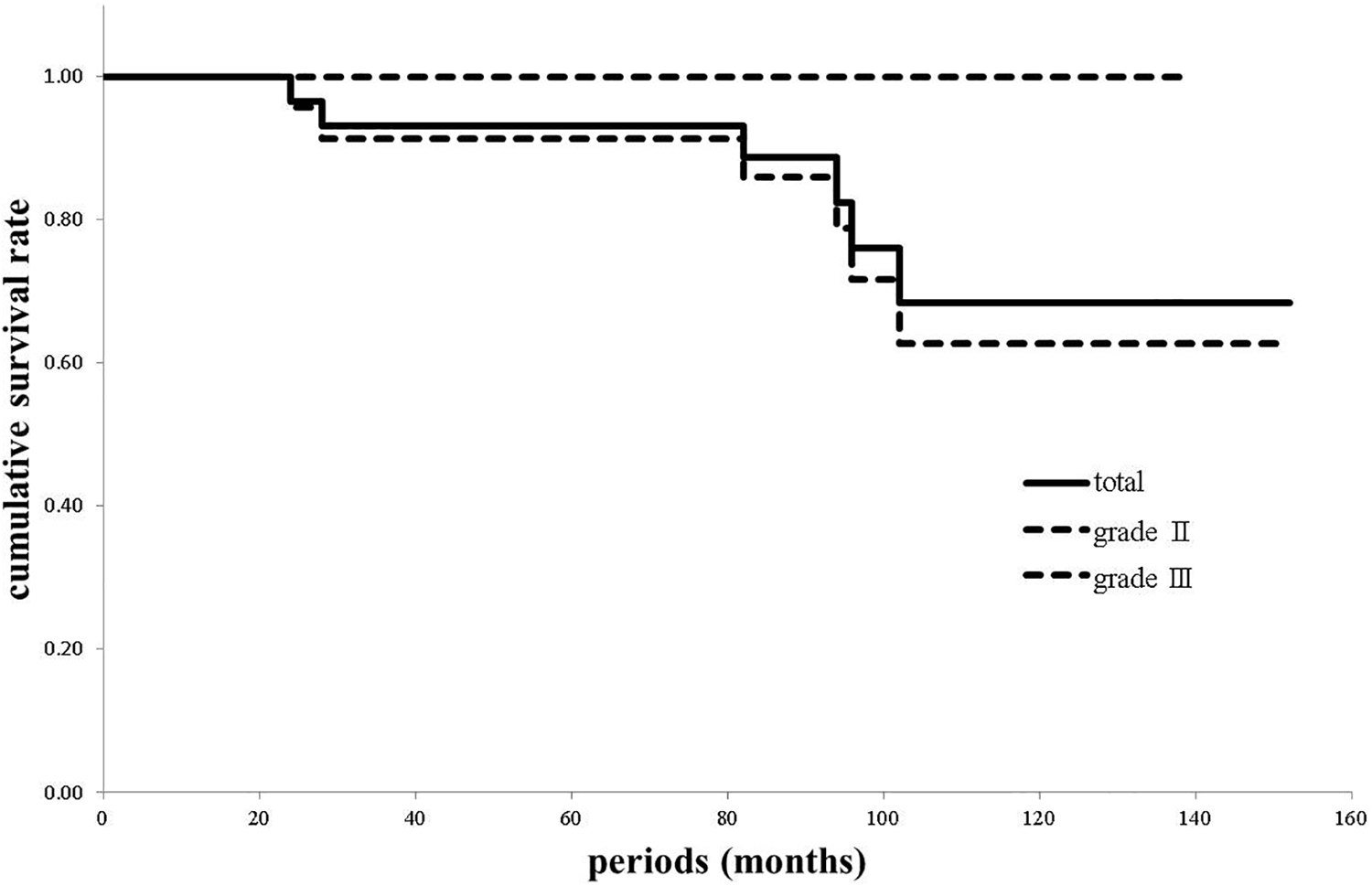
The Kaplan–Meier survival rates with 95% confidence intervals with unstable acetabular joint as the end point.
Discussion
In the present study, the survival rates at 10 years with revision THA using Kerboull cross plates and HA impaction was 73.2% (Figure 2). Kerboull et al. reported the survival rate of hips that were reconstructed with cross plates and structural allografts was 92.1% at 13 years. 12 Several clinical and radiographic studies of acetabular reconstruction using cross plates were reported; the survival rates that were evaluated at 4.9–8.7 years were 53%–82.3% with morselized bone, 13,14,19,22 whereas survival rates evaluated at 6.0–13.0 years were 82–92.3% with bulk bone. 12,14,22 –24 Excellent results were reported with acetabular reconstruction using cross plates with HA impaction, 15 with the 10 year survival rate of 100% in type II defects and 94.9% in type III defects with the end point of joint loosening observed at postoperative 12.8 years. 15
In our cohort, six hips were failed among those with AAOS type III defects. There were no significant differences in inclination angle following surgery and angle of the inserted screw between the groups (Table 1), however, screws were horizontally placed in one of the failed cases (Figure 3), this findings may be one of risk factor. There were no significant differences in HA thickness just after the operation (Table 1). However as the HA became thicker, the failure rate was increased (Table 2) and there were significant differences between survival rate and thickness of the grafted HA. Thicker grafted HA was seemed to be risk factor for implant failure. In several failed cases, scratch marks on implants or plates, which could have arisen from the impingement between the stem neck and cross plate, was noted. Frequent impingement could lead to overload on the implant and HA, leading to implant breakage and loosening.
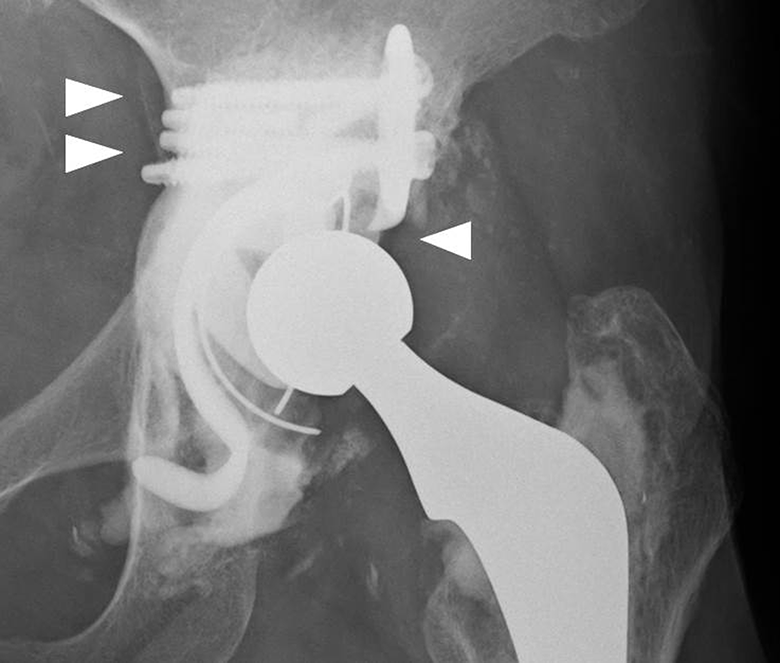
Radiographic images of one of the failed cases. Note the screws that were horizontally placed (arrow) and the fractured and loosened implant.
Three out of six failed cases had diagnoses of RA and ON treated with corticosteroids. In patients with RA or those treated with corticosteroids, the quality of bone is poor, and these patients are at an increased risk for osteoporotic fractures. Thus, in these patients, micro compression of acetabular bone without loosening of HA granules might have led to failure. Thus, in RA patients, a delay in full weight-bearing should be considered. 22
Further acetabular revision was performed in five out of six cases. The grafted HA granules were found to be hard, firmly adhering to the acetabular bone during the removal of grafted HA granules for re-reconstruction of the acetabulum. The ability to reconstitute bone stock is a major advantage of bone graft over substitutes like HA. The grafted HA granules did not reconstitute bone in a similar way to autograft/allograft. It is difficult to remove, chisel and reamer were used to break the grafted HA material, which was removed until the bleeding from acetabulum was found. In these cases, concerns remained regarding further bone loss that might have occurred because of the curettage.
In conclusion the reconstruction technique using a Kerboull-type acetabular reinforcement device with HA impaction was used as an alternative method in the absence of adequate allografts. Our experience suggested association between HA thickness and failure rate using this approach and the Kerboull-type acetabular reinforcement device with hydroxyapatite impaction is associate with higher failure rate in AAOS type III defects.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.