
Abstract
Introduction
Fracture-related infections (FRI) add insult to injury in delivering a second hit to trauma patients. A challenge even to experienced trauma surgeons, fracture-related infections call upon multidisciplinary management in addressing multiple facets including patient factors, fracture considerations of mechanical stability and biological viability, and pathogenicity of the infecting organism. 1 An understanding of fracture-related infection clinical outcomes including mortality empowers better-informed decision making, prognostication, and formulation of realistic treatment plans. Literature reports on fracture-related infection mortality are focused on postoperative infection rather than infection of the fracture site,2,3 or put exclusive emphasis on hip fractures4,5 where high prevalence of medical comorbidities may confound mortality analysis. In this study, we aim to identify survivorship, healthcare-associated, and serological outcomes of fracture-related infection patients, and hypothesise that non-antibiotic-resistant organisms, superficial, or early FRIs are associated with better survival.
Materials and methods
This retrospective study was conducted at a university-affiliated hospital which served as a designated trauma referral centre. Ethics approval was obtained from the institutional review board (reference number UW 21–422). Patients with suspicion of infection after fracture osteosynthesis between 2001 and 2020 were screened for inclusion. Such patients were identified through data queries of fracture fixation surgeries from the digital medical record database with International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) procedural codes of 79. This preliminary list was cross-referenced against diagnoses of postoperative infection (ICD-9-CM 958.3, 996.67, 996.78, 998.59), postoperative debridement procedures (ICD-9-CM 78.6, 79.6, 86.04, 86.22), or postoperative positive microbiological culture of bone, tissue, wound swab or fluid specimens. Fracture-related infection was defined per the 2018 international expert group consensus. 6 Patients with pathological fractures, peri-prosthetic fractures, or follow-up less than 1 year from diagnosis of FRI were excluded.
Patient demographics (age, sex), socioeconomic factors (nursing home residency, receipt of public financial assistance as reflected by hospital pay code), medical comorbidities (diabetes mellitus, Charlson comorbidity index), and serological parameters (C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), white cell count) were recorded.
Fracture-related infections were stratified according to organism involved, depth of infection, and temporality. Deep infections were defined as presence of infective material in communication with fracture site, implant, or bone; superficial infections were limited to subcutaneous tissue above the fascial layer.
After consensus-building sessions to ensure uniformity of case definition, all medical records including free-text entries were examined by two assessors to confirm validity of FRI diagnosis and study parameters, with the addition of a third assessor in the event of disagreement.
Primary outcome involved 1-year mortality of fracture-related infection patients, and differences in survivorships among different stratifications of fracture-related infection. Number of subsequent orthopaedic procedures (debridement alone or implant removal), length of hospital stay, number of outpatient attendances including clinic follow-up visits, duration of antibiotic therapy, analgesic requirement, and serological inflammatory markers including C-reactive protein, erythrocyte sedimentation rate, and white cell count were also included. Exploratory analyses included potential correlation between age and infection, and associations between management and survivorship.
Statistical analysis was performed using R Statistical Software version 4.0.3. Multivariable survival analysis was done on different stratifications of FRI by organism involved, depth of infection, and temporality. Cox proportional hazards model with adjustment of confounders was performed. Bonferroni correction was used to adjust for multiple statistical testing, with statistical significance set at p < 0.0167.
Results
Cross-mapping of 24,841 database records yielded 436 potentially eligible subjects. Upon manual scrutiny of individual patient medical records with application of inclusion and exclusion criteria, 311 fulfilled the study protocol and were included in analysis (Figure 1). Study flowchart.
Baseline characteristics.

FRI pathology and stratification.

Relationship between age and infection.

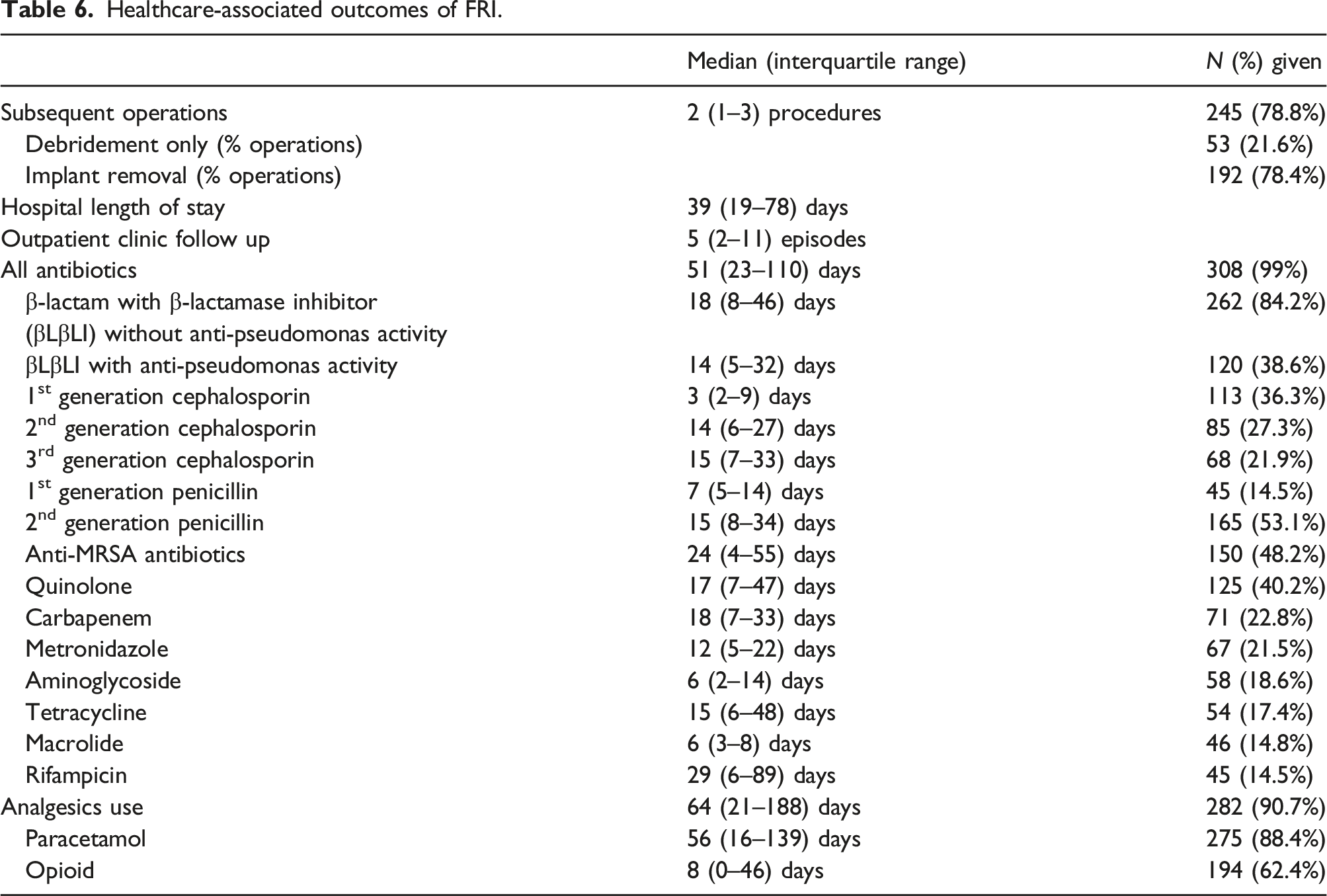
FRI were primarily managed operatively in 245 (78.8%) patients. Among these patients who received surgery, 211 (86.1%) were treated with primary wound closure after debridement, wounds were laid open in 20 (9.5%), and negative pressure dressings applied in 14 (6.6%).
FRI outcome – mortality.


(a) 1-year survivorship of fracture-related infection patients. (b) Survivorship of fracture-related infection patients in the study cohort.
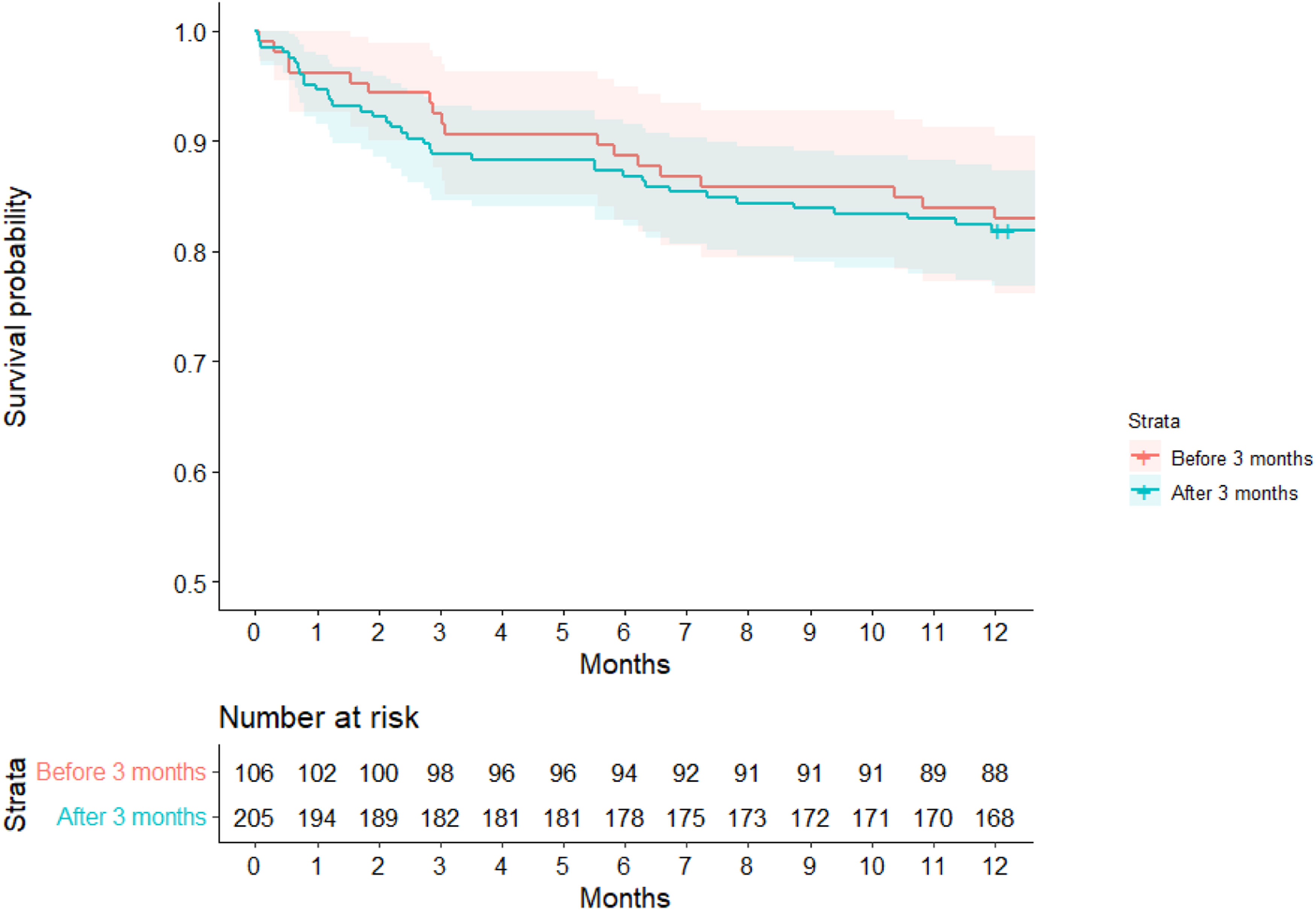
Multivariable analysis with Cox proportional hazards model with adjustment of confounders showed that FRIs caused by MSSA were associated with better survival then non-MSSA FRIs (adjusted hazards ratio 0.34, 95%CI 0.15–0.76, p = 0.008), which remained statistically significant after Bonferroni correction (Figure 3). Culture-negative FRIs were associated with improved survival (adj HR 0.40, 95%CI 0.17–0.97, p = 0.039), although it did not reach statistical significance upon adjustment for multiple testing (Table 5). There was no difference in survival between superficial or deep fracture-related infections (adjusted hazards ratio 0.86, 95%CI 0.62–1.19, p = 0.353) (Figure 4). There was no association between time of onset of FRI with survivorship (adjusted hazards ratio 1.0, 95%CI 0.99–1.00, p = 0.943) (Figure 5). Survivorship among fracture-related infections caused by methicillin-sensitive Staphylococcus aureus (MSSA) versus non-MSSA FRIs. FRI mortality associations. *Statistically significant after Bonferroni correction for multiple statistical testing. Survivorship between superficial and deep fracture-related infections. Survivorship between fracture-related infections presenting within and beyond 3 months of index fracture fixation surgery.


Healthcare-associated outcomes of FRI.
With regards to serological outcomes, CRP and ESR were elevated in 81.7% and 81.5% of fracture-related infection patients respectively. In contrast, an elevated white cell count was only observed in 35.9% patients. CRP normalised in 70.3% patients at a median of 46 days, while normalisation of ESR was observed in 53.8% patients at a median of 86 days (Figure 6) (Table 7). Proportion of fracture-related infection patients with elevated inflammatory markers over time. Serological outcomes of FRI.

Discussion
Fracture-related infections are associated with significant mortality, on par with fragility hip fractures. 7 Although the argument could be made that a proportion of patients were hip fracture patients, the median Charlson comorbidity score of our cohort is 0, indicating a low mortality risk prior to FRI. Far from being an afterthought, fracture-related infection is a disease entity in its own right, and should be accorded high vigilance to facilitate prompt diagnosis and management for minimising treatment failure risk. Inclusion of nuclear imaging (fluorodeoxyglucose positron emission tomography, white blood cell scintigraphy, single photon emission computed tomography) and histopathological (in chronic or late-onset cases) findings in the FRI diagnostic pathway further adds to the armamentarium in diagnosis. 8
Fracture-related infections caused by methicillin-sensitive Staphylococcus aureus, the commonest cause for FRIs in our cohort, were associated with lower mortality. This could be a result of greater availability of effective antibiotic drug options that do not require prolonged intravenous administration with associated in-hospital stay, and more favourable side effect profile (cf. risk of renal failure and need for serum drug level monitoring in the case of vancomycin). Failure to culture organisms on microbiological specimens in culture-negative FRIs could be an indirect reflection of low bacterial loads or effective antibiotic treatment, with subsequent association with better survival observed – statistical significance was nevertheless lost upon more stringent Bonferroni correction. Our results indicate that in addition to guiding antibiotic management, culture and sensitivity results could play a role in prognostication. All FRI patients should be managed with great care; specifically, patients with samples yielding MRSA, Enterobacterales, or organisms other than MSSA should be treated with extra caution due to their association with inferior outcomes. Patients could be counselled accordingly, and in frail elderly patients, realistic treatment goals could be formulated on the basis of better-informed decision making.
In the absence of established sub-classification criteria, attempts were made at stratifying fracture-related infections by depth of involvement and temporality. Despite ultimately proven in vain with no statistically significant difference in mortality among subgroups, the alarming observation remains that superficial and early infections do not confer survival benefit in FRI, and should be managed with the same gravitas as deep and late presenting infections.
Even when the FRI patient survives, prognosis is marred by long duration of hospital stay, subsequent procedures, and prolonged antimicrobial chemotherapy. Not only are patients’ well-being, work capacity, and quality of life 9 in jeopardy, publicly financed healthcare systems tasked with managing FRI patients (as in the case of the study site) are incurred additional manpower and resources in terms of acute hospital bed occupancy, operative theatre slots, investigative and treatment expenditure, with costs reported to be 6.5 times higher than managing non-infected counterparts. 10 This highlights the importance of prompt investigation and development of a multidisciplinary treatment (MDT) strategy at the outset.8,11 Treatment principles as outlined by Metsemakers et al. 11 involve preoperative medical and nutrition optimisation, attention to fracture stability, thorough debridement with low pressure irrigation of sufficient amount of normal saline, local antibiotic application, soft tissue coverage, and follow-up of at least 12 months.
Our results on serological outcomes confirm that normalisation of ESR takes a longer time than CRP in orthopaedic infections. 12 The observation that over half of fracture-related infection patients presented with normal white cell counts caution against its use as a diagnostic marker for FRI, in view of its low sensitivity leading to false negative results, potentially delaying diagnosis and treatment. This echoes similar findings by Govaert et al. 8 and Sigmund et al. 13
Strengths of our study include long duration of follow up, access to survivorship data linked to the government death registry allowing acknowledgement of out-of-hospital mortality, and data quality made possible by access to free-text medical record entries and manual checking by 2 independent assessors to correct for miscoding errors. Limitations in functional assessment of quality of life measures were a result of lack of standardised patient outcome measures for FRI, 11 fracture heterogeneity, and the study’s retrospective nature. In future, we look forward to validated instruments of patient-reported outcomes measurement information systems, by nature of in-person or virtual follow up, to allow comprehensive assessment of patient outcomes.
Conclusion
Fracture-related infections are associated with significant mortality, especially in cases where organisms other than methicillin-sensitive Staphylococcus aureus are involved, regardless of depth and temporality. Remedial surgical procedures, prolonged hospitalisation, long duration of antibiotics and protracted elevation of inflammatory markers were observed. Appreciation of its impact on mortality and morbidity should alert clinicians and patients to potential adverse outcomes, inform prognostication, and guide clinical decision making.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.