
Abstract
Purpose
Fracture-related infections are difficult to treat because of the formation of biofilms around implants. Systemic antibiotics are notoriously ineffective against biofilms due to their insufficient penetration of tissues with poor vascularity. The goal of treating fracture-related infections is to achieve bone union while retaining the implant. Our proposal of continuous local antibiotic perfusion is a sustained local delivery system of sufficient antibiotics to bone and soft tissue infection sites, including to bone marrow via needles as intra-medullary antibiotics perfusion and to soft-tissue via double-lumen subcutaneous tubes as intra-soft tissue perfusion.
Methods
In this study, we examined the outcomes of 40 patients treated for fracture-related infections using continuous local antibiotic perfusion between 2015 and 2021 at Steel Memorial Hirohata Hospital, Himeji, Japan.
Result
The antibiotic used for continuous local antibiotic perfusion was gentamicin in all cases. Implant removal was required in five patients. Two patients required toe amputation and knee arthrodesis, while the remaining 38 patients achieved fracture union. Only one case of transient acute renal injury as a systemic side effect was observed, but it soon resolved. The blood concentration of gentamicin could be adjusted to less than the trough level.
Conclusions
Continuous local antibiotic perfusion is a novel local drug delivery system that has the potential of delivering sufficient concentrations of antibiotics with few systemic side effects; it is a useful option for the treatment of fracture-related infections.
Keywords
Introduction
Fracture-related infections (FRIs) following osteosynthesis are usually challenging to treat because the goals of infection control and fracture healing must be pursued concurrently. 1 This is because there are dead cavities and hematomas around the fracture site that prevent intravenous antibiotics from achieving sufficient concentrations there. Bacteria also form biofilms, which are highly resistant to antibiotics,2–4 around implants and tissues with poor blood flow, making it difficult to control infections without removing such tissue. Generally, the priority during treatment is eliminating the infection through complete debridement of the affected bone, muscle, and soft tissue; implants are removed, if necessary,5,6 although this reduces the stability of the fracture site. Therefore, it would be ideal to retain implants while treating FRIs. However, the antibiotic concentration required to eradicate biofilms—the minimum biofilm eradication concentration (MBEC)—is much higher than the minimum inhibitory concentration (MIC).7–9 Achieving the MBEC locally via intravenous infusion is impossible due to systemic complications. In addition, in most FRIs, the infection spreads to the bone marrow and surrounding soft tissue, necessitating parallel treatment of soft tissue infection.
We propose continuous local antibiotics perfusion (CLAP) as a therapeutic concept for the sustained local delivery of antibiotics to infected bone and soft-tissue; local administration procedures were termed “intra-medullary antibiotic perfusion” (iMAP) for the bone marrow and “intra-soft tissue antibiotic perfusion” (iSAP) for soft-tissues. In iMAP, a daily dose of antibiotics is diluted with a small amount of saline and continuously infused at a low rate using a bone marrow needle placed near the infected site, allowing the delivery of a sufficient local concentration of the agent. 10 In iSAP, double-lumen tubes for injection and drainage are placed in the soft tissue surrounding the focus of infection; an antibiotic is administered at the same dose as that in iMAP via one of the tubes, and constant negative pressure is applied by the other tube to create a perfusion route for the antibiotic. A combination of iMAP and iSAP allows the antibiotic to infiltrate both the affected bone and surrounding soft tissue due to the assistance of negative pressure. It is then drained via the iSAP drainage tube. iMAP and iSAP could be used in isolation or in combination.
We believe that the combined use of iMAP and iSAP creates a continuous antibiotic perfusion pathway in which antibiotics administered via bone marrow needles or double-lumen tubes infiltrate infected areas and are promptly drained via drainage tubes. This pathway enables targeted antibiotic delivery while preventing the unnecessary infiltration of the systemic circulation by the agent.
Aminoglycosides reportedly reduce the infection rate in open fractures when administered locally and in combination with systemic antibiotics. 11 We opted for gentamicin as the standard antibiotic in CLAP for the following reasons: First, gentamicin is a bactericidal antibiotic that is also effective against drug-resistant microbes, including methicillin-resistant Staphylococcus aureus (MRSA).12,13 Second, gentamicin is more effective against biofilms than most antibiotics. 7 Third, the blood concentration of gentamicin is easy to monitor during CLAP and in clinical practice.
This study aimed to evaluate the utility of CLAP by reporting the outcomes of patients with FRIs who were treated with CLAP.
Materials and methods
Participants
Patients with FRIs were diagnosed when there was purulent discharge from a fistula or clinical signs of deep infection confirmed by the presence of pus that excluded superficial infection in isolation. 1 Cases of FRIs treated using CLAP from 2015 to 2021 that met the following criteria were included in this study: 1) availability of the blood antibiotic concentration as a safety indicator and local antibiotic concentration as an indicator of whether antibiotics were properly administered and 2) a postoperative follow-up period of at least 6 months.
This study was approved by the appropriate institutional review board (approval number: ****). Informed written consent was obtained from all patients whose clinical course or images have been presented in this manuscript.
Data collection
Data collected included patients’ age and sex, location and date of injury, presence of open fracture, type of fixation, time of onset of infection [early (<2 weeks), delayed (2–10 weeks), and late (>10 weeks)], 14 date of CLAP initiation, presence of steroid medication, presence of diabetes, presence of renal dysfunction [glomerular filtration rate (GFR) < 60 mL/min/1.73 m2 for more than 3 months (GFR category G3a–G5)], 15 American Society of Anesthesiologists (ASA) classification, 16 and time to latest follow-up visit.
The following treatment-related factors were also investigated: duration of systemic antibiotics use, duration and number of iMAP and iSAP implantations, respectively, and use of negative pressure wound therapy (NPWT). The efficacy endpoints of CLAP were the local concentration, time to normalization of biochemical signs of infection (raised white blood cell [WBC] count and C-reactive protein [CRP] levels in blood), presence of unscheduled surgical treatment such as amputation, recurrence of deep infection, and whether the implant could be retained. The fluid in the drainage tube was collected, and the antibiotics concentration was measured for 12 h as a reference for the local antibiotics’ concentration. The safety endpoints were the fracture union rate, time to fracture union, maximum serum concentration of gentamicin, presence of acute kidney injury (AKI) after initiation of CLAP based on the KDIGO classification, 15 presence of eighth cranial nerve palsy, and presence of an allergic reaction. Fracture union was assessed using radiographs. In patients with AKI, the time to recovery of renal function (the time until no longer classifiable by KDIGO) was also investigated.
Intra-medullary antibiotic perfusion
The iMAP technique, as previously reported,
10
is depicted in Figure 1(a). During plate fixation, the needle was inserted 2–3 cm away from the edge of the plate; it was inserted into the diaphysis of the bone along the nail, during intramedullary nail fixation. Next, we visually checked that the saline solution flushed from the needle flowed out of the fracture site (flow test). If this circulation pathway was not confirmed, we repeated the flow test (until the pathway was established) by changing insertion positions and needle depths or by creating perfusion routes using K-wires or drills. After verifying the pathway using the flow test, an iSAP tube was placed at the site of the lesion. Intramedullary antibiotics perfusion (iMAP). (a) One of two iMAP pins are inserted near the fracture site in the bone, and a small amount of highly concentrated antibiotic solution is continuously infused using a syringe pump. The injected agent penetrates around the infected lesion through the intramedullary cavity (yellow circle). The leachate is drained via a drainage tube. The yellow arrow indicates the inflow route of the antibiotic, and the red arrow indicates the outflow route of the leachate. (b) Appearance of an iMAP pin: 3 mm, 4 mm, and 5 mm diameter with 9 cm, 10 cm, and 11 cm lengths respectively. (c) Profile of an iMAP pin. This pin has a threaded tip and is fixed to the contralateral cortical bone. The injected agent passes through the pin due to its hollow structure and is delivered into the intramedullary cavity via a hole in the side. The dotted blue arrow indicates the inflow route of the antibiotic.
The Tohoku University-style bone marrow puncture needle (Senko Medical Instrument Manufacturing, Tokyo) was previously used to inject antibiotics into the bone marrow, but its structure, which consists of an inner and outer tube, allowed leakage of antibiotics from the injection site due to loosening; the needle was also dislodged in some cases. In addition, there was insufficient anchoring strength owing to the nature of the needle attachment. Having to constantly lay in bed is detrimental to the mental health of patients and affects their ability to perform daily activities. We developed the iMAP pin (Cubex Medical, Tokyo, Japan) to address these issues (insert Figure 1(b)). After pre-drilling into the contralateral cortical bone, the iMAP pin is inserted using a screwdriver. This pin has a threaded tip, allowing fixation to the contralateral cortex, thus increasing the anchoring stability. The iMAP pin is designed to allow antibiotics from the syringe pump to pass through its hollow core and enter the bone marrow via holes in both sides of the threaded part (insert Figure 1(c)). This custom pin solves the problems of leakage and dropout, as well as patient discomfort. The three variable sizes of iMAP pins (i.e. diameter of 3 mm, 4 mm, and 5 mm and lengths of 9 cm, 10 cm, and 11 cm, respectively) should be selected depending on the bone size.
Intra-soft tissue antibiotics perfusion
The iSAP technique (insert Figure 2) involves continuous infusion of antibiotics into soft tissues and aspiration of the infused antibiotic solution, blood, and effusion fluid via drainage tubes to establish a perfusion pathway at the infection focus. Prior to inserting the drainage tube, dead cavities are identified, after which an entry hole is made 5 cm from the margin of the dead cavity, and the drainage tube is introduced through this hole to infuse the dead space. If one tube is not sufficient for draining the dead space, more tubes are added to ensure complete drainage. Gentamicin is administered via the infusion tube, and continuous negative pressure is applied via the drainage tube (insert Figure 2(a)). Intra-soft tissue antibiotic perfusion (iSAP). The yellow arrow indicates the inflow route of the agents, and the red arrow indicates the outflow route of the leachate. (a) A representative diagram of iSAP. (b) A schema of the double-lumen tube. The tube has a two-lumen structure, with gentamicin injected from one side and leachate collected from the other side. (c) Combination of iSAP and NPWT using a Y-shaped connector.
Initially, only one injection tube and one drainage tube were used; however, due to the distance between the two tubes, the infused fluid was not collected by the drainage tube, and they were often blocked by hematomas or soft tissues. Therefore, we started using a double-lumen Salem sump tube (Japan Covidien, Tokyo) >20 Fr in diameter as the iSAP tube. Infusion was performed via the outer lumen and aspiration via the main lumen (insert Figure 2(b)); this reduced the incidence of obstructions. 17 When a wound was difficult to close, NPWT was administered using a RENASYS (Smith and Nephew Japan, Tokyo, Japan) device. This facilitated efficient effusion fluid collection due to the negative pressure generated in the iSAP tube by NPWT. This was achieved by connecting the drainage circuits with a Y-shaped connector (insert Figure 2(C)). NPWT was used continuously, with a negative pressure of 60 mmHg.
Antibiotic Regimen
Regarding local antibiotic administration, gentamicin was administered through the iMAP pin and double-lumen Salem sump tube, with the dose strictly controlled by a syringe pump. Treatment began with 1.2 mg/mL as the standard dose and 2 mL/h as the rate of solution infusion. During this period, the blood and leachate concentrations of gentamicin were measured twice a week. The rate of nephrotoxicity increases when the serum trough concentration of gentamicin is >2 μg/mL and the maximal serum concentration is >10 μg/mL. 18 Thus, the target gentamicin concentration was <2 μg/mL; if the concentration exceeded 1 μg/mL, the dose was lowered accordingly. If the concentration of the leachate fluid was low, the circuit was checked for abnormalities such as blockages and leaks.
Continuous local antibiotics perfusion is always used in combination with intravenous administration of systemic antibiotics. The choice of antibiotic and its duration of use were based on the recommendations of a group of FRI experts. When the pathogen was known, antibiotics were chosen based on pathogen susceptibility; otherwise, empirical therapy was initiated (consisting of sulbactam/ampicillin or cefazolin) and switched to pathogen-specific antibiotics as soon as the pathogen was identified. Parallel to CLAP, systemic antibiotics were continued for 4–6 weeks and then switched to oral antibiotics for several months.14,19,20
Treatment of fracture-related infections with a combination of intra-medullary antibiotic perfusion and intra-soft tissue antibiotic perfusion using continuous local antibiotics perfusion
Fracture-related infections were treated with a combination of iMAP and iSAP using CLAP. Once an FRI was diagnosed using the aforementioned criteria,
1
surgery to set up iMAP and iSAP was performed as soon as possible to prevent deep infection. It was postulated that fracture stability by internal fixation was essential for infection eradication; therefore, implants already in place were retained. Loosened implants or inadequately reduced fractures were addressed using single- or double-stage surgery. As shown in Figure 3, the combination of iMAP and iSAP completed the perfusion pathway in which the administered agent was infused throughout the infected lesion and then discharged via the tubes. The iMAP pin and double-lumen tube were withdrawn when local and hematological findings suggested resolution of the infection—a decrease in blood CRP levels was used as the first indicator, which was confirmed using local findings. Combination of iMAP and iSAP. A combination of iMAP and iSAP enables the efficient distribution of antibiotics in the bone marrow and soft tissues around the fracture site. It is now possible to aspirate hematomas and necrotic tissue that interfere with treatment; the swelling reduces rapidly. The leachate is collected from a drainage bottle, and the concentration of antibiotics is measured. The dosage of the agent is adjusted based on the results. The yellow arrow indicates the inflow route of the agents, and the red arrow indicates the outflow route of the leachate.
Results
Patient background
Data from 40 patients (28 men, 12 women) were included in this study. The mean age at the time of operation for the fracture was 60.5 (range, 17–98) years, and the mean follow-up period was 696.4 (range, 190–2231) days. Locations of injury were the tibia (n = 17), humerus (n = 6), patella (n = 3), pelvis (n = 3), radius (n = 2), femur (n = 2), calcaneus (n = 2), metatarsals (n = 2), ulna (n = 1), proximal phalanx (n = 1), and vertebra (n = 1; insert Figure 4(a)). 11 cases of open fractures were observed (Gustilo Anderson classification Type I, one case; Type Ⅱ, one case; Type Ⅲa, eight cases; and Type Ⅲb, one case). The method of osteosynthesis used was plating in 18 cases, intramedullary nailing in seven cases, screwing in eight cases, and others in seven cases (insert Figure 4(b)). Deep infections developed an average of 172.1 (range, 4–2042) days after the first internal fixation procedure, and CLAP was initiated upon diagnosis. Regarding infections, four cases (10%) were early, 15 (37.5%) were delayed, and 21 (52.5%) were late. The causative organisms were methicillin-susceptible Staphylococcus aureus (MSSA; n = 12), MRSA (n = 7), methicillin-resistant coagulase negative staphylococci (MRCNS; n = 4), Escherichia coli (n = 3), Corynebacterium sp (n = 2), Klebsiella pneumoniae (n = 2), others (n = 4), and unknown (n = 6; insert Figure 4(c)). Of the 40 patients, one was treated with steroids, nine had diabetes mellitus, and 11 had renal dysfunction. The ASA-PS classification was class 1 in 19 cases, class 2 in 20 cases, and class 3 in one case (insert Figure 4(d)). Patient characteristics. (a) Location of injury. (b) Type of fixation for ORIF. (c) Causative organism (d) ASA-PS classification.
Treatment background
Regarding treatment, 12 patients were treated with iMAP alone, 11 were treated with iSAP alone, and 17 were treated with a combination of both. Gentamicin was used as the antibiotic in all cases. An average of 1.41 iMAP pins (range, 1–2) and 1.25 tubes for iSAP (range, 1–2) were used. The mean CLAP treatment periods were 13.9 (range, 7–20) days and 14.1 (range, 10–20) days, respectively. NPWT was used concomitantly in 30 cases. Systemic antibiotics were given intravenously for an average of 3.1 (range, 1–13) weeks and then orally for an average of 12 additional (range, 1–52) weeks.
Efficacy evaluation
The mean local concentration of gentamicin was 1634 (range, 125–14,080) μg/ml. The CRP level decreased to <0.3 mg/dL at an average of 15.4 (range, 3–109) days after CLAP initiation. Of the 40 patients, five required implant removal to control the infection, and the implant retention rate after a single CLAP surgery was 87.5%. During the follow-up period, deep infection recurrence was observed in six patients, and CLAP was re-initiated. The infection was controlled in four patients, while one of the remaining two patients required toe amputation and one required knee arthrodesis.
Safety evaluation
Fracture union was achieved in 95% (38 of 40) of cases, and two cases required unscheduled surgical procedures. The mean time required for fracture union was 7.5 (range, 2–24) months. The mean maximum blood concentration of gentamicin was 1.7 (range, 0.3–4.9) μg/ml in patients treated with iMAP alone, 0.4 (range, 0.3–0.6) μg/ml in those treated with iSAP alone, and 1.1 (range, 0.3–2) μg/ml in those treated with a combination of both (insert Figure 5). Complications of AKI classified as KDIGO stage I during CLAP were observed in one patient, but renal function recovered within 6 weeks. There were no cases of eighth cranial nerve palsy or local allergic reactions following the initiation of CLAP. Peak concentration of gentamicin in blood. 12, 11, and 17 patients were treated with iMAP alone, iSAP alone, and a combination of both, respectively. The peak blood concentration of gentamicin (PBCG) exceeds 2 μg/mL in four of the patients treated with iMAP alone. Conversely, in the patients treated with a combination of both iMAP and iSAP, the PBCG does not exceed 2 μg/mL. The red line indicates 2 μg/ml, and the target concentration of gentamicin was adjusted to remain below this limit to avoid side effects.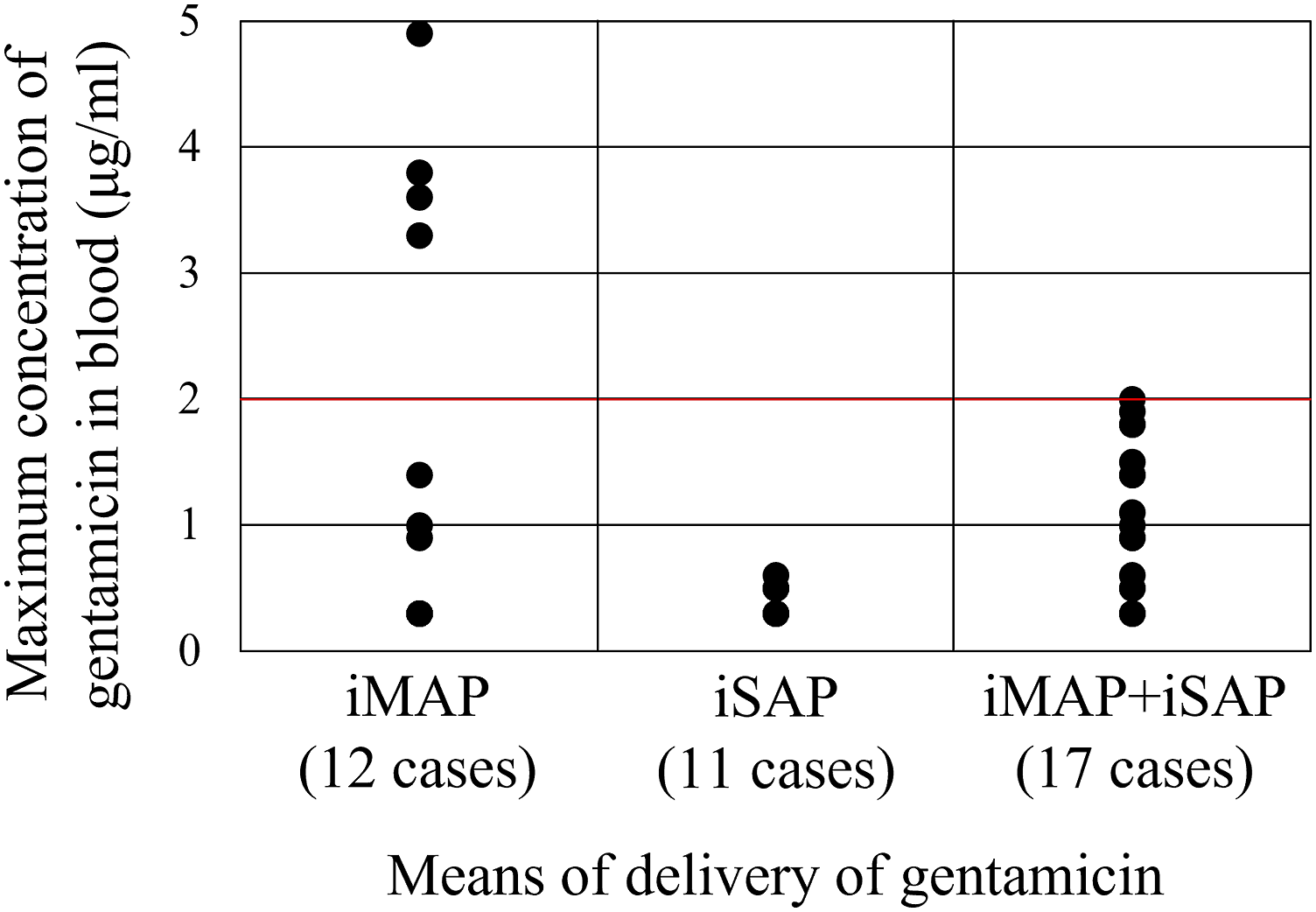
Case presentation
An 87-year-old woman with untreated diabetes mellitus (HbA1c: 9.0%) fell and injured her left hand. She presented with a left, closed, highly comminuted transcondylar distal humeral fracture (insert Figure 6(a)) and was hospitalized on the same day; appropriate glycemic control was achieved prior to surgery. We performed open reduction and internal fixation using dual locking plates and transplanted a bone graft to fill the defect on the 11th day after injury (insert Figure 6(b)). On postoperative day 14, symptoms including fever and swelling and heat around the surgical wound were noted along with purulent discharge from the wound and an increase in blood CRP levels. FRI was diagnosed according to the two major criteria, and surgery was performed the same day. A copious amount of purulent discharge was noticed when pressure was applied around the open wound. Intraoperative findings included a partially ruptured triceps fascia and purulent drainage from the deep elbow joint area, suggesting that the infection had spread into the joint (insert Figure 6(c)). After thorough lavage with a large amount of saline, an iMAP pin was percutaneously inserted in the distal humerus metaphysis where it does not interfere with the double plates. The flow test confirmed proper infiltration of the bone graft and intra-joint space. A subcutaneous dead space was confirmed, and the margins were marked with a surgical pen. A 22 Fr double-lumen tube was inserted into the joint as an iSAP from a position 5 cm from the margin of the dead cavity via the infected lesion. It was then confirmed that the iMAP fluids were drained by the iSAP tube. Using this system, a large amount of saline was used to irrigate the lesion. Another double-lumen tube was introduced into the subcutaneous area of the forearm. As per the standard CLAP protocol, gentamicin (1.2 mg/mL) was infused continuously via one iMAP pin and 2 iSAP tubes at 2 mL/h. The dual plates and bone graft were retained (insert Figure 6(d)). The causative organism was identified as MSSA based on several intraoperative samples. Local findings improved promptly after the initiation of CLAP. The CLAP system was removed 13 days after insertion. During CLAP, there were no findings suggestive of AKI, eighth cranial nerve palsy, or allergic reactions. The maximum blood concentration of gentamicin was 0.5 μg/mL, and the average local concentration was 1427 μg/mL (1040–1700 μg/mL). Gentamicin concentrations recorded in the blood and leachate are shown in Figure 6(e). Intravenous antibiotics were administered for 4 weeks and then replaced with oral antibiotics, which were administered for another 4 weeks. CRP levels, WBC counts, and details of the antibiotics used are shown in Figure 6(f). CRP levels normalized 9 days after the initiation of CLAP. Fracture union was achieved 6 months after surgery (insert Figure 6(g)). No signs of infection recurrence have been observed in the 2 years following surgery. The patient’s elbow range of motion ranged from 30 to 120°, and there were no limitations to her daily activities. Clinical images of a representative case. (a) Radiograph of the patient’s left humerus on arrival. a: Anterior-posterior view, b: lateral view, and c: three-dimensional computerized tomography images. (b) Radiographs of the left humerus immediately after osteosynthesis with dual-locking plates. a: Anterior-posterior view and b: lateral view. (c) Intraoperative findings. a: A large amount of purulent discharge is observed from the open wound (red circle). b: A partial rupture of the fascia (yellow circle) and purulent discharge from the same site (yellow arrow). (d) Clinical image of the CLAP set-up in the patient. a: Intraoperative findings. One iMAP pin and two double-lumen tubes for iSAP are inserted. The yellow arrow indicates the inflow route of the agents, and the red arrow indicates the outflow route of the leachate. b: Radiographs of the left elbow while undergoing treatment with CLAP. (e) Changes in gentamicin concentration during CLAP. The red line shows the concentration of gentamicin in the blood, and the blue line shows its concentration in the leachate. The latter is used as a reference for the local concentration. Both concentrations are maintained within their respective appropriate ranges. (f) The changes in CRP levels and WBC counts, as well as the type, duration, and method of administration of antibiotics used. The continuous line represents the CRP level, and the dotted line represents the WBC count. After CLAP initiation, both levels decrease rapidly. No re-elevation is observed, even after discontinuation of oral medication. (g) Radiographs at 6 months after the injury. Fracture union is achieved. a: Anterior-posterior view and b: lateral view.
Discussion
Implant-associated infections, including prosthetic joint infections (PJIs) and FRIs, are major postoperative complications. However, their treatment strategies differ considerably due to their fundamental characteristics. 20 The goal with PJIs is complete “eradication” of the infection and stable implant retention without recurrence until the end of life. Conversely, the goal with FRIs is bone union with infection “control” until fracture union is complete, following which the implants can be removed. Implant retention is amenable to the goal of fracture union in FRIs; biofilm suppression is essential to achieving this. CLAP is a novel local drug delivery system developed to achieve the goal of retaining implants while controlling infection.
Intra-medullary antibiotic perfusion was previously devised based on the concept of CLAP. 10 Initially, we treated FRIs using a combination of iMAP and a simple drainage tube; however, the tube got occluded in many cases, leading to an increase in the serum concentration of gentamicin. Thereafter, we combined iMAP with a suction system (which also delivered antibiotics to the surrounding soft tissue) to create a comprehensive antibiotic perfusion pathway. In addition, during the typical clinical course of FRIs, superficial surgical site infections progress to deeper layers and cavities surrounding the fracture, which then spread into the bone marrow. 15 Thus, we developed iSAP to have a means of applying suction and administering antibiotics to the surrounding soft tissue. In early infection, the application of iSAP to the superficial layer is enough to control the infection; however, in delayed or late infections, when the infection is assumed to have spread into the bone marrow, an additional application of iMAP is required. We do not use iMAP alone currently because of the possibility of raising blood levels of gentamicin. In summary, we use iSAP alone for early infection and iSAP and iMAP in combination for delayed or late infections. After initiating the concurrent use of iSAP and iMAP, there were no cases where the blood concentration of gentamicin crossed the safety threshold. Thus, the combination of iMAP with iSAP is an effective and ideal therapeutic modality in FRIs and the perfect perfusion system for CLAP.
Negative pressure wound therapy is an effective tool for treating open or difficult-to-close wounds.21–23 The combination of NPWT with the continuous instillation of physiologic saline or antiseptic solution is reportedly effective in the treatment of infected ulcers and bone and soft tissue infections.24–27 The principle behind these treatments is the comprehensive irrigation of the contaminated area followed by the collection of the washing solution using continuous negative pressure. These systems, similar to the iSAP model, are effective in treating superficial open wounds but not in treating deep, closed wounds surrounded by vascular dead spaces. In contrast, in most FRIs, the infected area is substantial at the superficial level and in the muscular layers and bone marrow. We discovered that connecting the suction circuits of an iSAP tube and an NPWT system created a more efficient perfusion pathway for the antibiotic solution, resulting in a more sustainable method of CLAP. If pressure was not maintained due to a leak or obstruction of the CLAP route, the NPWT system alerted us. It also crimps and reduces the dead cavity (where the antibiotic has difficulty reaching) by concurrently suctioning the superficial and deep layers. Thus, we have treated FRIs using a combination of NPWT and CLAP to optimize the local delivery of antibiotics and better manage the surrounding vascular dead space.
AKI and eighth cranial nerve palsy are systemic side effects of gentamicin.28,29 The trough concentration of gentamicin is 2 μg/ml for intra-venous administration; therefore, theoretically, in continuous administration, keeping the concentration under this level will prevent systemic side effects. 18 In this study, there were almost no cases of systemic side effects, which we attribute to continuous monitoring and dosage adjustments based on serum gentamicin levels.
It is also important to maintain an appropriate local concentration of the antibiotic. Exposure to high concentrations of gentamicin does not inhibit the activity or proliferation of osteoblasts and endothelial cells, both of which are essential for fracture union. 30 However, another aminoglycoside (tobramycin) reportedly caused cell death at extremely high concentrations (≥10,000 μg/ml). 31 The MBEC of gentamicin against Staphylococcus aureus is reportedly 64–512 μg/ml,12,30,32 and we believe that it can be safely used if its local concentrations are adjusted to a range that exceeds the MBEC but is below the concentration that results in cytotoxicity. In this study, fracture union was achieved in 95% of the cases, which suggests that the local concentration was maintained within the appropriate range. A major advantage of this method is that the blood and local concentrations of the antibiotic can be adjusted by altering the dosage of the drug being administered.
There are two major methods for the local administration of antibiotics, roughly classified as methods using a carrier and methods not using carriers. An indwelling bone cement, such as polymenthyl methacrylate and calcium sulfate, containing antibiotics is a well-known example of a carrier method. This method requires debridement to allow for the placement and eventual removal of a carrier.33-35 However, with this method, local antibiotic concentrations are one to several times higher than the MIC at 4–6 weeks postoperatively,36–38 and this is far below the concentration required to inhibit biofilm formation. In addition, this range is hypothesized to be the “mutant selection window,” which promotes the growth of resistant bacteria.39–42 Therefore, these methods have limited local antibiotic elution areas and durations. A no-carrier method—the local intra-operative injection of antibiotic solutions—lowers postoperative infection rates.11,43 However, the duration of antibiotic elution is short in this method. 44 Another method of local antibiotic administration, the suction irrigation method, requires a large amount of washing solution, into which it is difficult to mix high concentrations of antibiotics. 18 Therefore, these methods have limitations in terms of their duration and the concentration of antibiotics used. In contrast, CLAP uses a syringe pump that allows the continuous administration of antibiotics at any rate against the intramedullary pressure. In addition, using the pressure gradient created by the combined use of CLAP and NPWT makes it possible to transfer and expand the infiltration range of antibiotics beyond previous limits. These points suggest that CLAP may be more useful than conventional methods for the treatment of FRIs. We are considering the application of this treatment method in PJIs, and we hope to continue research in this avenue.
The limitation of this study is that no cases treated by other methods were included to be used as a comparison group. We understand the importance of having a comparative group comprising FRIs treated with other methods, and we consider this to be a subject for future studies.
Conclusion
In conclusion, CLAP, which can safely deliver antibiotics locally at concentrations unachievable by systemic administration, is an effective treatment method for difficult-to-treat cases of FRIs due to its lack of side effects and proven efficacy.
Footnotes
Authors’ contributions
AM and TO were the major contributors to writing the manuscript. RM, HM1, HM2, TF, KO, RK, and TN conceived the study and were involved in the study design and coordination. All authors read and approved the final version of the manuscript. AM is the guarantor of this work and, as such, had full access to all data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The corresponding author received consultant fees to develop the CLAP system from Cubex Medical. The remaining authors have no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the institutional review board of the Steel Memorial Hirohata Hospital (approval number: H27-0311).
Consent for publication
Patients provided signed informed consent forms regarding the publication of their data and photographs.
Consent to participate
Informed written consent was obtained from all patients whose clinical course or images have been presented in this manuscript.
Availability of data and materials
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.