
Abstract
Purpose
To evaluate the clinical efficacy of using free tissue flap combined with contralateral instep thick plantar skin in reconstructing complex plantar forefoot defects.
Methods
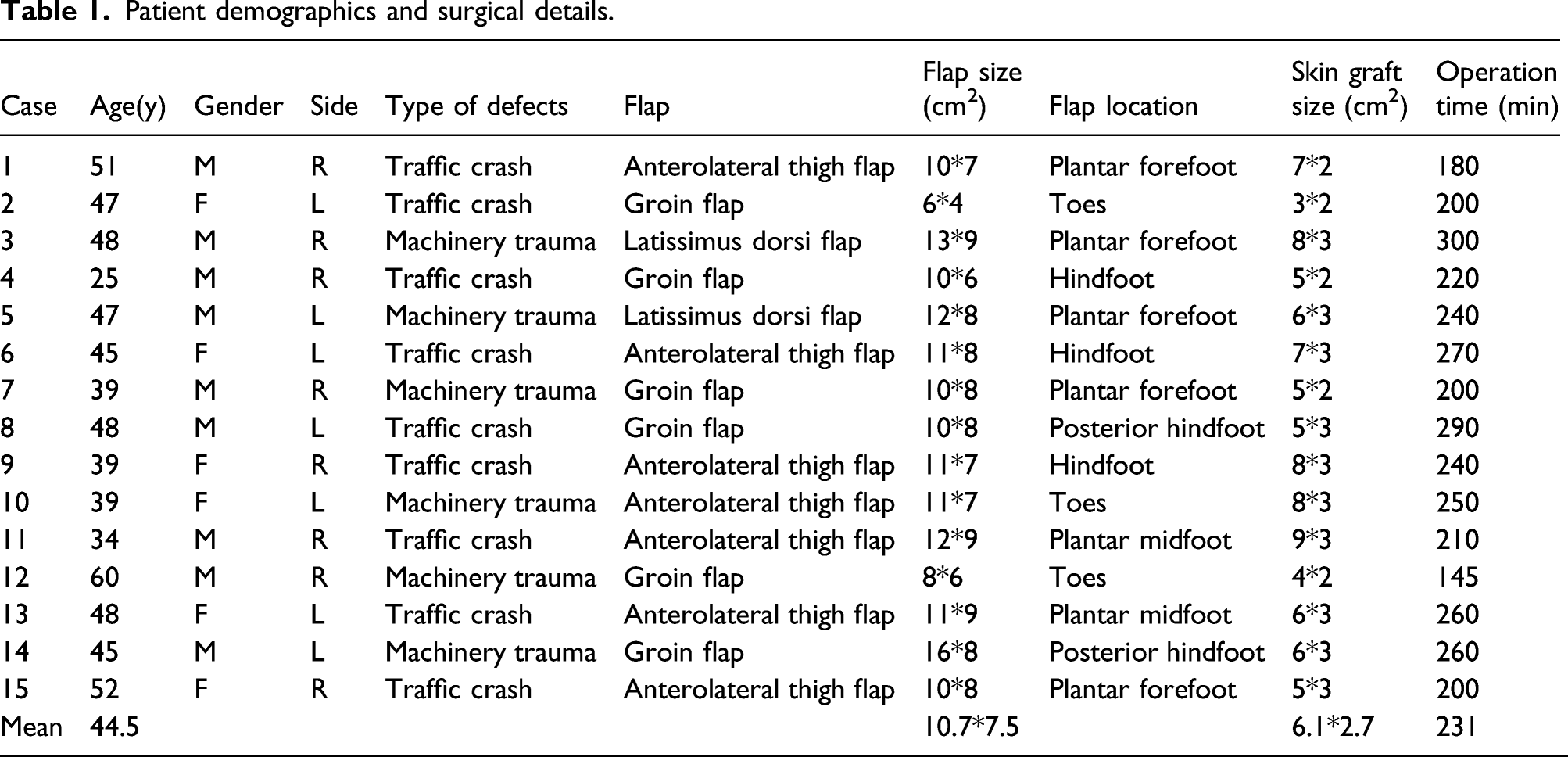
During the past 8 years, 15 patients, aged 25–60 years, with defects in the soft-tissue and composite bone of the forefoot were treated. Their defects were caused by trauma. These defects were all located on the plantar forefoot. The free tissue flaps transposed to reconstruct defects were anterolateral thigh flaps, groin flaps, and latissimus dorsi flaps. Flap size varied in width 4-cm and length (6–16 cm). The mean size of flaps was 80.3 cm2. The follow-up period ranged from 12 to 90 months (mean, 25.5 months).
Results
Partial flap loss was observed in one anterolateral thigh flap and one latissimus dorsi flap. One patient showed skin graft loss at the defect site, and the wound was re-epithelialized by changing dressings. Hyperkeratosis was not observed in any of the cases. All patients were able to walk near-normally within 2.5 months after surgery, and there was no recurrence of ulceration.
Conclusion
We advocate using a free tissue flap combined with contralateral instep thick plantar skin for reconstruction of moderate or large complex plantar forefoot defects.
Introduction
Skin and soft-tissue defects over the weight-bearing plantar foot are most commonly seen in car accidents and machine injuries. Repairing these defects is challenging due to the special characteristics and important role of the foot in weight-bearing and walking. 1 Currently, although there are various methods available, they all have disadvantages. Hence, it is difficult to formulate standard repair principles.2,3 Plantar skin has characteristics that differ from those of skin covering other parts of the body. The medial plantar flap of the foot presents an ideal reserve for reconstructing particular areas that require sensate and glabrous skin. 4 However, the use of this flap is restricted to reconstructing medium and large complex defects, and the free flap alone cannot meet the requirement for long-term walking. 5 Therefore, we first used a free tissue flap combined with contralateral instep thick plantar skin to recover the tendon, nerve, bone, and other important tissues, and also made use of the characteristics of the durable skin to achieve satisfactory outcomes.
This article aimed to assess whether the free flap, combined with contralateral instep thick plantar skin, could be reliably used for reconstruction of the plantar aspect of the forefoot.
Patients and methods
The injured patients underwent thorough debridement and vacuum sealing drainage during emergency surgery. All patients were evaluated preoperatively using multidetector-row computed tomographic angiography (CTA) and Doppler ultrasonography. Before the operation, local inflammation of ulcers was controlled.
We performed three different flap techniques to repair defects in the 15 patients (Mean 44.5 years old): anterolateral thigh flaps (7 patients), groin flaps (6 patients), and latissimus dorsi flaps (2 patient). The free flap size was designed to be slightly larger than the defect. During free flap elevation, the free flap was elevated according to a previously described method.6–9 Of note, at least one cutaneous nerve was preserved and then anastomosed with the cutaneous nerves in the recipient site with micro-sutures. After anastomosis was performed in the recipient area, the weight-bearing site skin of the flap was resected, and then the contralateral instep full-thickness skin graft was used to repair the defect. The flap skin could be used for the second donor site repair only if it could not be sutured directly. Postoperatively, all patients were treated with adequate dosage of intravenous antibiotics (broad-spectrum cephalosporin), subcutaneous heparin (4000 IU, once daily for 3–5 days), and analgesics (oral or IM), as necessary. The external plaster cast was removed a week later, and passive training and postoperative rehabilitation were performed. Stitches were removed 2 weeks postoperatively. Using crutches, the patients were advised to keep the involved leg weight-free for a month. One month later, the patients gradually performed weight-bearing training using orthopedic shoe devices. Strengthening exercises were initiated 6 weeks after surgery.
Results
Patient demographics and surgical details.

(a) and (b) The complex plantar forefoot defects. (c) The defects are resurfaced by free flap. (d) and (e) The weight-bearing site of the free flap is recovered by contralateral instep full-thickness skin graft immediately after the procedure. (f) The shape of the affected sites recovered well by the time of 6 months follow-up.

(a) The complex plantar forefoot defects. (b) The defects are resurfaced by anterolateral thigh free flap and contralateral instep full-thickness skin graft. (c) The shape of the affected sites recovers well by the time of 4 months follow-up.
Discussion
The plantar aspect of the forefoot is an important subunit for weight-bearing and walking. 10 Reconstruction of severe forefoot deformities is a great challenge to microsurgery. In 1987, Stevenson et al. 11 proposed three basic principles for repairing foot injuries: sensation, stability, and satisfactory appearance. Although skin grafts are usually sufficient for reconstructing non-weight-bearing sites, mechanically resistant and sensate local or free flaps are preferred for covering defects of the heel, lateral foot, and plantar forefoot to provide durable coverage. 12 The reverse sural artery, sural artery perforator, and posterior tibial artery perforator flaps are usually sufficient for reconstructing defects of the heel, lateral foot, and plantar forefoot. However, they are limited by functional impairment. 13 Since the application of the medial plantar flap reported by Shanahan in 1979, it has gained increasing attention from clinicians due to several advantages, including consistent vascular anatomy, wear-resistance, and texture similarity. 14 Medial plantar flaps are fasciocutaneous ones from the non-weight-bearing instep area. They can be raised as pedicled flaps, cross-foot flaps, or free flaps. Moreover, they include the same anatomical features unique to the plantar skin, namely, a thin layer of subcutaneous fat and dense fibrous septae anchoring the skin to the underlying fascia. 15 Although medial plantar flaps are regarded as the first choice for heel reconstruction, their use is limited by defect size. 5 The use of free flap transfer for lower extremity reconstruction is particularly useful for large and three-dimensional defects, distal wounds, secondary reconstruction, exposure of vital structures, and osteomyelitis of the foot. Additionally, it is useful due to the possibility of obtaining fine cutaneous sensibility by primary coaptation of the donor nerve. The anterolateral thigh and radial forearm flaps are the most frequently utilized free flaps. 16 Wound healing complications occurred in up to 35% of cases despite long-term follow-up. 1
A key problem is how to obtain a large wear-resistant flap. In our study, we successfully reconstructed large soft-tissue defects in the weight-bearing site of the forefoot in 15 patients. Furthermore, satisfactory outcomes were achieved in a relatively consistent and simple manner. All flaps regained protective sensation, and wearing footwear and weight-bearing were not affected 2 years after surgery. At 90 months follow-up, hyperkeratosis was not observed. However, as with other free flaps, special attention must be paid to several aspects intraoperatively. First, thorough debridement is a key prerequisite for tissue survival by which necrotic and unhealthy tissues should be removed as much as possible. Second, using accurate preoperative perforator mapping by computed tomography angiography and Doppler ultrasound, a targeted perforator flap could be harvested safely and quickly. Third, in cases of extensive vascular contusion, surgeons should not perform suturing in a rapid manner. Fourth, strict surveillance, timely treatment, and systemic postoperative rehabilitation training guarantee a successful operation. The technique described herein has several advantages. First, the skin donor site is located at the non-weight-bearing subunits and could be repaired by direct suture or skin graft, which has little effect on the function and appearance of the contralateral foot. Second, thickness and texture of the skin more closely approximate defects and can provide durable coverage. Third, the design of a free flap is flexible and can meet the needs of various complex wounds.
The study has several limitations: First, this technique might not be suitable in patients who cannot undergo free flap surgery due to many contraindications. Second, there are two donor sites in our procedure which may increase the degree of injury and operation time. Third, a larger sample size is needed to confirm and extend our findings. Fourth, the efficacy of our technique was not assessed by gait analysis preoperatively and postoperatively. Our technique should be established in a larger population to confirm its efficacy and low incidence of complications.
Conclusion
This article demonstrated the versatility of the free flap combined with contralateral instep thick plantar skin. This technique can be an ideal choice for reconstruction of the plantar aspect of the forefoot due to its reliable blood supply and low complications in donor sites.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
The clinical study was approved by the Ethical Committee of our institution, and the patients signed an exhaustive informed consent form after being informed of the benefits and risks of the procedure.