
Abstract
Background
The utilization of all-suture anchors in coracoclavicular (CC) suture fixations offers satisfactory clinical advantages. This study aimed to compare the biomechanical properties of suture looping, conventional metallic anchors, and all-suture anchors in CC suture fixation in a synthetic bone model.
Hypothesis
Suture looping for CC fixation would result in smaller cyclic elongation and greater ultimate pull-out strength than suture anchor techniques.
Methods
A total of 27 composite scapula were divided into three groups: suture looping group (group L), metallic anchor group (group M), and all-suture anchor group (group A). In group L, two No. 2 braided sutures were looped into the coracoid base for CC fixation. In groups M and A, 5.0 mm metallic suture anchors and 2.8 mm all-suture anchors were used, respectively. Prepared specimens were secured using a material testing machine. Each specimen was tested with a preload between 0 and 20 N for 10 cycles, cyclic loading between 20 and 70 N for 1000 cycles, and final loading to failure. Cyclic elongation, linear stiffness, ultimate load, and failure modes were recorded.
Results
All the specimens were subjected to cyclic loading tests. Elongation after cyclic loading in group L (1.0 ± 0.2 mm) was significantly smaller than that in groups M (1.4 ± 0.2 mm) (p = .002) and A (2.5 ± 1.1 mm) (p < .001). Cyclic elongation in group M was also significantly lower than that in group A (p = .004). Ultimate failure load in group L (472 ± 53 N) was significantly greater than that in group M (380 ± 35 N) (p = .002) and A (354 ± 94 N) (p = .010). Suture rupture was the most common failure pattern in group L, whereas two specimens failed because of a coracoid fracture. Both suture rupture and anchor pull-out were common in groups M and A.
Conclusions
The suture looping technique in CC fixation provides a significantly smaller cyclic displacement and greater ultimate failure load than metallic and all-suture anchors. The clinical relevance is that smaller cyclic elongation and greater ultimate failure load imply a reduced risk of fixation construct failure.
Introduction
The coracoclavicular (CC) and acromioclavicular (AC) ligaments are key stabilizers of the AC joint. 1 Hook plate fixation is a common technique for treating acute AC joint dislocation,2–4 with studies showing that adding CC suture augmentation reduces subacromial osteolysis, postoperative pain, and loss of reduction after implant removal.5,6 Similarly, restoring CC ligament function is crucial in distal clavicle fracture treatment.7,8 CC augmentation combined with locking compression plate fixation enhances outcomes and reduces complications in unstable fractures. 8 When using a hook plate for distal clavicle fractures, CC suture fixation provides superior functional results compared to the hook plate alone. 9
With the increasing prevalence of CC suture fixation, there is growing concern regarding iatrogenic anterior deltoid injury. 10 Detachment of the anterior deltoid from the clavicle is typically required for precise insertion of the conventional suture anchor or loop sutures beneath the coracoid process. 10 To mitigate the risk of iatrogenic deltoid detachment, Seo et al. introduced a CC fixation technique utilizing an all-suture anchor with the assistance of a drill handle under fluoroscopic guidance. 10 According to the findings from their postoperative shoulder computed tomography (CT), their technique successfully prevented iatrogenic postoperative deltoid atrophy. 10
Although the utilization of all-suture anchors in CC suture fixations offers satisfactory clinical advantages, concerns about early fixation failure have been raised by findings from a cadaveric study. 11 Hong et al. reported that the fixation construct using all-suture anchors resulted in significantly greater cyclic displacement and smaller ultimate failure load than that of metallic anchors. 11 It is worth noting that the pull-out force of an all-suture anchor is related to the thickness of the cortex, 12 which usually decreases with aging.13,14 Therefore, findings from a previous biomechanical study 11 using cadaveric specimens with a mean age of 67 years cannot be directly applied to young patients with healthy bones. In contrast, although the suture looping technique is common in CC suture fixation, looping the suture under the coracoid process represents the most challenging step in CC stabilization. 15 Using a suture anchor in CC fixation may simplify surgical procedures, 16 but it remains unclear whether CC fixation using a suture anchor achieves stability comparable to that achieved using suture looping.
To overcome the disadvantages of the aforementioned studies, we aimed to compare the biomechanical properties of suture looping, conventional metallic anchors, and all-suture anchors in CC suture fixation in a synthetic bone model. We hypothesized that suture looping for CC fixation would result in smaller cyclic elongation and greater ultimate pull-out strength than suture anchor techniques.
Methods
Experimental specimen
Twenty-seven fourth generation composite scapulae (model 3413; Pacific Research Laboratories, Vashon, WA, USA) were used. Composite bone was chosen because it has been suggested as a reliable substitute for biomechanical testing,17,18 and the composite scapula model has been used in a previous biomechanical study. 19
The specimens were randomly divided into three groups: a suture looping group (group L), metallic anchor group (group M), and all-suture anchor group (group A). In group L, two No. 2 Hi-Fi sutures (ConMed, Utica, NY, USA) were looped to the coracoid base. In group M, a 5.0 mm metallic suture anchor (Super Revo, ConMed, Utica, NY, USA) with double-loaded No. 2 Hi-Fi sutures was inserted into the coracoid base (Figure 1(a)). In group A, a 2.8-mm all-suture anchor (Y-Knot RC, ConMed, Utica, NY, USA) with double-loaded No. 2 Hi-Fi sutures was inserted after pre-drilling in the coracoid base. The anchors were selected according to those used in clinical practice.10,20 The insertion depth of the all-suture anchor was determined based on the manufacturer’s instructions, ensuring that the most distal laser line was positioned below the cortical layer. In all specimens, the soft anchors were located inferior to the coracoid (Figure 1(b)). Illustration of suture anchor insertion into the coracoid base in (a) the metallic anchor group and (b) the all-suture anchor group. The white arrow indicates the bicortical fixation of the all-suture anchor.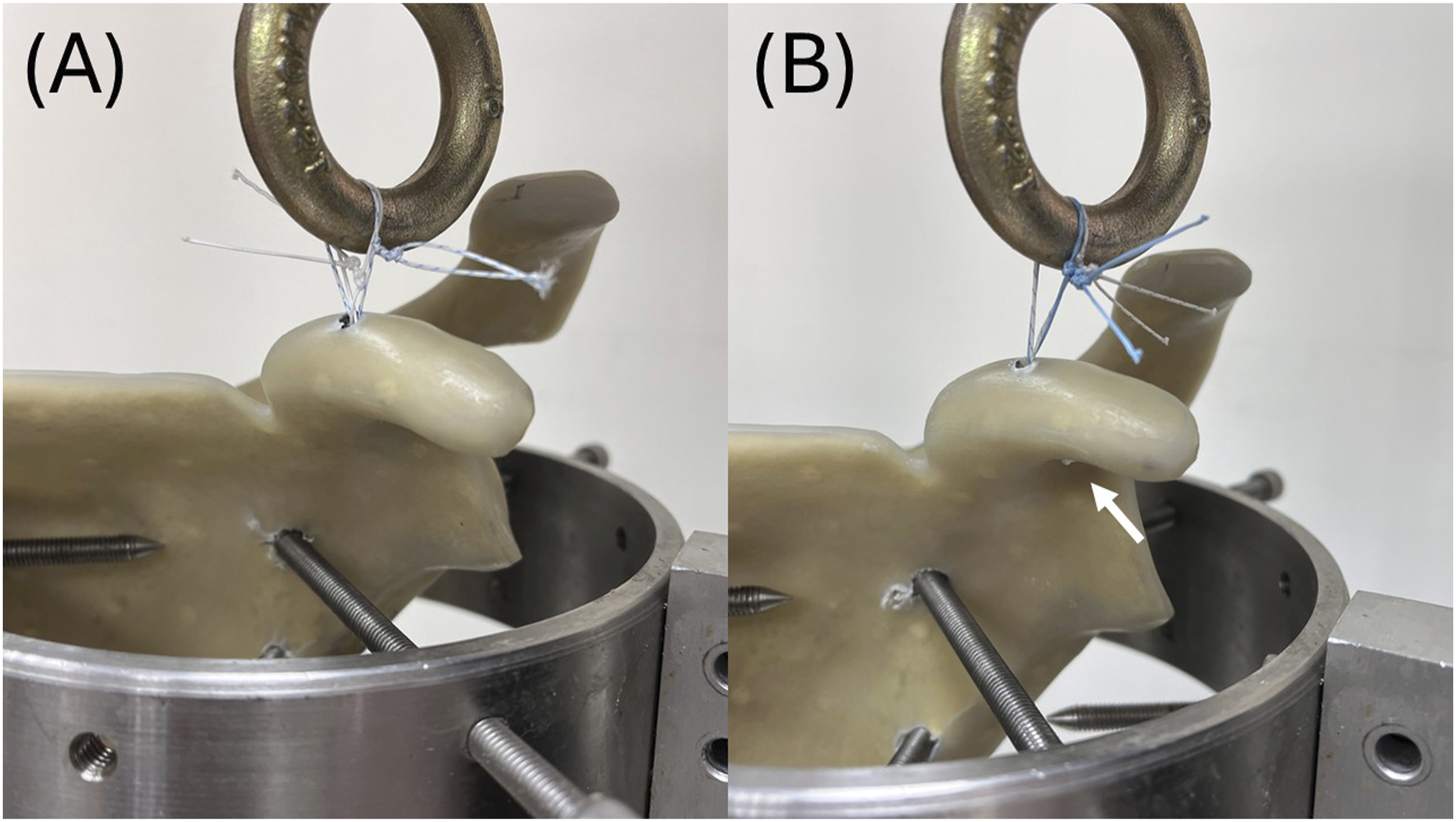
Biomechanical testing setup
Each scapular specimen was fastened to a universal material-testing system (AG-X; Shimadzu, Tokyo, Japan) using a custom-made metal clamp. The suture ends of the looping and suture anchors were tied together on the adapter of the material-testing machine. The distance between the inferior border of the adapter and superior cortex of the coracoid bone was standardized in accordance with a previous biomechanical study11,21: 10 mm in the superior-inferior direction and 6 mm in the anterior-posterior direction, resulting in a spatial distance of 12 mm (Figure 2). Biomechanical setup for specimens.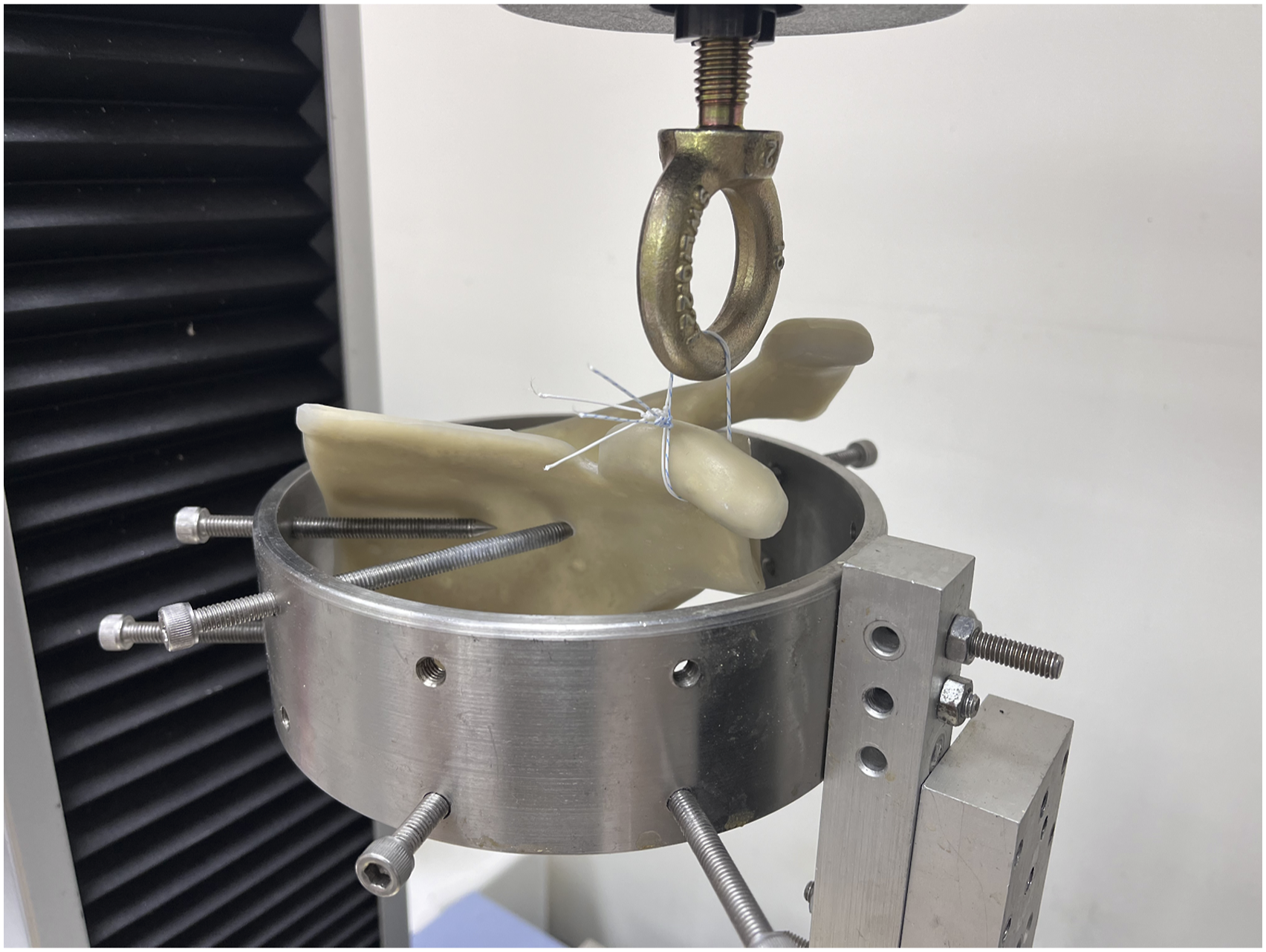
The synthetic scapula was mounted on a universal material testing system. The suture ends of either looping sutures or the anchors were tied together on the adapter connected to the material testing machine. The standardized distance between the lower edge of the adapter and upper cortex of the coracoid bone was set at 10 mm vertically and 6 mm horizontally, resulting in a spatial separation of 12 mm.
Biomechanical testing protocol
The biomechanical testing protocol adhered to the methodology outlined in previous studies.11,21 Initially, each specimen underwent preconditioning ranging between 0 and 20 N for 10 cycles to mitigate the effects of creep. After preconditioning, the specimens were subjected to cyclic loading between 20 and 70 N for 1000 cycles at a crosshead speed of 1 mm/s. The difference in the elongation recovery from the 1000th loading to the length of the complex after the first cycle was defined as cyclic elongation. 21 Following cyclic loading, each specimen underwent a load-to-failure test at a crosshead speed of 50 mm/min. Linear stiffness, ultimate load, and failure modes were recorded at the end of the test.
Statistical analysis
The required sample size for the present study was calculated based on a pilot study with nine specimens randomly assigned to three groups using G * Power version 3.1.9.7 software (Heinrich Heine-University of Dusseldorf, Dusseldorf, Germany). An α equal to 0.05 and power (1 – β) of 0.80 were given to the priori model. After substituting the means and standard variations of the three pilot study groups, an effect size of 0.74 was obtained. Accordingly, a sample size of 24 specimens, with eight in each group, was determined to be appropriate. Therefore, we opted to include nine specimens in each group, resulting in 27 specimens for this study.
Statistical comparisons were performed using SPSS Statistics version 22 software (IBM SPSS Inc., Chicago, IL, USA). Descriptive statistics, including means and standard deviations, were calculated for each group. Statistical significance was set at p < .05. The Chi-square test was used to compare failure modes among the three groups. The Kruskal–Wallis test was used to compare non-parametric parameters among the three groups; post-hoc analysis with the Mann–Whitney U test was conducted with Bonferroni correction, resulting in a significance level of p < .017.
Results
Biomechanical properties in suture looping, metallic anchor, and all-suture anchor groups.

*Significant differences among the three groups were determined using the Kruskal–Wallis test (p < .05).
a-eSignificant difference in post-hoc analysis between the two groups using the Mann–Whitney U test with Bonferroni correction (p < .017).
Discussion
The major finding of the current study was that the suture looping technique in CC fixation resulted in a significantly smaller cyclic displacement and greater ultimate failure load than fixation constructs using metallic or all-suture anchors in a composite scapula model. Previous clinical studies have indicated that adding a CC fixation construct is a crucial augmentation when surgically treating acute AC joint dislocations and distal clavicle fractures.5,8,9 When performing a CC fixation technique, whether employing suture looping or metallic suture anchor techniques, iatrogenic detachment of the anterior deltoid from the clavicle is typically necessary to expose the coracoid process, raising concerns about deltoid atrophy. 10 To address the aforementioned disadvantage, a technique utilizing an all-suture anchor in CC fixation was introduced, resulting in the avoidance of deltoid atrophy at the 1-year follow-up. 10 The present study further evaluated various CC fixation techniques from a biomechanical perspective and determined that suture looping techniques resulted in the strongest construct, whereas a fixation utilizing an all-suture anchor was associated with a greater risk of construct loosening.
The cyclic loading test in the biomechanical study is designed to mimic postoperative rehabilitation activities.22,23 In the present study, a load between 20 and 70 N was selected for cyclic loading, as it represented at least 10% of the ultimate load and covered a physiological load scenario encountered during a light postoperative rehabilitation program. 21 Greater elongation observed during the cyclic loading test indicates the loosening of a repaired construct during early rehabilitation, thereby increasing the risk of clinical failure. 11 The findings in the current synthetic bone model indicate that the looping suture technique resulted in the smallest cyclic elongation, followed by the metallic anchor, with the all-suture anchor demonstrating the greatest cyclic elongation. Similar findings were observed in a previous cadaveric study, which demonstrated that CC fixation with metallic anchors resulted in significantly smaller cyclic elongation compared to fixation with all-suture anchors. 11 Although CC fixation using all-suture anchors helps to avoid deltoid atrophy, caution should be exercised when selecting this technique, as it yields inferior results in cyclic elongation tests.
The occurrence of all-suture anchor pull-out during CC fixation has previously been reported, 10 posing a clinical concern. A previous cadaveric biomechanical study indicated that the pull-out strength of all-suture anchors in CC fixation was smaller compared to that of metallic anchors. 11 The findings in the present synthetic bone model differed from previous results, showing no between-group differences in ultimate failure load between metallic and all-suture anchors. These differences may arise from variations in cortical thickness between cadaveric and synthetic bones, as the maximum pull-out force of an all-suture anchor has been demonstrated to correlate with the thickness of the bone cortex. 12 Based on the findings of the present study, an all-suture anchor may be regarded as a viable option when selecting the suture anchor technique for CC fixation in young patients with good bone quality. However, it is important to consider the associated medical expenses because all-suture anchors are expensive. 24
Although coracoid fractures occurred in two specimens in group L during the load-to-failure tests in this biomechanical study, coracoid fracture is not currently considered a clinical complication of suture looping techniques.25,26 Instead, the use of coracoid tunnel fixation is a risk factor for coracoid fracture. 26 When examining the raw data, we found that the ultimate loads of these two specimens were particularly high, reaching 528N. This finding suggests that the suture looping technique provides a strong fixation construct, making suture loosening less likely. Failure occurs only when the bone can no longer withstand the strong tensile force, which also leads to mechanical failure in suture anchor fixation techniques.
Although findings from different studies cannot be directly compared, the biomechanical testing results in the current study generally align with those of previous studies.11,21 The elongation after cyclic loading were 1.7 ± 0.7 and 1.6 ± 0.6 mm for the 5.0 mm metallic anchors in a porcine 21 and cadaveric models, 11 respectively. Meanwhile, the elongation after cyclic loading was 2.5 ± 1.2 mm for the all-suture anchor in the previous cadaveric testing. 11 In the present synthetic bone study, similar cyclic elongation values were found in the metal anchor (1.6 ± 0.6 mm) and all-suture anchor (2.5 ± 1.1 mm) groups.
Limitation
The present study has some limitations. First, this was an in-vitro, time-zero biomechanical study. Although physiological loading 21 was simulated using the testing protocol, the study did not consider soft tissue healing. Therefore, caution should be exercised when interpreting the results for clinical use. Second, a synthetic bone was used in the current study. The strength of cortical bone in the coracoid process may differ significantly from that of natural bone, affecting anchor pull-out mechanics. Meanwhile, as synthetic bones replicate the biomechanical properties of healthy human bones 27 , data from the present study cannot be directly applied to patients with osteoporosis. Third, the clavicle was not included in the biomechanical testing. This method was chosen to minimize the effect of clamp stability on the clavicle, 11 but the effect of clavicle rotation during shoulder movement cannot be simulated. Fourth, the relatively small number of specimens per group may potentially lead to an underestimation or overestimation of biomechanical differences among fixation techniques. Fifth, physiological loading cannot be completely simulated. The cyclic loading applied in unidirectional testing did not fully replicate real-life physiological conditions. Sixth, the effect of anchor size was not taken into account. It remains unclear whether a larger anchor will lead to better or weaker fixation strength.
Conclusion
The suture looping technique in CC fixation provides a significantly smaller cyclic displacement and greater ultimate failure load than metallic and all-suture anchors.
Footnotes
Acknowledgments
We thank Skeleton Materials and Bio-compatibility Core Lab., Research Center of Clinical Medicine, National Cheng Kung University Hospital Tainan, Taiwan for assistance with this project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by National Cheng Kung University Hospital, Tainan, Taiwan (NCKUH-11304025 and NCKUH-11307025), National Science and Technology Council (NSTC112-2314-B-006-115-MY) and Tainan Municipal Hospital (managed by Show Chwan Medical Care Corporation), Tainan, Taiwan (RA24008)