
Abstract
Purpose
Chondrosarcoma is an orthopedic malignancy, and the purpose of this study was to evaluate the effect of surgery and radiotherapy (RT) on the survival of patients with chondrosarcoma.
Methods
Data were obtained from the SEER database for patients diagnosed with chondrosarcoma between 1988 and 2015. All patients were divided into surgery, RT, surgery + RT, and no surgery/no RT groups. Kaplan–Meier curves were used to analyze the overall survival and cancer-specific survival of patients in different treatment groups. The propensity score matching was used to balance baseline covariates between patients in the surgery and surgery + RT groups and in the RT and surgery + RT groups.
Results
Data from 3756 patients with chondrosarcoma were included in this study. The number of patients who underwent surgery, RT, surgery + RT, and no surgery or RT was 2885 (76.8%), 112 (3.0%), 403 (10.7%), and 356 (9.5%), respectively. Multivariate Cox regression models showed that treatment modality was independent risk factor for OS and CSS. Before PSM, Kaplan–Meier curves showed that OS and CSS were highest in the surgery group and lowest in the RT group. After PSM, although there was no significant difference in OS (p = .13) and CSS (p = .22) between the surgery and surgery + RT group, OS was longer in the surgery group than in the surgery + RT group. Additionally, OS (p < .001) and CSS (p = .009) were longer in the surgery + RT group than in the RT group after PSM.
Conclusion
Surgical resection was the key approach for the treatment of chondrosarcoma, while RT confers no significant advantage in improving patient survival time.
Introduction
Chondrosarcoma accounts for 17%–24% of malignant bone tumors, and it is characterized by the formation of the cartilaginous matrix by malignant cells. Chondrosarcoma mostly occurs in adults aged 30–60 years and have equal incidence in both sexes. 1 Chondrosarcomas are divided into two subtypes: conventional chondrosarcoma, which accounting for approximately 85% of all chondrosarcomas, and rare chondrosarcoma. 2 Conventional chondrosarcoma can be further categorized into primary central chondrosarcoma and secondary peripheral chondrosarcoma based on its position in the bone, with more than 85% of chondrosarcoma diagnosed as primary central chondrosarcomas. 2 Several rare tumor subtypes can also be distinguished, such as clear cell chondrosarcoma, mesenchymal chondrosarcoma, and dedifferentiated chondrosarcoma, all of which constitute 10%–15% of all chondrosarcomas.3–5
In clinical practice, extensive resection with negative margins is the preferred initial treatment for patients with chondrosarcoma with large tumors or involvement of the mesenchymal bone.6,7 However, in cases of large tumor size, highly malignant tumors or tumors that are difficult to resect, surgery may not always be satisfactory and radiotherapy (RT) units may be used as a treatment for incomplete resection postoperatively or for symptomatic relief.8,9 In a retrospective analysis of 60 postoperative patients with extracranial high-risk chondrosarcoma, preoperative or postoperative RT as an adjuvant treatment for tumors that cannot be resected in their entirety may reduce and prolong local recurrence. 10 A recent retrospective study of mesenchymal chondrosarcoma showed that adjuvant RT reduced the rate of local recurrence. 11 However, there is consensus that chondrosarcoma is not sensitive to RT, and Lee et al. 12 showed in a large sample case study that whether patients received RT or not did not change the outcome or prognosis. In addition, another study found that patients who received simultaneous surgical treatment and adjuvant RT had a shorter survival time than those who received only surgery. 13
Currently, the use of RT for chondrosarcoma treatment remains controversial. Therefore, we propose to evaluate the impact of surgery and RT on patient survival using clinical data from the Surveillance, Epidemiology, and End Results (SEER) database (https://seer.cancer.gov) of patients diagnosed with chondrosarcoma, with the primary study objective of overall survival (OS) and cancer-specific survival (CSS) second.
Materials and methods
Patients
The SEER database is a large publicly available cancer database, including demographic information and cancer characteristics used to study the impact of cancer on the population.14,15 Patients diagnosed with chondrosarcoma (histological type ICD-O-3: “9220: chondrosarcoma, NOS”; “9221: juxtacortical chondrosarcoma”; “9230: chondroblastoma, malignant”; “9240: mesenchymal chondrosarcoma”; “9242: clear cell chondrosarcoma”; “9243: dedifferentiated chondrosarcoma”) between January 1988 and December 2015 were searched using the SEER*Stat software (version 8.3.5). In this study, a total of 4132 patients were detected from the SEER database. Exclusion criteria were as follows: patients aged <18 years (n = 123), unrecorded survival time (n = 6), undetermined marital status (n = 232), and unknown treatment modality (n = 15). Finally, 3756 patients were included in the study (Figure 1). Patient information, including marital status, age, sex, race, primary site, histological type, SEER stage, grade, therapy approaches, survival time, and outcomes were recorded in the database. Schematic flow diagram of inclusion and exclusion criteria for our study cohort.
Patients were divided by age into four categories: <40 years, between 40 and 60 years, and >60 years. Furthermore, patients were divided into four groups according to therapeutic approaches: the surgery group was defined as patients who only received surgical resection of the tumor; the RT group was defined as patients who only received RT; the surgery + RT group was defined as patients who received RT preoperatively, intraoperatively, or postoperatively; and the no surgery/no RT group was defined as patients who did not underwent surgery or RT. OS was regarded as the primary endpoint and was defined as the time in months from diagnosis to death due to any cause. CSS was regarded as the secondary endpoint and was defined as the time in months from diagnosis to death specific to chondrosarcoma. The study used previously collected de-identified data and no additional authorization or ethical review was required.
Statistical analyses
Statistical analyses were performed in the R environment (version 3.5.3). The survminer package and Kaplan–Meier analysis with log-rank test were used to conduct survival data analysis and visualization. Cox proportional hazards regression with Wald test was conducted to determine risk factors associated with OS and CSS. p-values <0.05 were considered statistically significant.
In clinical practice, individuals receive treatment in a non-randomized manner, which may lead to systematic differences in baseline characteristics. 16 The propensity score matching (PSM) allows balancing covariates to control for biased treatment impact of studies. Compared with multivariable regression, it provides improved performance in the setting of a low number of events and is specifically more robust, precise, and less biased in the setting of seven or fewer events per confounder. 17 The inverse probability of treatment weighting (IPTW), another method applied to balance baseline measured covariates, is usually standard for balancing data. 18 In this study, PSM and IPTW were performed according to the treatment approaches, on the covariates of marital status, sex, race, age, primary site, histological type, SEER stage, and grade by using the matching package, providing functions for multivariate and propensity score matching and for detecting optimal covariate balance depending on a genetic search algorithm. 19 Subsequently, we further investigated the effect of surgery or RT on survival of chondrosarcoma patients by balancing the baseline covariates of patients in the surgery and surgery + RT groups and in the RT and surgery + RT groups by PSM. After IPTW processing, the data were used as reference for the PSM. Survival analysis, univariable Cox proportional hazards regression, and multivariate Cox proportional hazards regression were performed to analyze the raw data, and the data after elimination of treatment selection bias through PSM, respectively.
Results
Characteristics of the chondrosarcoma patients
Characteristics for different metastasis in our study.

Abbreviations: Grade I, well differentiated; Grade II, moderately differentiated; Grade III, poorly differentiated; Grade IV, undifferentiated. SEER, Surveillance, Epidemiology, and End Results; RT, radiotherapy. Percentages may not total 100 because of rounding.
Univariate and multivariate cox analysis of OS and CSS before PSM
Independent of baseline differences, we analyzed the association between OS, CSS, and different treatments using the Kaplan–Meier method with log-rank test (Figure 2). The results showed that patients who underwent surgery (including surgery and surgery + RT) had longer OS and CSS than those who received RT only or no treatment. In addition, patients treated with RT alone had worse survival than those treated without surgery or RT. Overall, patients with chondrosarcoma who underwent surgical resection had better survival than those who received RT only or no treatment. Kaplan–Meier survival curves according to treatment of chondrosarcoma patients before propensity score matching. (
Univariate and multivariate analysis of overall survival (OS) and cancer-specific survival (CSS) rates before propensity score matching.
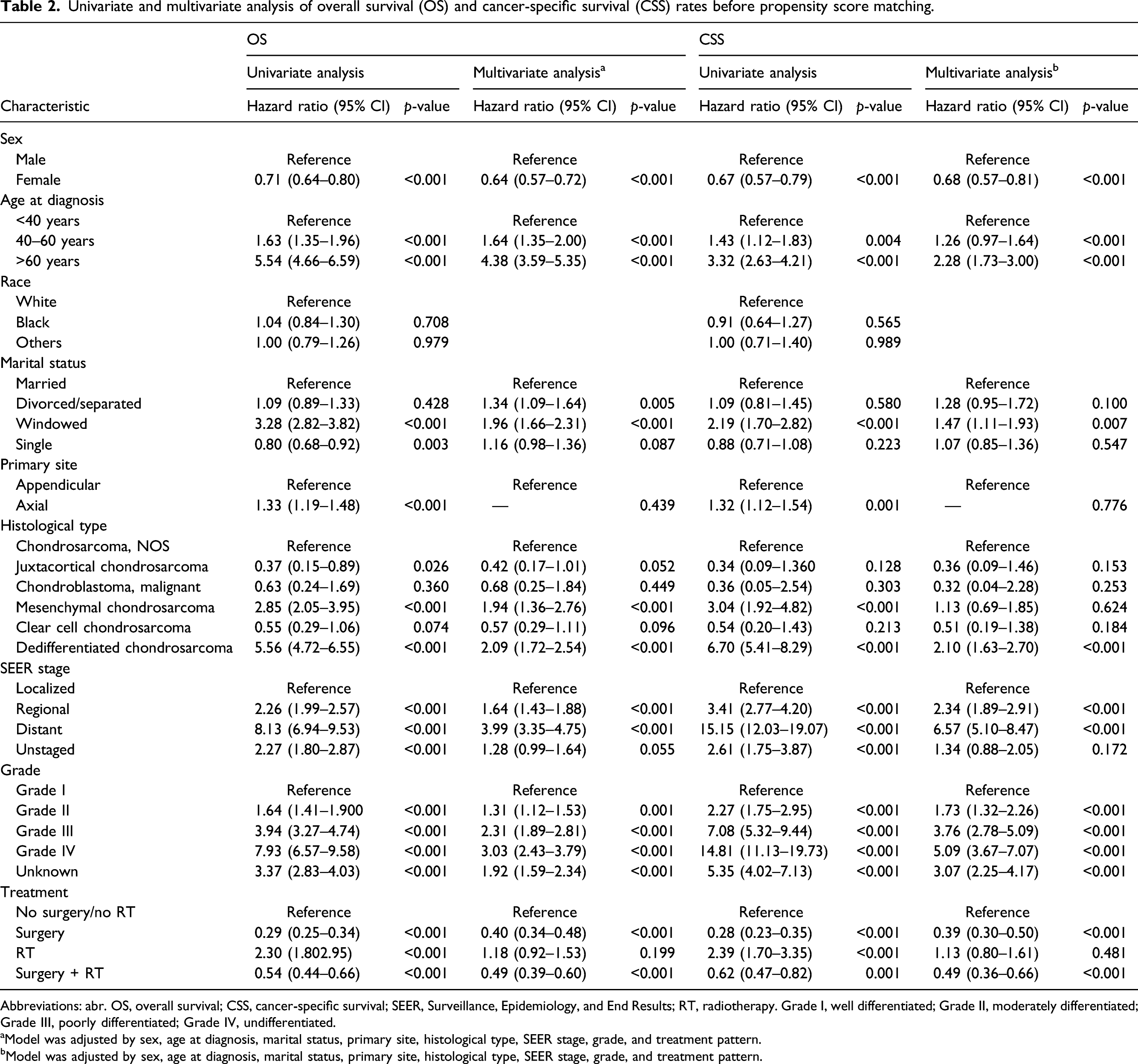
Abbreviations: abr. OS, overall survival; CSS, cancer-specific survival; SEER, Surveillance, Epidemiology, and End Results; RT, radiotherapy. Grade I, well differentiated; Grade II, moderately differentiated; Grade III, poorly differentiated; Grade IV, undifferentiated.
aModel was adjusted by sex, age at diagnosis, marital status, primary site, histological type, SEER stage, grade, and treatment pattern.
bModel was adjusted by sex, age at diagnosis, marital status, primary site, histological type, SEER stage, grade, and treatment pattern.
Surgery and surgery + RT patients after PSM
Characteristics of surgery and surgery + RT patients before and after PSM.

Abbreviations:Grade I, well differentiated; Grade II, moderately differentiated; Grade III, poorly differentiated; Grade IV, undifferentiated. PSM, propensity score matching; SEER, Surveillance, Epidemiology, and End Results; RT, radiotherapy.

Kaplan–Meier survival curves according to surgical chondrosarcomas with or without radiotherapy after propensity score matching. (
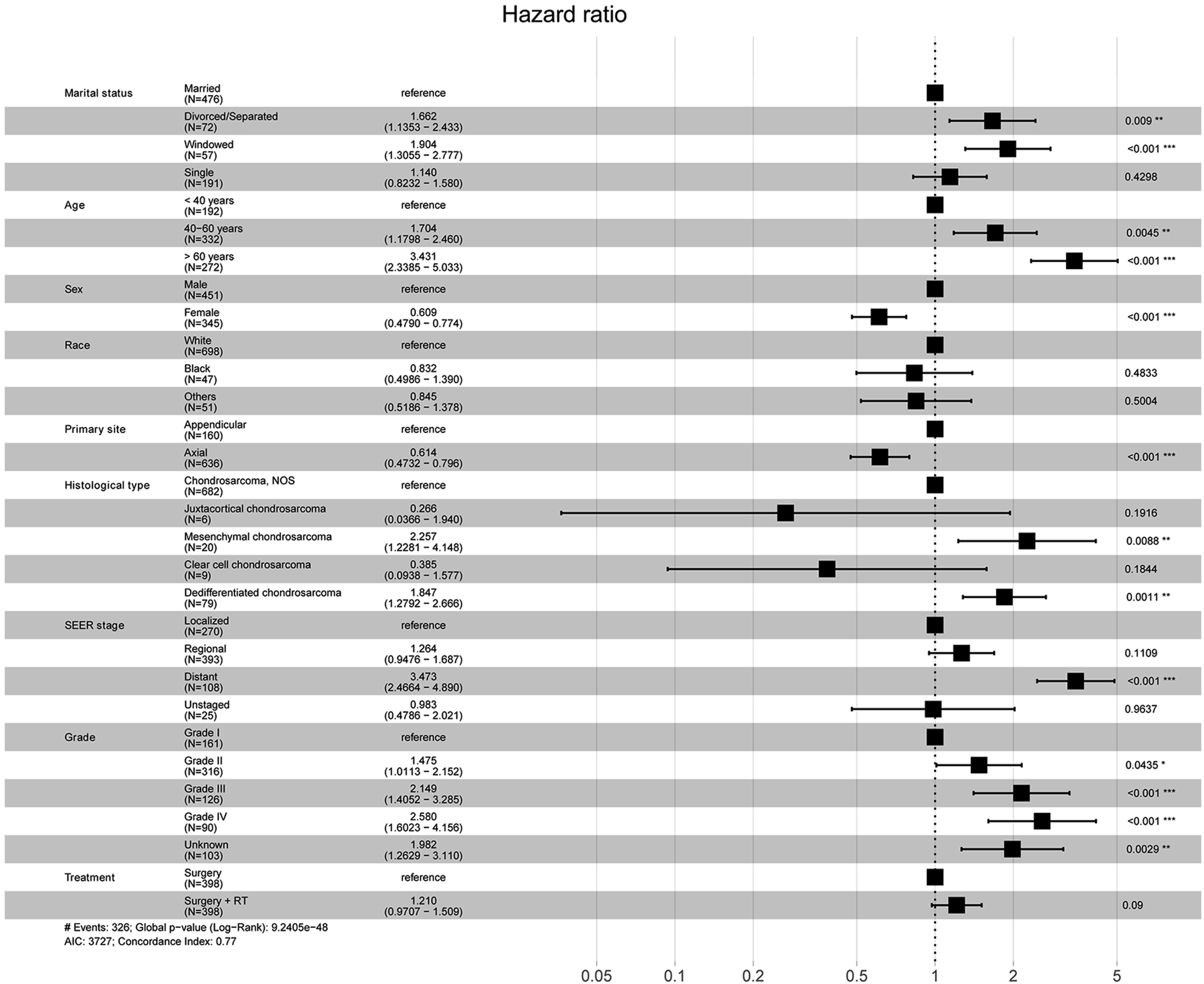
Forest plot shows multivariate cox proportional hazards regression of overall survival for surgical chondrosarcomas after propensity score matching procession.
RT and surgery + RT patients after PSM
Characteristics of surgery and surgery + RT patients before and after PSM.

Abbreviations; Grade I, well differentiated; Grade II, moderately differentiated; Grade III, poorly differentiated; Grade IV, undifferentiated.; PSM, propensity score matching; SEER, Surveillance, Epidemiology, and End Results; RT, radiotherapy.

Kaplan–Meier survival curves according to RT chondrosarcomas with or without surgery after propensity score matching. (

Forest plot shows multivariate cox proportional hazards regression of overall survival for radiotherapy chondrosarcomas after propensity score matching procession.
Discussion
In the general population, the prevalence of primary malignant bone tumors is estimated to be 1:100,000, of which 17%–24% are chondrosarcomas.20, 21 Giuffrida et al. analyzed a total of 2890 chondrosarcoma cases from 1973 to 2003 using SEER dataset and found that patients with clear cell chondrosarcoma had the highest 5-year survival rate (100%), followed by patients with common chondrosarcoma (70%), and patients with dedifferentiated chondrosarcoma had the worst survival rate. 22 Surgical resection is the primary approach and is considered the “gold-standard” for the treatment of chondrosarcoma. RT can be used in cases where the primary disease is unresectable, and the tumor is not completely resected and the symptoms are in remission. 23 However, the impact of applying RT for chondrosarcoma remains controversial. Therefore, we designed this study to illustrate the impact of RT on the survival of patients with chondrosarcoma.
In this analysis, 3756 patients with chondrosarcoma were included to determine whether RT improves survival. Approximately 76.8% received surgery, 3.0% received complete RT, and 10.7% received a combination of surgery and RT, whereas the other 9.5% failed to receive treatment. Survival analysis showed significant differences between these treatment groups. For patients with chondrosarcoma who underwent surgery, half of them had an OS time of more than 10 years, regardless of the type of RT treatment received. In contrast, only a minority of patients who received RT alone had an OS time longer than 10 years. In addition, patients receiving RT alone exhibited the worst OS or CSS time compared to patients in the other three groups. Cox proportional hazard regression model showed that RT strategy was an independent risk factor for OS in patients with chondrosarcoma, and similar result was observed in the Cox regression model for CSS.
PSM was applied for balancing baseline measurement covariates to control for biased treatment effects of the research. First, after PSM in surgical patients with or without RT, no significant differences were observed in both OS and CSS between the two groups, but the median OS time was shorter in surgical patients with combined RT. Second, after PSM in RT patients with or without surgery, chondrosarcoma patients with surgery + RT had better OS and CSS than those who received RT alone. Cox analysis also indicated that surgical treatment was an independent protective factor in patients treated with RT. One study showed a slight difference in CSS (p = .048) and no significant difference in OS (p = .075) in patients with spinal chondrosarcoma combined with or without RT. 24 This study further noted that RT may have a negative impact on survival time in patients with surgical chondrosarcoma. Overall, the results suggest that patients with chondrosarcoma who received surgical resection tend to have a good prognosis, that RT does not improve survival time for patients with chondrosarcoma, and that RT cannot be used as a primary management for cases of chondrosarcoma.
Although chondrosarcomas are not sensitive to RT and RT may carry a potential risk of paralysis and other neurological side effects for chondrosarcoma patients, RT is still considered a treatment for inoperable chondrosarcoma patients and for the relief of local symptoms.2,25 If RT is considered, it should be a factor in deciding treatment. Xu et al. 23 suggested that RT could be used as a remedial treatment to reduce the recurrence rate for patients with positive margins or those unable to undergo extensive resection. Eric et al. 26 found that receipt of external beam RT was associated with CSS benefit for localized extraskeletal myxoid chondrosarcomas. However, several studies have shown conflicting views. By retrospectively analyzing 973 cases of chondrosarcoma of the spine from 1973 to 2012, Arshi et al. 13 found that RT was an independent indicator of worse OS and that RT worsened outcomes in patients with confined and locally invasive disease. Similar result was reported by Chen et al. 24 who suggested that OS and CSS were higher in the surgery alone group than in the surgery + RT group for chondrosarcoma of the osseous spine, and that low-grade chondrosarcoma of the osseous spine was resistant to RT. Our findings are more consistent with the latter study as patients who received surgery combined with RT had a shorter mean median OS time than surgery alone, and patients who received RT but not surgery had a worse survival time than surgery alone. Therefore, we do not recommend the use of RT in chondrosarcoma and RT does not improve survival in cases where chondrosarcoma is not completely resected.
In speculating on the reasons why RT was associated with poorer prognosis, we noted that patients who underwent surgery were more likely to be white, localized stage, and grade I–II, while more elderly, widowed, and distant stage patients opted for RT. Age and tumor stage were recognized prognostic correlates of chondrosarcoma, and a large number of studies have shown that advanced age as well as high stage of chondrosarcoma were associated with poorer prognosis.24,27,28 In addition, marital status was also a prognostic factor in chondrosarcoma. Through a survey of 4502 patients with chondrosarcoma between 1977 and 2014, Gao et al. 29 found that widowed patients had the worst CSS compared to married, divorced, and single patients (p < .001).
To the best of our knowledge, this is the largest sample size analysis on the prognostic impact of surgery and RT on chondrosarcoma. We demonstrated the association between the different treatments and survival time in patients with chondrosarcoma using survival analysis and Cox proportional hazards regression analysis. Moreover, PSM was used to balance the baseline measured covariates in order to control the biased treatment effects of research, which should improve the robustness of the results. However, our analysis also has several limitations: (1) we analyzed all types of chondrosarcomas together, which may not have captured the effect of different types of chondrosarcoma with different responses to RT; (2) since the SEER database does not contain information on the dose and duration of RT, different doses and durations of RT may produce different treatment effects and therefore require further study; (3) due to missing data in the SEER database on whether the treatment approach/choice changed during the study period, we were unable to obtain information on whether patients changed during treatment; and (4) in addition, information on post-treatment complications could not be found in the SEER database, and we were unable to obtain information on the surgical margins of patients with chondrosarcoma, which could also affect the prognostic survival time.
Conclusion
In this analysis, we can conclude that surgical resection should remain the primary treatment for chondrosarcoma, and RT confers no significant advantage in improving patient survival time.
Supplemental Material
sj-pdf-1-osj-10.1177_10225536221086319 – Supplemental Material for Effect of surgery and radiotherapy on overall survival in patients with chondrosarcoma: A SEER-based study
Supplemental Material, sj-pdf-1-osj-10.1177_10225536221086319 for Effect of surgery and radiotherapy on overall survival in patients with chondrosarcoma: A SEER-based study by Miao Wang, Yu Song, Shengfu Liu and Weibing Sun in Journal of Orthopedic Surgery
Footnotes
Acknowledgments
The author is very grateful to all the funders of the SEER database.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study used previously collected de-identified data and no additional authorization or ethical review was required.
Data availability
All of the data is available on the SEER database.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.