
Abstract
In the 1970s, the concept of sport addiction appeared in scientific literature, warning of the addictive properties of exercise when taken to extremes. Appearing in over 6500 peer-reviewed articles in Google Scholar from 1979 to 2017, this construct is of interest to the fields of mental health and sport sociology as it provides a heuristic case to consider the conditions which allow for a category-in-the-making to gain meaning despite its absence from leading classification systems. Using Hacking's framework of ecological niches, this review of literature provides a critical examination of “sport addiction” and aims to investigate the driving forces and the means by which social actors from the scientific community negotiate the landscape and boundaries of this emerging disorder. The results highlight the prominence of psychology in the diffusion of the construct and the reticence of the medical world to legitimize it as a mental health category.
Keywords
Introduction
A large body of literature exists on the positive link between physical activity and health and reflects a broad consensus that sport and exercise are integral to a healthy lifestyle (Craig, 2016). While these claims remain largely uncontested, the emergence of the classification “sport addiction” highlights the potential downfalls of exercise. This concept is of interest to the fields of mental health and sport sociology as it provides a heuristic case to consider the conditions which allow for a mental health category-in-the-making to gain meaning and currency as a medical category within some professional circles despite its absence from leading classification systems, including the American Psychiatric Association's Diagnostic and Statistical Manuel (DSM) and the International Classification of Diseases (ICD).
The objective of this article is to analyze, from a sociohistorical perspective, the evolution of this emerging classification in the scientific field by reviewing 377 peer-reviewed articles on sport addiction. More specifically, we ask: (1) How is sport addiction being constructed and problematized as an object of knowledge in scientific literature but also reworked and redefined to gain legitimacy in the scientific field? (2) What are the conditions which enabled this healthy behavior to morph into a potential pathology?
Sport and health: normative links
To understand how the construct of “sport addiction” was able to emerge while the medical field (1) greatly values the health benefits of exercise and (2) holds authoritative power in determining the parameters of normality and abnormality (Canguilhem, 2013), we must look to history.
Recognizing that differences exist between western countries (Rieu, 2010), we take the U.S. to illustrate how this favorable relationship between sport and health developed in the medical field. First, classical health reform literature in 19th-century America is rooted in the ancient non-natural tradition of Hippocrates and Galen, who articulated vigorous exercise as a non-innate prophylaxis (Berryman, 1989). Hence, during the 1800s, moderate exercise featured prominently in medical books as key to the preservation and enhancement of health (Tipton, 2014). In prevention and hygiene literature, this tradition was popularized as the “laws of health” (Berryman, 2010: 196). The value of exercise for health and self-improvement ushered in the physician-led physical education movement in the late 1880. With organized and competitive sport gaining popularity, physical education developed as a distinct profession encompassing its own specialized fields (Berryman, 1989). Turn-of-the-century advancement in the field of infectious disease led to the relative divestment of the medical community in the study of exercise (Rieu, 2010).
Finally, in the 1960s, medical interest in exercise was rekindled for two main reasons. First, groundbreaking mid-century epidemiological studies clearly linked physical inactivity and chronic disease (Favier-Ambrosini, 2016). Second, exercise regimes became medically prescribed in response to growing public health concerns regarding the productive and economic consequences of unhealthy lifestyles (Berryman, 2010). Recaptured by the powerful medical institution, exercise gained credibility concomitantly to the emerging healthism 1 discourse of the 1970s and 1980s (Carney et al., 2018), where top medical and sport science journals began publishing research on various aspects of physical activity (Berryman, 2010). Medical professionals thus became gatekeepers of the message of responsible exercise for health risk management (Génolini and Clément, 2010) and contributed to the exponential production of publications and statements promoting exercise as vital to health (Waddington, 2002). Interestingly, the timing coincides with the mid-1970s emergence of the term “sport addiction” in scientific literature.
Broadly, the medical establishment endorses a “sport-health ideology” (Malcolm, 2017: 6) where illness has become a consequence and punishment of non-adherence to medical and sports norms. Moreover, health is no longer defined by an absence of disease, but as a “state of complete physical, mental, and social well-being” (WHO, 2020: 1). This utopian configuration of health has to be understood in the context of Western societies where the individual is constructed as responsible for his own health and as the principal actor of his well-being (Leonardi, 2018). Therefore, sport becomes a tool to achieve healthism, where all daily acts must be thought out in terms of a “cost-benefit ratio for our health” (our translation, Moreau and Vinit, 2007: 42).
Because physical activity is now framed as medicine (Carney et al., 2018), sport and exercise figure prominently in the disease treatment and prevention paradigm, even though (1) recurrent sport injuries or doping in elite sport are regarded as public health concerns (Catlin et al., 2008) and (2) sport is still largely absent from public health policies in some western countries like the U.S. (Warner, 2019). Without delving into modern controversies surrounding exercise regimes, this overview shows how, within the medical field, exercise has historically been considered conducive to health (Neville, 2012). We turn to our theoretical framework to explain how this article provides a nuanced, contextual account of the scientific evolution of sport addiction to examine the conditions which enabled certain exercise behaviors to transform into pathology.
Theoretical framework
Hacking’s (1998) theory of ecological niches is useful to study the socio-historical emergence and conceptual intricacies of a category-in-the-making (Brossard, 2019; Neufeld and Foy, 2006). This framework proposes to examine how, in a given society at a given historical moment, some “transient mental illnesses” emerge, potentially for a limited time. In this context, the emergence and diffusion of a trouble evolves in accordance with social and political change (Garriott and Raikhel, 2015). This theory thus explores the various, potentially contradictory micro-powers at stake—for example, experts who negotiate the landscape and boundaries of the illness. Rising scientific interest in sport addiction since the 1980s make it a suitable case study for this perspective.
Hacking's theory of ecological niches considers that four “vectors” must converge for a “transient mental illness” to develop: (1) medical taxonomy (the illness integrates the medical representations of its time); (2) observability (the illness is observable in its social context); (3) cultural polarity (the illness occupies an ambiguous position between several “social figures”); and (4) release (the illness provides a form of relief that is not attainable elsewhere in the culture). While the initial theory focused on transient mental illness, Brossard (2019) proposes operationalizing each vector to encompass all mental illness by exploring the social configurations which render “falling ill” empirically realizable.
More specially, by applying the vectors to our corpus of scientific articles, we can explore (1) the “social configuration in which some people are led to get involved in the diffusion of a studied category” (medical taxonomy vector) (Brossard, 2019: 7); (2) how the classification process takes shape in the scientific realm—how the problem is made visible and is interpreted as a problem (observability vector); and (3) the populations being studied, the main social figures being endorsed through the identified troubled behaviors and the debates allowing the category to be discussed, argued and depicted in the scientific world (cultural polarity vector); and (4) how sport addiction can provide people a way—often the only way—to escape their social strains, such as constraining norms, emotional difficulties or cultural expectations (release vector). In this text, we especially focus on the medical taxonomy vector to illuminate the various positions and frameworks proposed in scientific literature, thus showing how medical and non-medical actors delineate and define social transgressions being translated as “sport addiction”.
Method
Our data is drawn from a review of literature on sport addiction that was conducted as part of a broader research project on behavioral addiction in Canada and Australia. In February 2019, we performed a literature search for publications from 1950 to 2017 in the database Google Scholar, a multidisciplinary web-based search engine for academic literature, to identify studies relevant to our analysis. The following search terms were entered to delineate our search: “sport addiction” OR “exercise addiction” OR “sport dependence”, “exercise dependence” OR “bigorexia”.
The initial search yielded 6673 articles in English or French, and were screened using the following inclusion criteria: (1) the publication qualified as a scientific article published in a peer-reviewed journal; (2) if more than 100 articles were identified for one year, only articles with at least 10 citations were considered; and (3) at least one paragraph in the article addressed the topic of sport addiction. With respect to selecting inclusion criteria, our decision was first pragmatic. After thoughtfully perusing the literature provided by the search terms, we were confronted with a large number of articles. Selection criteria were chosen strategically to reduce the sample whilst also offering a comprehensive picture of the current state of knowledge about the topic. Our decision was also theoretical. In studying how categories take shape in the social world, we specifically aimed to select articles that had “won” the interest of the scientific community and therefore, were more likely to be diffused on the social realm. This decision also aligned with our objective to analyze the framings circulating in the scientific sphere.
Data selection was performed by the first author, and studies that met the aforementioned criteria were carefully read to ensure accurate inclusion and topic relevance. The last author and a third party researcher were consulted regularly to resolve uncertainty. The screening process yielded the retrieval of 405 relevant scientific articles. We excluded 28 neurobiological studies which aimed to study specific neurobiological/neurophysiological elements of sport addiction. These studies were analyzed as separate data. We retained 29 studies that explained sport addiction through neurological understandings but, contrary to the 28 excluded neuro-based studies, these papers did not study specific neurological components.
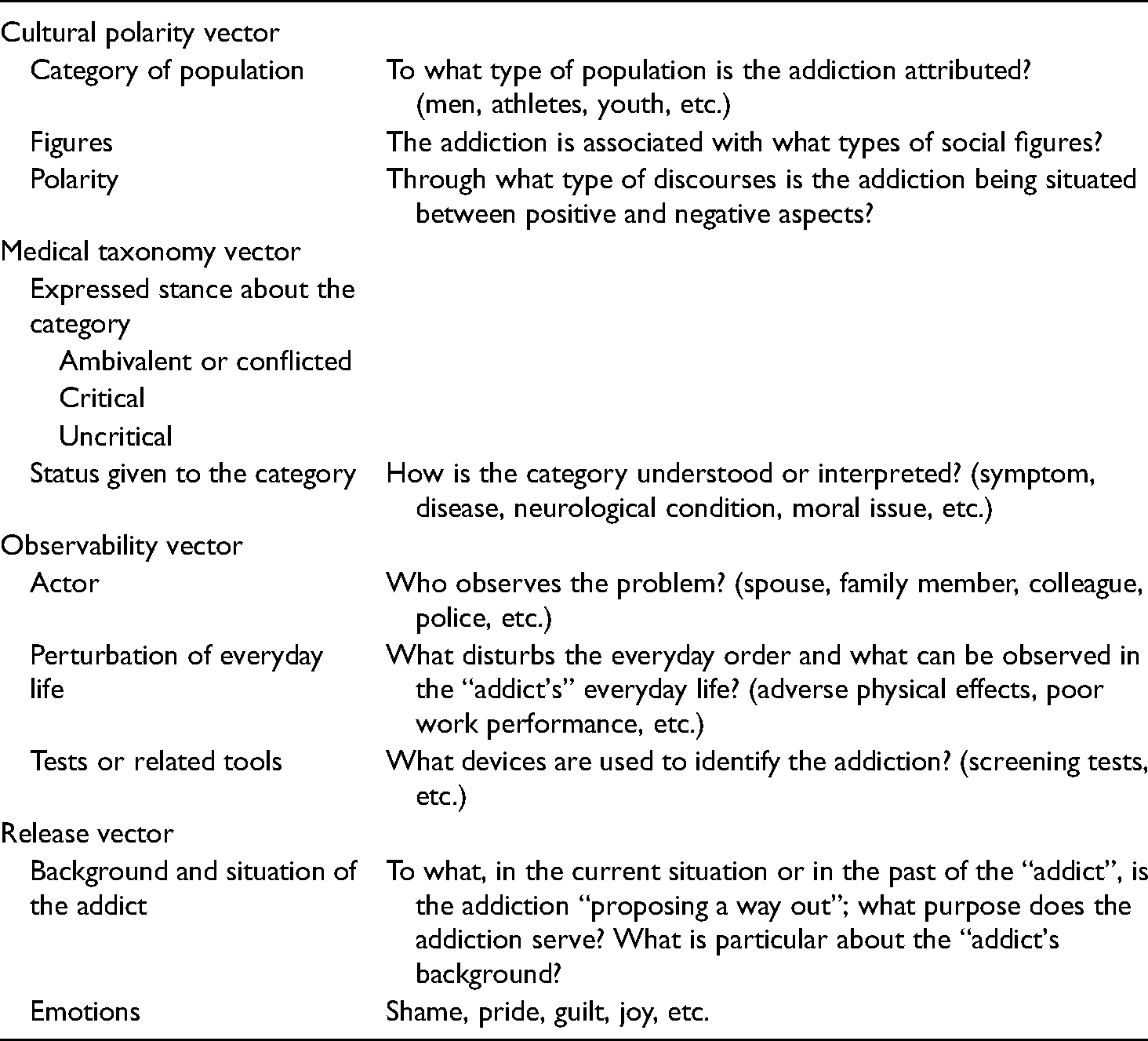
A total of 377 articles were retained for coding and analysis. The publications were imported into NVivo-12, a software designed for qualitative data management and analysis, and were carefully re-read by the first author. A hybrid approach of deductive and inductive thematic analysis (Fereday and Muir-Cochrane, 2006) was chosen for its theoretical flexibility and reflective quality. Data was manually coded by the first author, initially by deductive reasoning, using a code guide based on Hacking's theory of ecological niches, which included the four vectors and theoretically-driven subcategories (Table 1).
Theoretically driven coding guide using Hacking’s vectors.
Through an iterative process and data-driven inductive approach, we then refined categories of analysis inductively, thus detailing how each of Hacking's vectors were being configured in scientific research. The second author adopted the role of “critical friend” (Smith and McGannon, 2018: 117) and was consulted regularly for coding verification. Several steps of category merging were undertaken to obtain the final numbers of categories (see Figure 1 for an example of coding map).
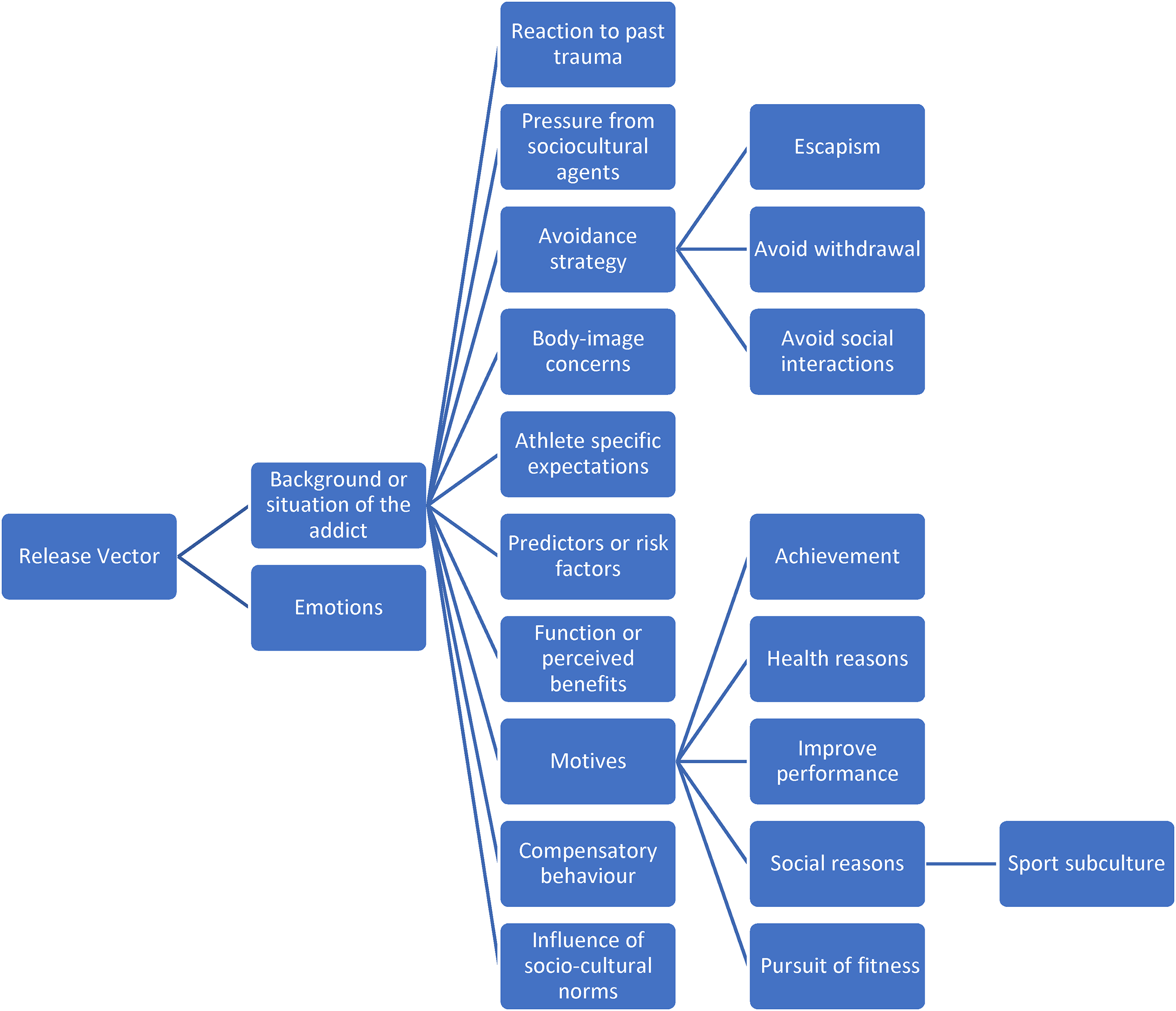
Simplified thematic map for the release vector showing sub-categories for “background or situation of the addict” and detailing only the themes of “avoidance strategy” and “motives”.
Due to our coding method and loose boundaries of categories, overlaps between categories were observed, therefore, data is presented mainly as numbers instead of percentages.
Results
Descriptive characteristics
Descriptive characteristics were first created to provide a global portrait of our data to examine where and when sport addiction was being diffused. Our results include (1) the number of articles produced per year, (2) the predominant journals that have published on sport addiction and (3) the subject area or field of expertize of first authors who have contributed to the category's diffusion in scientific literature.
Number of articles produced per year
The articles retained for analysis were published between 1979 and 2017 (Figure 2). From the time of the first publication on sport addiction in 1979 until 1994, the number of articles published per year ranges from one to five. A slight increase occurs between 1995 and 1998, where seven to ten articles were produced per year. After a decrease in 1999 and 2000, a second increase appears from 2001 to 2010, where publications reach between ten to twenty per year. This expansion continues as the number of publications peaks at thirty in 2011 then largely plateaus until 2016. We explain the lower publication rate in 2017 by the date chosen for analysis (February 2019), when articles might not have had the opportunity to be cited more than ten times.
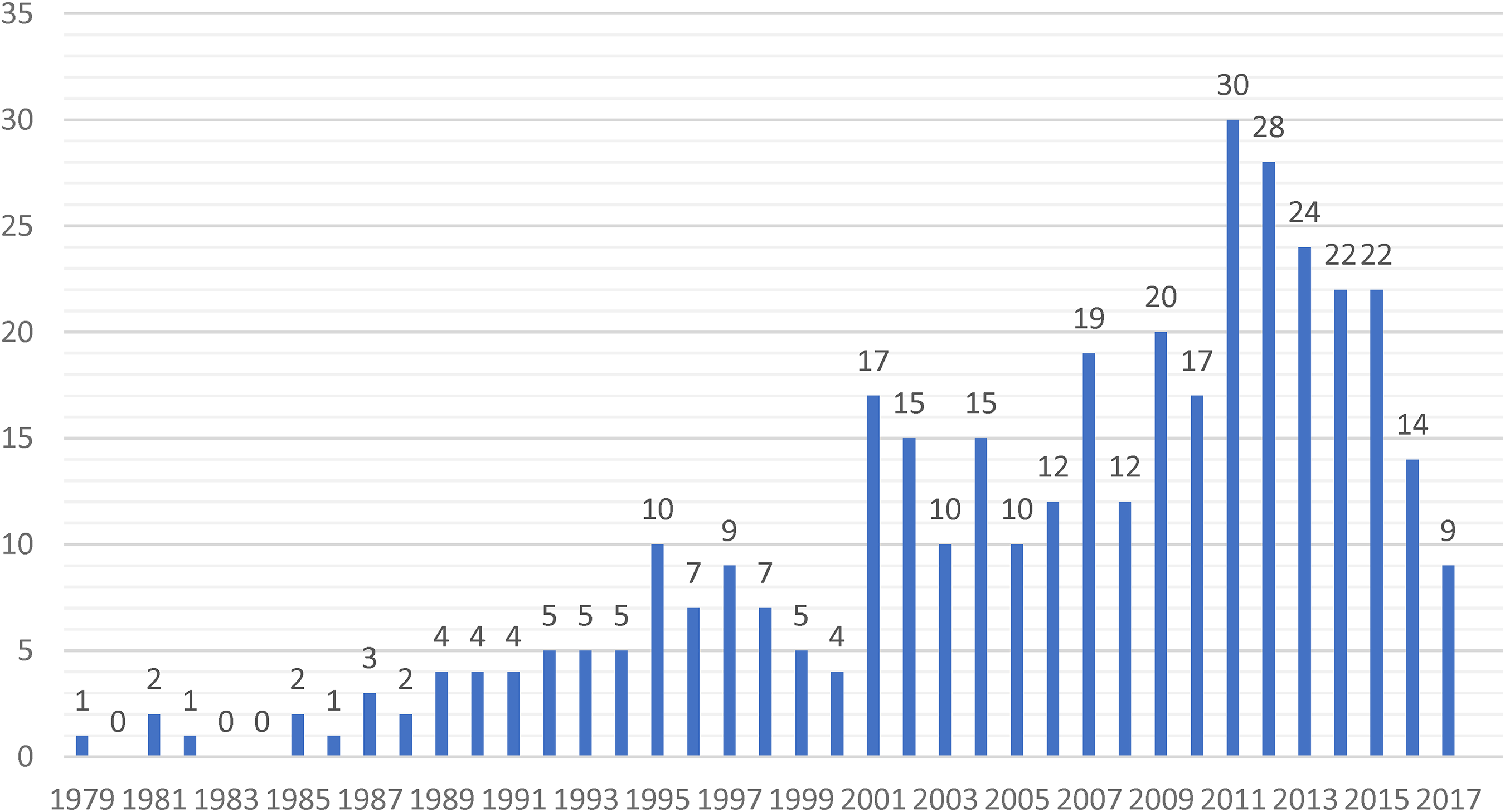
Number of articles published on sport addiction per year (1979–2017).
Journal names/types
Data was drawn from 120 different journals, classified according to their primary subject area, as per their respective web pages. This yielded 28 journal types. Psychological journals produced the largest number of articles on the topic of sport addiction (n = 117). Other significant journal types include eating disorders/body image (n = 77), sport medicine/sport science (n = 74), addictions (general) (n = 51), psychiatry (n = 23), and behavioral addictions, where all 19 articles appear in the relatively recent Journal of Behavioral Addictions.
Expertize of first authors
These findings regarding the dominance of psychology align with our data on the academic background of first authors. We found that 123 first authors were either psychologists or affiliated with a psychology department. The other most prominent disciplines are psychiatry (n = 42), sport sciences (n = 35), physical education/kinesiology (n = 33), medicine (n = 30) and physiology (n = 9).
The medical taxonomy vector: framing sport addiction
Taking a stance: affirming or resisting the realness of sport addiction
One of the analytical elements within the medical taxonomy vector refers to the author's stance or viewpoint; that is, how authors either support or contest the “realness” of sport addiction. Authors’ stances were classified into three categories: convinced (n = 282), cautious (n = 123) and skeptical (n = 35).
Convinced
Significantly, out of the 377 articles analyzed, 282 convey a non-critical stance towards the category; that is, they depict sport addiction as a meaningful, distinct diagnostic entity and do not question its existence: “There is now much evidence that a state of exercise dependence exists […]” (Long et al., 1993: 321).
Cautious
One-third (n = 123) of papers, while they may not question the category's existence per se, convey an ambivalent position toward specific elements, such as ambiguous boundaries between normal and pathological, as in Håman et al. (2017: 2)—“no consensus exists in the scientific literature regarding when exercise becomes excessive or compulsive”—or discord regarding prevalence rates, as in Egorov and Szabo (2013: 206)—“The spectrum of the reported preponderance ranging from 0.3% to 77% shows that there are theoretical and methodological barriers to research in this area”. While these authors generally “accept as a given that such a group of individuals [sport addicts] exists” (Le Grange and Eisler, 1993: 101), they call for specific areas of research to better delineate and understand the dysfunction.
In 58 articles coded as “cautious”, this ambiguity was most often attributed to lack of consensus regarding definitions and to inconsistent terminology, therefore leading to an unclear conceptualization of the construct across studies. Indeed, although “sport addiction” has been an object of research for over three decades, no consensus has yet been reached on terminology. The definitional/terminological debate is sustained and exacerbated by a variety of factors, including lack of consensus regarding the characteristics, symptomatology, underlying mechanisms, etiological factors and determinants of sport addiction. Also, 17 papers affirm that lack of empirical evidence prevents substantiation of the construct's existence. Another 17 of these “cautious” authors question the quantitative criterion used to define, evaluate and diagnose sport addiction. As Lease et al. (2016: 470) illustrate, “a high frequency of exercise does not automatically imply a maladaptive exerciser”. Relating to “major methodological problems with past investigations” (Pasman and Thompson, 1988: 760), such ambiguities reflect a broader dilemma about the measurement instruments and assessment tools developed for sport addiction. What these existing psychometric tools capture and convey about so-called sports addicts varies significantly from one test to another and, as highlighted by Szabo et al. (2015), they tend to evaluate risk rather than diagnose. Indeed, we’ve identified over 86 tests and scales, discussed later, most of which assess different aspects of the phenomenon through various criteria and often non-validated measures.
Skeptical
A mere 28 of the 377 articles were coded as skeptical, meaning they openly question the legitimacy of the category. Interestingly, nearly two-thirds of critical papers were published after 2011 and most (n = 20) utilize sociological elements to critique the construct. In some cases, they question the clinical significance of the syndrome or warn against the iatrogenic effects of labeling and of medicalizing sport and other everyday activities: If [exercise ‘addiction’ should be defined and used as a diagnostic category], then people may begin to construct themselves and their exercise in this way and present with the ‘problem’ of exercise addiction […]. As this happens medical practitioners will start to diagnose it and clinical psychologists, amongst others, will invent ways of ‘treating’ and ‘curing’ it (Cox and Orford, 2004: 187).
Others urge researchers to consider social context to avoid individualizing problems; as argued by Konkolÿ Thege et al. (2015: 2), “there is concern that the medicalization of behavioral addictions drives our attention to the person instead of the societal, technological and financial systems that may make individuals susceptible to the development of these dysfunctional habits”. In these instances, there is a volition to reframe the trouble by shifting the gaze toward broader social structures, cultural ideologies, political forces and historical factors. As per the cultural polarity vector, these papers provide a mise en garde against the endorsement of the label, thus allowing the construct to become an object of discussion and controversy (Hacking, 1998).
Etiological and explanatory models of sport addiction
The status given to the category, a second analytical element under Hacking's medical taxonomy vector, allows us to investigate how, and through which etiological models, a category is explained and constructed. Specifically, our findings indicate that sport addiction is predominantly structured around five interpretation models: (1) psychological models or theories (n = 163) (personality traits, intrinsic and extrinsic motivational components, positive or negative reinforcement); (2) addiction model (n = 148), which mainly uses classical indicators of substance dependence via the DSM to frame sport addiction and largely emphasize neurobiological interpretations of addiction; (3) multidimensional perspective (n = 120), which connects classical indicators of addiction to other factors (psycho-bio-physiological); and (4) sociocultural frames (n = 67).
Psychological models
Considering that psychology journals have produced a plurality of scientific articles on sport addiction, psychological models unsurprisingly dominate the literature (n = 162). Articles were coded in this category when specific psychological processes were utilized to better apprehend or explain psychological factors associated with sport addiction. Amongst these publications, three psychological explanatory models stand out: (1) cognitive-behavioral models (n = 64), (2) personality theories (n = 41) and (3) motivational theories (n = 24).
Psychological explanatory models appear in only 19 studies prior to 2000 and flourish during the 2000s and 2010s. Indeed, to go beyond classical indicators of addiction to problematize the trouble, authors increasingly sought to examine specific psychological mechanisms behind sport addiction and identify the associated means, motivations and personality components.
Addiction model: a biomedical view of sport addiction
The addiction paradigm (n = 118) provides a more homogeneous view of sport addiction by focusing mainly on the core biomedical features of addiction. Aside from the classical indicators, we found that within the addiction model, the construct is shaped by two other main assumptions. First, it is explained through neurobiological features (n = 29) or compared to drug addiction (n = 22) (which often highlight the physiological mechanisms of addiction). In line with biomedical interpretations of addiction, sport addiction was first compared to a drug in Morgan's foundational article in 1979. These comparisons noticeably gain complexity and frequency, especially after 2000, where the drug-like effects of sport addiction are increasingly examined in relation to neurobiological mechanisms.
Second, and this happens mostly after 2010, sport addiction is discussed in relation to other types of behavioral addictions (n = 20). Generally, studies either investigate addictive comorbidities—“Exercise addicts […] appear more exposed to another form of behavioral addiction (ie, compulsive buying) […] and they spend more time on their computers” (Lejoyeux et al., 2008: 357)—or consider how sport addiction substitute another addiction, as in Kolnes (2016: 2): “it could, however, be suggested that she had mainly replaced one compulsion with another in the process of becoming a devoted triathlete”. This rising interest in the relationship between sport addiction and other behavioral addictions may be attributed to the increasing credibility of non-substance addictions in medicine, as indicated by the inclusion of certain behavioral addictions, such as gaming disorder and internet addiction, in the DSM-5 (Pinna et al., 2015) and with the creation of the Journal of Behavioral Addictions in 2012.
Multidimensional models
Sport addiction was conceptualized according to a multidimensional perspective in 120 papers. Multidimensional models generally rely first on classical models for indicators of addiction then extend such models by incorporating psychosocial factors. Veale (1987) was the first to propose that sport addiction should encompass both biomedical features, like withdrawal, and psychosocial components, such as interference with social functioning. Later the same author, along with colleagues (Ogden et al., 1997: 352), conceptualized exercise dependence “within both traditional biomedical and psychosocial perspectives” by developing their Exercise Dependence Questionnaire. Particularly after the construction and validation of the most important assessment tool, Hausenblas and Downs’ (2002) Exercise Dependence Scale (EDS), eagerness to combine various theories to account for the multidimensional features of sport addiction became evident in literature.
Accordingly, during the 2000s, we observed a strong push for social recognition of the problem through this process of utilizing psychometric instruments to objectify sport addiction. Aside from the 53 papers which mainly rely on Hausenblas and Downs’ model to explain or study the construct, other multidimensional models appear in scientific literature, including the psychophysiological model (n = 38) and the biopsychosocial model (n = 25).
Sociocultural frame
Another framework proposed in scientific literature is the sociocultural perspective (n = 67). While multidimensional frameworks may consider sociocultural risk factors, “sociocultural” papers frame sport addiction first and foremost as a disorder driven by sociocultural factors. Sociocultural frames divert from the dominant positivist viewpoint found in most addiction, psychological and multidimensional theories by studying sport addiction from a social constructionist vantage point. Most of these articles (n = 59) use a normative perspective, where one model particularly stands out: the cult of the body, present in 44 papers. Here, cultural body image ideals are presented as important risk factors in the development and sustainment of sport addiction. The often unattainable but internalized body standards are said to help predict and explain pathological exercise behavior. Fitness or sport culture (n = 8) offers another normative lens through which the emergence of sport addiction can be understood. Finally, sociological theories are present but scarce in scientific literature on sport addiction (n = 5).
Notably, these normative studies appear in literature only after 2010, perhaps partially owing to increased scholarly interest in gender variables and emerging body-image related illnesses, especially in men, such as bigorexia and muscle dysmorphia. Indeed, research papers examining body disorders in men account for 37.3% (n = 25) of sociocultural studies published between 2010 and 2017 and reflect today's cultural climate where men's bodies are represented in ways that increasingly encourage dissatisfaction with one's appearance (Mataix, 2011).
Constituting a problem: the blurry boundaries of “sport addiction”
The medical taxonomy vector also enables mapping the label's social evolution according to its comparisons or connections to other illnesses. Significantly, 340 studies mention at least one link to other diagnostic categories, thus blurring the parameters of this category in-the-making. Our findings indicate, first, that eating disorders and body image disorders are by far the most-cited illnesses related to sport addiction. Second, sport addiction is also compared to various other mental health disorders.
Eating disorder or sport addiction? Nearly half of the studies (n = 186) mention the link between sport addiction and eating disorders. This relationship originates in the 1990s, with 26 studies on the subject. A notable increase is observed in the 2000s (n = 72) and again in the 2010s (n = 137). These studies portray the relationship diversely, by constructing sport addiction as playing a central role in the pathogenesis of eating disorders, as either a prominent feature, symptom, contributor, comorbid illness, or manifestation of eating disorders.
A total of 63 studies link sport addiction to body image disturbances, including drive for muscularity (n = 10). It is also linked to muscle dysmorphia in 36 articles, where sport addiction is explained as a manifestation or component of this disorder. Several studies mention the ongoing primary or secondary disorder debate—the question being, in the absence of eating disorder symptoms, can sport addiction constitute a clinically significant syndrome? Some authors argue that sport addiction only co-exists with eating disorder pathology (n = 29) or other mental illnesses, while others argue that sport addiction can exist independently (n = 37), as a primary addiction.
Never a lone addiction? Aside from eating disorders and body image disorders, other mental health diagnostic categories have been linked to sport addiction. Obsessive-compulsive disorder (OCD) (n = 42) is most cited as correlated to sport addiction. The obsessive quality mentioned in these papers reiterates the link with eating disorders and muscle dysmorphia, which are recognized as having strong obsessionality components. The patterns and rituals intrinsic to sport addiction are explained as “strongly reminiscent of the rituals of an OCD” (Beumont et al., 1994: 28), indicating cognitive strategies and behavioral and somatic symptomatology consistent with both disorders (Adams et al., 2003). There are debates concerning how to classify sport addiction in relation to OCD: is sport addiction a form of eating or body image disorder (which both have obsessive qualities) (Schlegel et al., 2015), an obsessive-compulsive spectrum disorder (Gulker et al., 2001), a disorder of its own that may exacerbate obsessive-compulsive symptomology (Davis et al., 1998) or merely a symptom of OCD to relieve or avoid emotional distress (Pinna et al., 2015)?
Conversely, other studies have argued that OCD could be a precursor and risk factor for the development of sport addiction due to the potential anxiolytic effects of the addictive exercise behavior (Berczik et al., 2012). The term “compulsion” (n = 22) also serves to frame sport addiction as an illness that manifests primarily through compulsive qualities. Viewed as compulsion, sport addiction has an anxiety-reducing function and focuses on behavioral features, such as rigidity and driven exercise routines. Resonating with the release vector, this framing emphasizes how exercise addiction provides an outlet to deal with constraining norms. Finally, in another 24 papers, sport addiction is conceptualized as a problem co-occurring with other psychiatric disorders, with depression (n = 22) and anxiety (n = 19) being the most significant.
In sum, the construction of sport addiction can be read through the lens of positivist and social constructivist paradigms. In a context where the field of psychology holds the greatest authority over the diffusion of the label, we can affirm that the positivist model dominates. With the objective of moving beyond linear interpretations and offering a contextualized account of the construct, we turn our attention to Hacking's subsequent vectors to explore the interplay between medical categories, clinical observations, social consequences, and possible functions.
Observability vector
Hacking's observability vector examines how and by which means the problem is (1) rendered visible and (2) interpreted as a problem, thereby reframing exercise as a potentially unhealthy behavior. The most common symptomatologic elements can be put in direct relation to the components included in tests and tools designed to assess sport addiction. Hence, this vector reveals that an individual can “fall ill” from sport addiction when a combination of various perturbations is observed in everyday life. We’ve classified these into five categories: classical indicators of addiction, physical, psychological, behavioral and social manifestations of sport addiction.
The first observation is the dominance of psychological symptomatology, mentioned in 231 papers, used to objectify sport addiction. The following psychological components are the most prominent: mood state alterations (n = 59), such as irritability, anxiety, and depression; feeling compelled to exercise (n = 38); loss of control (n = 34), rigidity, including ritualized and stereotyped behaviors (n = 40); fatigue (n = 17); and denial (n = 8). A second finding is the preponderance of classical indicators of addiction (n = 221), namely, withdrawal, salience and increased tolerance. This is unsurprising considering that the addiction, psychological and multidimensional frames rely on these indicators to assess and evaluate sport addiction. The most-cited withdrawal symptom is psychological distress in response to deprivation (n = 43). Physical symptomatology is highlighted in 126 research papers, where main descriptors are ignoring injuries (n = 48) or medical advice (n = 13); physical injury, injurious behavior, or overuse syndrome; (n = 47); and menstrual irregularity (n = 10).
As for common behavioral responses (n = 88), they primarily involve increased food surveillance (n = 36) or starvation (n = 6); substance abuse behavior, such as doping (n = 13); or use of food supplements (n = 5). In terms of social consequences (n = 104), decay in interpersonal relationships (n = 49) and vocational disruptions (n = 37) are the most significant indicators in our data. The frequency of these everyday observations provides useful information on the components being studied or included in the tests and tools of diagnosis and evaluation. Notably, very few qualitative studies appeared in our data corpus and many primarily aim to validate an instrument tool.
Tests and assessment tools for sport addiction: a global portrait
The most popular sport addiction assessment tools have been examined elsewhere (Adams and Kirby, 2002; Hauck and Blumenthal, 1992; Lichtenstein et al., 2017), concluding that “there is no consensus about the way to identify and categorize the phenomenon” (Lichtenstein et al., 2017: 86). Here, we offer a global picture of these tests by presenting turning points in how sport addiction has been measured. First, we identified 86 tests and screening tools (Figure 3 shows the 10 most-cited measurement tools) designed to evaluate the various facets of sport addiction. Over 74% (n = 64) of these tests appear in only one or two publications. Aside from ten measurement tools that appeared in articles between 1979 and 1999, 87.4% were designed after the year 2000.
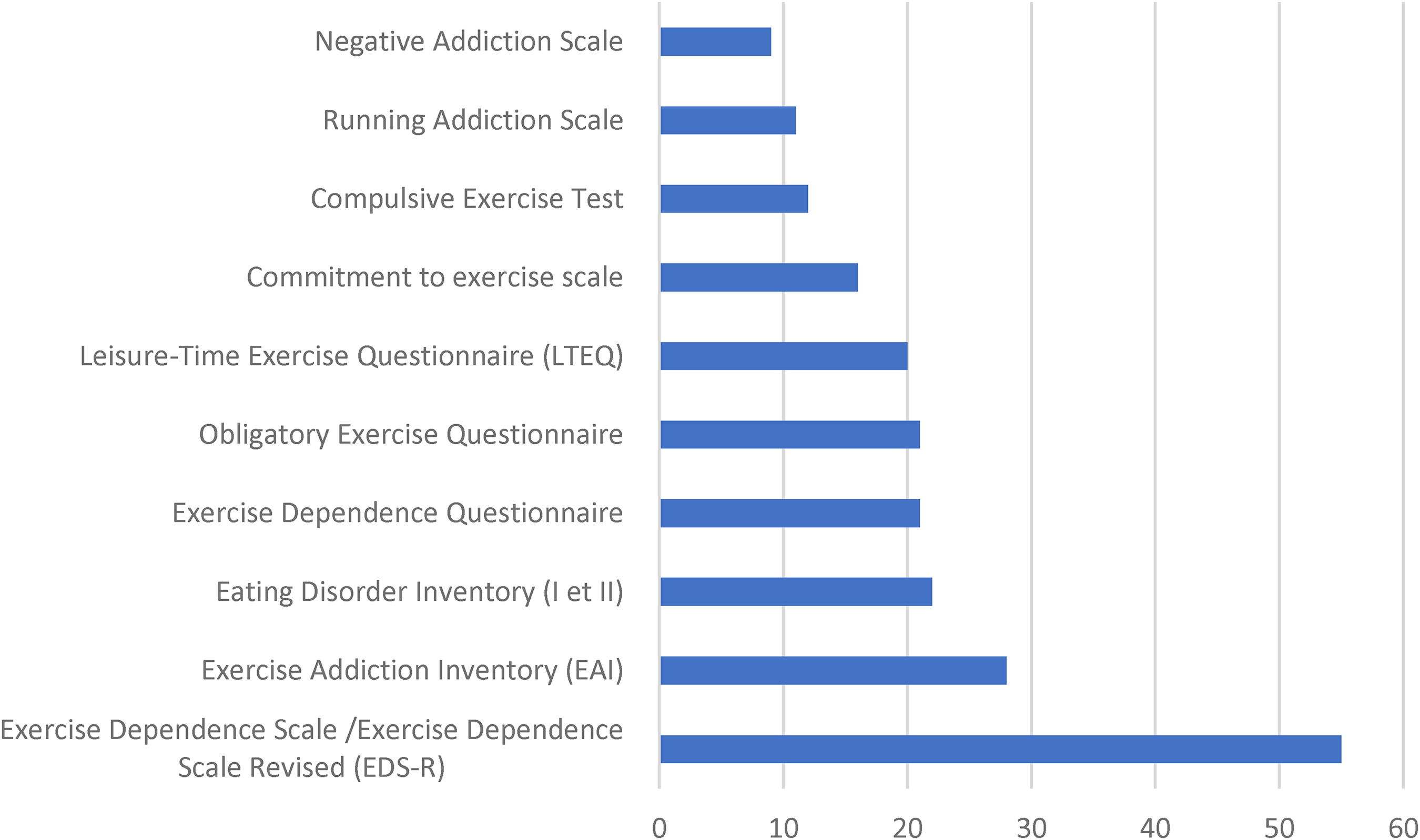
10 most-cited measurement tools for sport addiction (1979–2017).
From positive to negative addiction
Carmack and Martens’ (1979) Commitment to Running Scale, cited in 13 articles, was the first psychometric assessment designed for exercise dependence and was based on the premise that it was a positive addiction. The Running addiction scale (Estok and Rudy, 1986), mentioned in 11 studies, was the first instrument produced to measure negative addiction to running.
From secondary to primary disorder
The idea that exercise dependence was secondary to an eating disorder dominated the literature in the 1990s and several tests showcase this trend. The Obligatory Exercise Questionnaire (Pasman and Thompson, 1988) (n = 21) was designed to measure exercise dependence in relation to eating disorders and was cited mostly in the 1990s, but lost momentum after 2010, when it was cited only 5 times. This coincides with the creation of Ogden et al. (1997) Exercise Dependance Questionnaire (EDQ), which aims to reflect primary exercise dependence, and, later, with the growing popularity of Hausenblas and Downs’ EDS, which assesses for primary exercise dependence by first eliminating the possibility of an eating disorder diagnosis. Reflecting the scientific interest in the link between sport addiction and eating disorders (or the willingness to show that exercise dependence exists in a primary form), the third-most-cited assessment tool in sport addiction research is the Eating Disorder Inventory I and II (Garner et al., 1983) (n = 22) and, more specifically, its Drive to Thinness subscale, most often used to determine risk factors for primary exercise dependance.
From unidimensional to multidimensional
Earlier measures of sport addiction, like the quantification-based Godin Leisure-Time Physical Activity Questionnaire (Godin and Shephard, 1997) (n = 20) assessed the issue by means of unidimensional scales. With the development of the EDQ (Ogden et al., 1997) (n = 21) sport addiction started being considered a multidimensional construct in psychometric testing.
These ideas regarding multidimensionality and primary addiction are supported by Hausenblas and Downs’ EDS, the most-cited measurement tool in our data (n = 55). These authors have operationalized exercise dependence as a multidimensional construct based on the DSM-IV criteria for substance dependence or addiction such as tolerance, withdrawal effects, continuance, lack of control, reductions in other activities, time, and intention. This 21-item test has been revised and translated into multiple languages and distinguishes between individuals who are at-risk, have some symptoms, or have no symptoms of exercise addiction. In line with the establishment of multidimensional measures, the second-most-cited assessment tool is the Exercise Addiction Inventory (EAI) (n = 28) designed by Griffiths et al. (2004).
To conclude this section, while they differ in their specific measurement goals, these 86 tests and tools all seek to provide evidence for the existence and empirical investigation of sport addiction, a syndrome that, until the 2000s, had been mainly constructed on speculations. Validation of measurement instruments seems a primary concern for researchers in the field of sport addiction, indicating that research in this field is still exploratory rather than confirmatory.
Cultural polarity vector: fostering ambivalence
The debate around the positive and negative consequences of sport addiction is central to understanding how the construct is portrayed as holding an “in-between position” (Brossard, 2019: 237). In response to William Glasser's book Positive Addiction (1976), which distinguished between positive and negative addiction and claimed that sport was a positive one because it produced psychological strength, Morgan (1979) was the first to propose that sport addiction was a “negative addiction” as it could become a distortion of normal behavior.
Reflecting this constantly-reinstated polarized view of sport addiction, most papers subsequent to Morgan's begin with a sentence that first highlights the positive aspects of exercise before introducing the idea of exercise as pathology, thus positioning exercise as being both healthy and possibly unhealthy: Physical exercise improves cardiovascular health, strengthens muscles and bones, promotes neuroplasticity, decreases anxiety, offsets depression and more generally promotes feelings of wellbeing. However, when taken to extremes, exercise can result in a behavioural addiction (Fattore et al., 2014: 279).
Identification of criteria by the scientific community allows the category to move toward the negative pole. Albeit, as illustrated in the few qualitative articles available, exercise addiction reflects a more nuanced representation in the real world. Indeed, the positive outcomes can outweigh the potential harms: Even when considering these contradictions these individuals did appear to be making an informed and rational choice to exercise in the way they did, with possibly harmful consequences viewed as being outweighed by a desire to achieve their goals (around body, control, fitness) and enjoying the activity (Cox and Orford, 2004: 86).
At a social level, as observed in 11 papers, sport addiction is also viewed as a socially acceptable behavioral addiction or even favorable compulsion for various reasons: it is a mood regulator, a tool to fit in with the prominent healthism discourses and a way for people to perform their individuality. The available social figures of sport addiction further this ambivalence.
Social figures of sport addiction: expanding ambivalence to the social sphere
With the rising popularity of the online Fitspiration trend, excessive sport is being glorified in the media (Holland and Tiggemann, 2016). Within this fitness culture, some authors note how certain trends can foster the development of sport addiction in certain populations, like triathletes or marathon runners. As noted by Håman et al. (2017: 2), aggressive fitness norms that legitimize and even promote unhealthy fitness behavior, “contribute to push the boundary lines of health norms regarding conformal healthy behaviors to a more extreme level, since unhealthy behaviors become normalized and socially accepted”.
In another study on the culture of thinness in sports, Atkinson (2011: 247) further explains: “After they have learned acquiescence to groupthink processes, some athletes become bombarded with pro-thinning beliefs and practices to the extent that regular bouts of intense slimming are normative, rather than deviant or pathological, components of sport culture”. These blurred boundaries between healthy and unhealthy exercise are rendered visible mainly through studies of extreme sports and further Hacking’s (1998) cultural polarity vector, which considers that growth and promotion of a disorder is facilitated by its ability to sit between historically located vice and virtue.
Interestingly, we observed that sport addicts are being evaluated and described in terms of socially valued characteristics. Prominent figures mentioned in sport addiction literature include The Type-A (n = 6), The Extrovert (n = 6), The High or Overachiever (n = 5), or The Adrenaline Junkie (n = 3). On the other end of the spectrum, the sport addict is also described in less socially acceptable terms, thus making the addict an undesirable social figure—for example, The Obsessive-Compulsive (n = 24), The Narcissist (n = 12) and The Neurotic (n = 6). Perfectionism (n = 27) and hyperactivity (n = 7) offer an in-between position: while these traits can be viewed positively in the social world due to performance-driven norms, they are deemed psychologically disruptive in terms of ability to self-regulate and are related to negative traits, such as rigidity or restlessness.
To summarize, our data supports the claim that sport addiction rests as an in-between category where taking sports to extremes can be both enviable (as it responds to normative injunctions of health, beauty, and productivity) and frowned upon (because it also depicts a negative representation through traits deemed undesirable in the Western social world, including neuroticism, denial, and psychological weaknesses).
Who is targeted?
We found that 14.3% (n = 54) of sport addiction studies specifically target women and 11.4% (n = 43) target men. Considering the number of studies that link sport addiction to eating disorders, this could be partly explained by the fact that eating disorders have been constructed as a women's issue and scientific interest in male experiences of eating disorders is relatively recent (Zhang, 2014).
Concerning the types of sports, we found that running (n = 35) was most often mentioned, followed by weightlifting (n = 20) and bodybuilding (n = 15), which are cited mainly in papers on muscle dysmorphia. Finally, marathons/triathlons (n = 16), high risk sports (n = 6) and cycling (n = 6) represent other types of sports identified in scientific literature.
Release vector
In terms of release, this vector affirms that the trouble provides a way out for people who are unable to access the social materials (the means) that would allow them to achieve certain normative cultural objectives (the goal). Sport addiction seems to provide four general areas of release.
Body image concerns
In this case, sport addiction (the means) is used to achieve the cultural goal of an ideal body or self. The goal of changing the body is often mentioned (193 articles refer to body image concerns to explain underlying motives behind excessive exercise). The motives include change in body weight (n = 69) or body shape (n = 46), drive for muscularity (n = 29), drive for thinness (n = 16), aesthetic outcome (n = 15) or drive for muscle tone and leanness (n = 7), as well as the need to alleviate body dissatisfaction (n = 7) or the fear of fat (n = 3).
Social status
People may also “fall ill” from sport addiction to achieve a certain social status (n = 27)—through adherence to a valued sport subculture, for example. Also, when one has labile self-esteem, excessive exercise becomes a means to validation and social recognition: Regarding external regulation, it is possible that, at first, exercise dependence is a consequence of recognition and appreciation by others (e.g. expressions such as “you are so thin” or “you are so strong”) and that this feeling is later internalized and becomes an introjection (Sicilia and Gonzales-Cutre, 2011: 326).
At an existential level, it can also fill a void (Valleur and Valéa, 2009) or provide a sense of meaning and identity, as in Partington et al.’s (2009: 181) qualitative study: “It comes back to that ego and that searching for a fulfillment”.
Arousal-seeking
Of interest is the finding that euphoric effects of exercise, known commonly as runner's high or scientifically as the endorphin-hypothesis, is most often mentioned as a release rather than an explanation for sport addiction. This feel-good factor was mentioned in 34 papers to experience elation or to arouse the senses. Cox and Orford’s (2004: 176) qualitative data illustrates: I got a buzz from the other stuff, from running and swimming, I got a buzz because it makes you feel so good … there's that … what I call a “sweet” moment when everything comes together, when you get everything right when you’re doing your sport … and it feels great.
These descriptions hint at the types of release “sport addicts” are searching for: “a desire to recreate the feelings experienced [when exercising]” (Partington et al., 2009: 182); “a quest for excitement” (Dunning and Waddington, 2003: 362); or, as one qualitative research participant describes it, “The relief of reaching the top of something hard is close to elation” (Heirene et al., 2016: 337). Interestingly, the neurological descriptions of elation derived from brain disease models of sport addiction appears reductionist compared to the latter phenomenological accounts of “sport addicts”. Experiential discourse indeed creates space to expand on the felt and lived experience of “sport addiction” and rethink pleasure, perhaps as a “site of innovation” (Keane, 2021: 4) or as a “practice of freedom” (Rose, 1999: 61).
Coping
Addiction to sport provides an array of benefits, offering the addict a way to cope with or respond to cultural or social demands. While some may use exercise to self-regulate mood, as cited in 74 articles, others turn to excessive exercise for avoidance or escapism (n = 30). Exercise as a means of control and security appears in 22 articles, as in Kolnes (2016: 16): “Accordingly, the use of extensive exercise […] to relieve and escape bodily distress and embodied feelings, gives her a sense of disruption and a feeling of control”. Also noteworthy are the studies (n = 6) that have attributed sport addiction to past abuse or trauma. Finally, others have demonstrated that sport addiction can be a compensatory behavior (n = 21) to respond to social ideals, by compensating for either a devalued social identity or an internalized lack of masculinity.
Discussion
This sociohistorical analysis of literature shows that the scientific realm has produced a myriad of studies on sport addiction despite its absence in leading classification systems. Nevertheless, no consensus has been reached on the ontology, definitions, and investigation methods of sport addiction. How has this category been able to evolve and gain strength within the scientific field without being recognized by the medical and psychiatric fields?
We first hypothesize that the tendency of an increasingly diverse population to take sports to extremes (Zhou et al., 2020), where ordinary people partake more frequently in extreme competitions is “pushing the boundary lines of health norms regarding conformal health behaviors to a more extreme level” (Håman et al., 2017: 5). Hence, as in the cultural polarity vector, social acceptability of extreme behaviors may not only produce new ambivalent social figures but may also render sport addiction a more valuable construct as it “fits” with new health norms, rendering it a hypernormative-type of behavioral addiction (Moreau et al., Submit). This process also reveals the “sport addict” as a subject of modern governance responding to the neoliberalist demands of self-optimization (Harbusch, 2022), where some are taking to the extremes “the positively valued activities that are promoted as obligatory habits of health” (Keane, 2021: 3).
Second, the upsurge of corporeal media trends, such a “fitspiration” (Raggatt et al., 2018), provide idealized images of the modern athletic and healthy body, which, in turn, produce new physical standards (Prichard et al., 2020), as highlighted in the release vector. In this context, exercise becomes a means to reach evolving and often unattainable health and fitness norms, therefore creating a “contextual container” (Reinarman and Granfield, 2014: 16) and opening up new discursive spaces from which sport addiction can expand, creep into the everyday lives of “ordinary people” (Reinarman and Granfield, 2014: 1) and even be normalized.
Third, despite the power held by the medical field in organizing and legitimizing categories (Carney et al., 2018), psychology currently holds authority over the label and sustains it within the scientific field, as in the medical taxonomy vector. Indeed, considered a “generous field” (Rose, 1996: 87), psychology lends itself easily to various “agents of social authority” and can “render rational the grounds of decision and action”. But is psychology alone powerful enough to keep the category alive?
Contrary to other behavioral addictions whose social recognition did not rely on typical categorization processes—sex addiction, for example (Larocque et al., 2022)—sport addiction seems to lack the consistency necessary to hold the attention of various medical and non-medical stakeholders, as in the observability vector, where an array of assessment tools exist but have not yet provided a coherent measure (Lichtenstein et al., 2017). Also, what differentiates sport addiction from other behavioral addictions is its inherently positive relationship to the medical world. Perhaps the idea of exercise as therapy or as medicine—that is, exercise as a virtue, as per the cultural polarity vector—is too well-anchored for medical experts to define exercise as pathology or as vice. Indeed, the moral panic (Reed, 2015) associated with chronic disease as a known public health issue is greater than the concern for excessive exercisers, a population whose prevalence is still widely debatable. This highlights the strength and fragility of the sport-health ideology: the link between sport and health may be strong in the medical realm but still delicate in the public sphere.
Study limitations
Hacking's framework was particularly useful to study how sport addiction is uniquely being appropriated in the scientific field. However, as per recent studies of emerging classifications (Brossard et al., submitted), analysis of one field (scientific, in this case) does not necessarily signal the stabilization of a mental health category. Indeed, extending the research beyond academe to fields where sport addiction is being deployed is essential to gain a comprehensive understanding of categorization processes and of contemporary politics of labeling. Multiplying sites of observation (Marcus, 1995) and expanding the fieldwork beyond a specific place or timeframe (Desmond, 2014) would further account for the actors and “interest groups” (Reinarman and Granfield, 2014: 1) involved in the diffusion of the concept and their vested interests. If our focus on the scientific production of the construct of sport addiction illuminated the pervading methodological, theoretical, and epistemological debates within this field, it did not allow to account for these multiple actors and power dynamics. Our methodology represents another limitation, as it does not correspond to a meta-analysis or pure systematic review. In this context, rigorous criteria found in Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA), were not implemented. One limitation of this intuitive approach to criteria selection relates to the possibility of missing significant studies, which we may have also missed by limiting our inclusion criteria to French- and English language articles. However, this approach did provide sufficient data to reach saturation point and offer a comprehensive view of existing data on sport addiction. Also, the medical taxonomy vector was especially complex to code due to elastic boundaries of the construct, thus resulting in overlapping categories. Despite these limitations, our methodology and analytical process allowed us to operationalize Hacking's vectors as a strategy to surpass descriptive elements.
Conclusion
To conclude, utilizing Hacking's framework to study the evolution and appropriations of sport addiction within the scientific field fills an important gap in literature. While providing a contextualized account of the emergence and diffusion of the construct, it also extends analysis beyond traditional medicalization studies, which have classically focused mainly on the medical jurisdiction (Conrad, 2013). The medical taxonomy vector revealed certain epistemological and methodological issues and debates that resonate with fields outside sport addiction and the sciences. In a previous article (Roy et al., 2019), we showed that publication of the DSM-5 prompted severe criticism and controversies in the media as several paradigms collided, as in the case of sport addiction (conformist vs. reformist, conflictual vs. constructivist, etc.). These represent classical contemporary debates in mental health, where the boundaries between psychological, biological, and social etiologies are porous.
While our analysis revealed the prominence of psychology in the diffusion of the construct, its expansion and legitimation may necessitate greater social adhesion stemming from bottom-up, consumer-based movements, which often drive the wider diffusion and recognition of mental health categories (Barker, 2007). Some questions remain: are laypeople who take exercise to extremes willing to push for social and medical recognition of their subjective, embodied distress, thereby taking the lead in the medicalization of excessive exercise? Or, is adherence to the idea of sport-as-virtue too strong for this process to unfold in the social sphere, thus rendering sport addiction susceptible to failed medicalization?
Footnotes
Acknowledgements
The authors would like to offer special thanks to Baptiste Brossard, Mélissa Roy, Julien Thibault-Levesque, Ben Hemmings and Brice Favier-Ambrosini, who provided invaluable insights and expertize that greatly influenced our thought and writing process. We also extend our gratitude to Joëlle Moncrief for assistance with data collection, to Kate Finnigan for her editing services and to the reviewers whose comments allowed to enhance the quality and rigor of this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Social Science Research Council (grant number no 435-2018-0729).
Data availability
There is currently no data set associated with this paper. The data that support the findings of this study are available from the corresponding author [EL] upon reasonable request.