
Abstract
Stratification of colorectal cancer for better management and tangible clinical outcomes is lacking in clinical practice. To reach this goal, the identification of reliable biomarker(s) is a prerequisite to deliver personalized colorectal cancer theranostics. Osteopontin (SPP1) is a key extracellular matrix protein involved in several pathophysiological processes including cancer progression and metastasis. However, the exact molecular mechanisms regulating its expression, localization, and molecular functions in cancer are still poorly understood. This study was designed to investigate the SPP1 expression profiles in Saudi colorectal cancer patients, and to assess its prognostic value. Hundred thirty-four (134) archival paraffin blocks of colorectal cancer were collected from King Abdulaziz University Hospital, Saudi Arabia. Tissue microarrays were constructed, and automated immunohistochemistry was performed to evaluate SPP1 protein expression patterns in colorectal cancer. About 20% and 23% of our colorectal cancer samples showed high SPP1 cytoplasmic and nuclear expression patterns, respectively. Cytoplasmic SPP1 did not correlate with age, gender, tumor size, and location. However, significant correlations were observed with tumor grade (p = 0.008), tumor invasion (p = 0.01), and distant metastasis (p = 0.04). Kaplan–Meier survival analysis showed a significantly lower recurrence rate in patients with higher SPP1 cytoplasmic expression (p = 0.05). At multivariate analysis, high SPP1 cytoplasmic expression was an independent favorable prognostic marker (p = 0.02). However, nuclear SPP1 expression did not show any prognostic value (p = 0.712). Our results showed a particular SPP1 prognostic relevance that is not in line with most colorectal cancer previous studies that may be attributed to the molecular pathophysiology of our colorectal cancer cohort. Saudi Arabia has both specific genomic makeup and particular environment that could lead to distinctive molecular roots of cancer. SPP1 has several isoforms, tissue localizations and molecular functions, signaling pathways, and downstream molecular functions. Therefore, a more individualized approach for CRC studies and particularly SPP1 prognosis outcomes’ assessment is highly recommended toward precision oncology.
Introduction
The ultimate goal of precision oncology is to maximize chances of successful treatment outcome by accurately stratifying cancer patients in order to deliver the appropriate treatment plan. However, the implementation of such approach is still challenging.1,2 This challenge is mainly due to the poorly understood interactions between the genome, the environment, and lifestyle, which contribute to the inherent plasticity, heterogeneity, and complexity of cancer.3,4 Therefore, the management/treatment of cancer remains extremely challenging and particularly in the case of colorectal cancer (CRC). Despite the use of multimodal treatment approaches based on the TNM staging system, 5 the prediction of CRC patients’ outcomes is variable and not consistent even for those within the same stage. 6 In fact, the median survival of patients with in-operable metastatic CRC remains less than 3 years. However, currently available combinations of chemotherapy, radiation treatment, and surgery could provide a 5-year survival of 26% to 40% of CRC patients with resectable advanced disease. 7 Therefore, there is an urgent need to identify new reliable molecular prognostic biomarkers that could more accurately stratify the patients according to their genomic blueprint for better management and more individualized theranostics. 8 Currently, huge efforts are being made to detect novel biomarkers with possible diagnostic, prognostic, and/or predictive value in order to alleviate the burden of CRC.9–11 Although several potential markers have been evaluated, a reliable diagnostic and/or prognostic biomarker(s) allowing effective stratification of patients with high risk of relapse and/or those who may be benefited with adjuvant therapies for better outcomes is still lacking in clinical practice. Therefore, there is a pressing medical need to identify more accurate molecular markers to predict and improve the prognosis of CRC patients.
Secreted phosphoprotein 1 (SPP1)—also called as Osteopontin (OPN)—is a matricellular protein, which has been reported to be differentially expressed in a variety of cancer cells. It is a phosphorylated sialic acid–rich noncollagenous bone matrix protein, belonging to small integrin-binding ligand N-linked glycoprotein (SIBLING) family. SPP1 is encoded by gene spp1, which is located in the human chromosome 4 (4q21–4q25) consisting of seven exons with highly conserved promoter. 12 Elevated levels of SPP1 have been detected in cancer cells and body fluids of patients including blood, urine, and bile. 13 Numerous studies have demonstrated that SPP1 expression in CRC is associated with poor prognosis and short overall survival. It is suggested to play an important role in several tumor-associated processes including invasion, migration, angiogenesis, inflammation, and metastasis. 14 The exact molecular mechanisms regulating the expression of SPP1 in malignant cells are still poorly understood. It has been shown that SPP1 promotes tumorigenesis through cell–ECM (extracellular matrix) interactions and by regulating signaling pathways through binding with integrin and CD44, a multifunctional cell surface adhesion receptor involved in metastasis. 15 Using CRC cell lines, overexpression of SPP1 has been reported to be associated with higher invasion, faster disease progression, and metastatic dissemination. 16 Numerous studies have suggested SPP1 overexpression as possible predictor of poor prognosis in CRC.17,18 However, so far reported results on the association between SPP1 expression and its prognostic value in CRC have been largely inconsistent and sometimes contradictory.17,19–23 Therefore, the current study was performed to study the SPP1 protein expression patterns in Saudi Arabian CRC patients and evaluate its prognostic value.
Patients and methods
Patients
The study was performed on paraffin blocks of patients diagnosed with colorectal adenomas (n = 41) and primary CRC (n = 134) at the Department of Pathology, King Abdulaziz University, Jeddah, Saudi Arabia. Patients included in the study did not receive any chemo or radiotherapy prior to surgery. Normal colorectal mucosae (n = 40) were taken from unremarkable mucosa in patients with diverticular disease, ulcerative colitis, ischaemic colitis, or Hirschsprung disease. The samples were used according to the guidelines of the Ethical Committee of King Abdulaziz University Hospital (KAUH) and the study was approved by the Research Committee of the Biomedical Ethics Unit, Faculty of Medicine, King Abdulaziz University. Patients gave an informed written consent prior to the surgery. The relevant clinicopathological features such as age, gender, stage, grade, and lymph node status, the follow-up, and survival data were collected from patient files and summarized in Table 1. The mean age at the time of diagnosis was 57 years (range: 15–92 years).
Clinicopathological characteristics of 134 CRC patients.

CRC: colorectal cancer.
Treatment and follow-up
The patients were seen at 3–6-month intervals until death or end of follow-up which was June, 2013. Some patients were lost from the follow-up. The mean follow-up time for the whole series was 24 months (range: 1–144 month). During the follow-up period, 33/134 (25%) patients developed recurrence and 22% of patients died of disease. Disease-free survival (DFS) and disease-specific survival (DSS) were calculated as the time from diagnosis to the appearance of recurrent disease or to the date last seen disease-free and time from diagnosis to death (due to disease) or to the date last seen alive, respectively. In calculating DSS, patients who died of other or unknown causes were excluded.
Tissue microarray construction
Tissue microarrays (TMAs) were designed and constructed as previously described 24 in order to identify suitable region on a donor tissue block. Briefly, hematoxylin- and eosin-stained sections of normal colorectal mucosae, colorectal adenomas, primary tumors, and nodal metastasis were examined by an experienced pathologist and areas of interest were chosen and marked on slides. Two tissue cores each 1.5 mm in diameter were punched from donor block(s) in an automated TMA instrument (TMA Master 1.14 SP3 from Histech Ltd. Budapest, Hungary) and inserted into a recipient paraffin block.
Immunohistochemistry
Paraffin blocks of constructed TMAs were cut at 4 μm, and mounted on positive-charged slides (Leica Microsystems Plus Slides). Sections were deparaffinized in xylene and rehydrated in an automated immunostainer (BenchMark XT, Ventana® Medical systems Inc., Tucson, AZ, USA). Pretreatment was done using prediluted CC1 (cell conditioning solution) for 60 min. Antihuman rabbit anti-OPN polyclonal antibody (Spring™ Bioscience; Cat E3284) was incubated at 37 °C for 20 min. Ventana® I-view DAB detection kit was used according to kit manufacturer instructions. Subsequently, slides were washed, counterstained with Mayer’s hematoxylin and mounted. Negative control (substitution of the primary antibody with Tris-buffered saline) and positive control slides were included.
Interpretation of SPP1 immunostaining
Sections were evaluated independently without knowledge of the clinicopathological characteristics of patients by two pathologists (W.G. and M.H.). The slides were observed under light microscope for immunostaining using a semiquantitative method based on a scale of staining intensity from 0 to 3. Grade 0 represented negative (–), grade 1: weak (+), grade 2: moderate (++), and grade 3: intense (+++). All slides were divided into two categories. Weakly stained specimens were considered as having low SPP1 expression, whereas moderate and intense samples were included in high expression category. For the interpretation of staining intensity positive control sample was taken as maximum intensity score of 3.
Statistical analyses
The statistical analysis was performed using the IBM SPSS Statistics Version 19.0 (IBM Company, USA) software package. Chi-square test (χ2) was used to examine the association between SPP1 expressions with various clinicopathological characteristics. Univariate survival analysis (DSS; DFS) was based on Kaplan–Meier method, with log rank test. DSS and DFS were calculated, based on the time from diagnosis to death (due to disease), and on the time from diagnosis to the appearance of metastatic disease or recurrence, respectively. Cox proportional hazards regression model was used to assess the value of SPP1 as independent predictor. The model was controlled for confounding by the following variables: age, lymph nodes status, grade (for DFS), and recurrence as additional variable (for DSS). The assumption of proportional hazards was controlled by log-minus-log (LML) survival plots. In all tests, the values p < 0.05 were regarded statistically significant.
Results
Expression patterns of SPP1
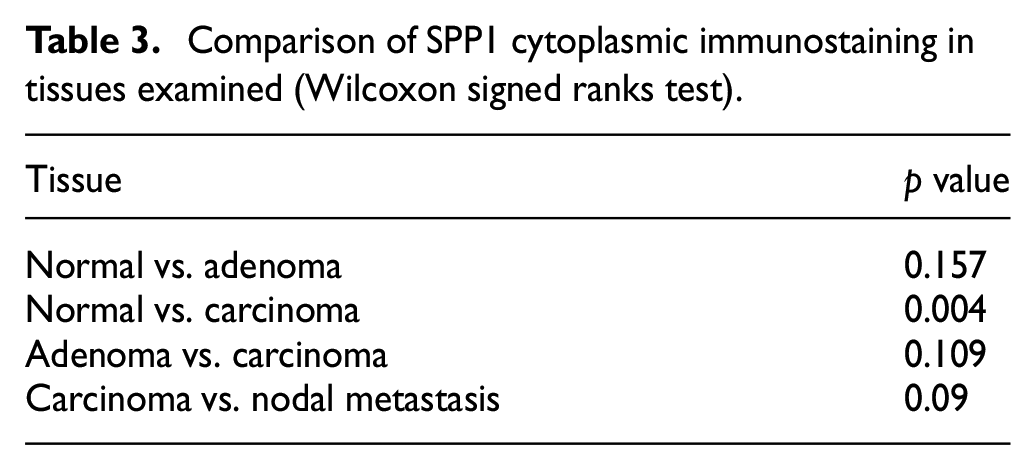
The expression patterns of SPP1 in normal, adenoma, CRC, and nodal metastasis are illustrated in Figure 1. SPP1 in normal colonic mucosa showed only cytoplasmic immunostaining at the apicolateral aspects of colonocytes (Figure 1(a)). In adenoma, dysplastic cells showed mostly apical cytoplasmic immunostaining that varies from weak to moderate. Nuclear immunostaining was weak. In CRC, twenty percent (20%) of all tumors revealed diffuse cytoplasmic expression patterns and about 23% of cases were positive in nuclei, respectively (Figure 1(c) and (d), respectively). In nodal metastasis, about 15% showed moderate/high cytoplasmic staining and 24% nuclear staining. There was no statistically significant difference between normal mucosa and adenoma. However, SPP1 immunostaining is statistically higher in CRC than in normal mucosa (p = 0.004). Further details are provided in Tables 2 and 3.
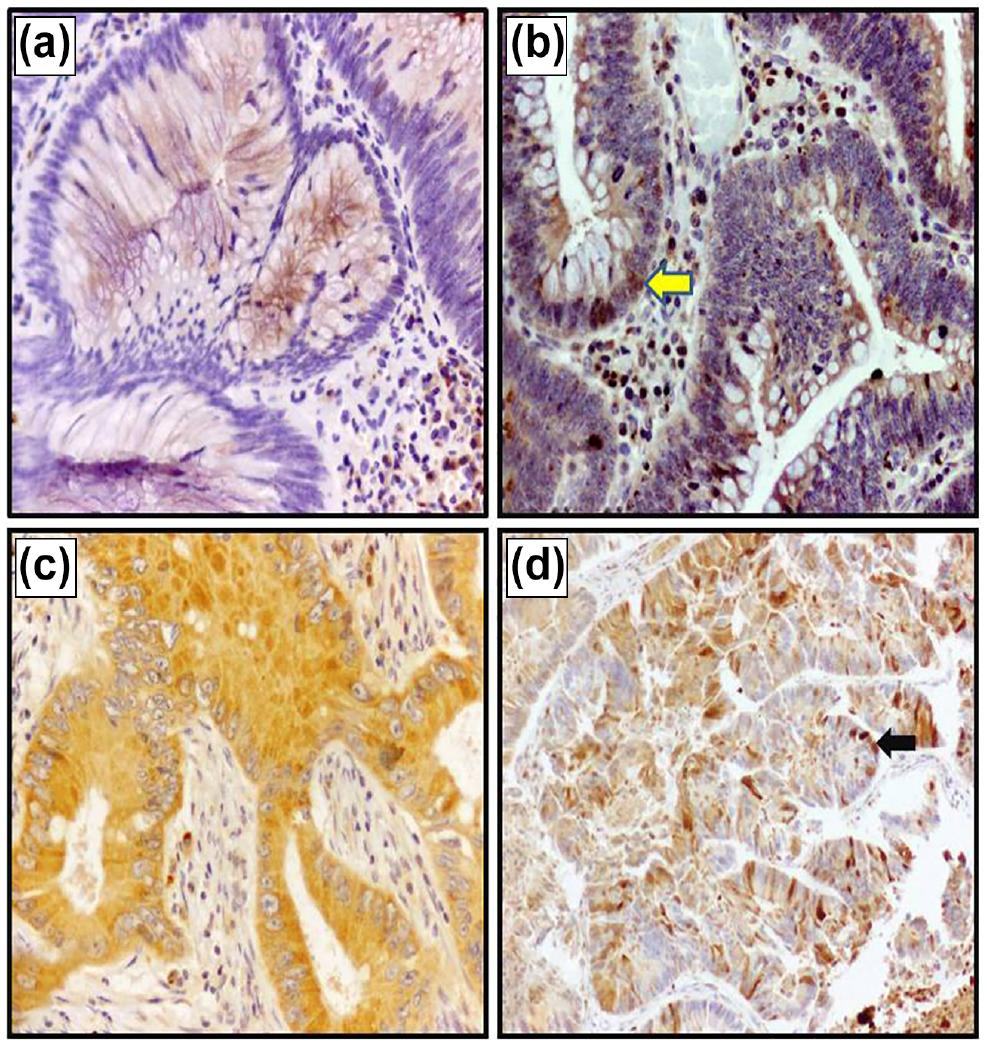
SPP1 immunostaining patterns. In normal mucosa, cytoplasmic immunostaining is shown in the apicolateral aspects of colonocytes ((a); 200×). In adenoma, immunostaining is shown in the apical portion in addition to weak nuclear immunostaining (arrow; (b); 200×). CRC samples showed diffused cytoplasmic immunostaining ((c); 200×) and cytoplasmic and nuclear (arrow) immunostaining ((d); 100×).
Categories of SPP1 cytoplasmic immunostaining in different tissues (one sample chi-square test).

Comparison of SPP1 cytoplasmic immunostaining in tissues examined (Wilcoxon signed ranks test).
Correlation of SPP1 cytoplasmic expression with clinicopathological features of CRC
By using different cut-off points to study the correlations between the expression patterns of SPP1 with different clinicopathological data, we found that the cut-off point of (0,1 vs. 2,3) i.e. (negative/weak vs. moderate/high) expression pattern profile was the most suitable discriminator for correlating expression patterns with clinical follow-up data. The present study revealed that there was no correlation between the gender, age, tumor size, and tumor location. However, a borderline association was seen between SPP1 expression and lymph node involvement (p = 0.06). Interestingly, highly significant negative correlations were observed between the SPP1 expression patterns profile and distant metastasis (p = 0.04), tumor invasion (p = 0.01), tumor grade (p = 0.008), and recurrence (p = 0.05). Accordingly, tumors with low SPP1 expression showed high tendency toward distant metastasis than those tumors with high SPP1 expression patterns. Moreover, patients with low SPP1 expression had both poorly differentiated tumors and higher invasion tendency compared with those with high SPP1 expression patterns. Furthermore, tumors with low SPP1 expression patterns showed higher rates of recurrence than those with high expression profile (Table 4).
Correlation of Osteopontin expression patterns and clinicopathological features of 134 CRC patients.

CRC: colorectal cancer.
Correlation of SPP1 cytoplasmic expression with patients’ survival outcomes
It is important to highlight that although SPP1 was expressed in the cytoplasm and nuclei, the nuclear expression patterns did not show any significant trend in both DFS (p = 0.712) and DSS (p = 0.975; data not shown). In univariate (Kaplan–Meier) analysis (at low, intermediate, and high expression cut-off points), there were significant differences in survival outcomes between patients with different SPP1 cytoplasmic expression patterns, in which SPP1-positive patients had more favorable disease/recurrence-free survival (DFS; p < 0.05, log rank; Figures 2 and 3) than patients with low and/or intermediate cytoplasmic expression profiles. Interestingly, at 2 years of follow-up time, 95% of patients with high SPP1 cytoplasmic expression patterns were alive free of disease as compared with 50% of patients with low SPP1 cytoplasmic expression patterns. More importantly, at 5 years of follow-up time, all patients with tumors of low SPP1 expression patterns showed recurrence while only 17% of those patients with tumors of high SPP1 expression patterns relapsed (i.e. 83% are recurrence/disease-free). In addition, patients with intermediate SPP1 expression behaved better than those with low SPP1 expression patterns (Table 5). In contrast to DFS, SPP1 expression patterns had no significant correlation with DSS (p = 0.6, log rank, Figure 4), although a better DSS trend for patients with tumors of high SPP1 expression patterns was observed. To determine the independent prognostic factor with respect to DFS of patients, SPP1 was included in the Cox proportional hazards model, along with the other clinicopathological factors including early onset, tumor grade, and lymph node metastasis. Multivariate analysis confirmed that high SPP1 expression was an independent favorable prognostic marker in terms of DFS with a hazard ratio of 0.414 indicating that cancers with high SPP1 expression are 2.4 times less likely to recur (p = 0.02).
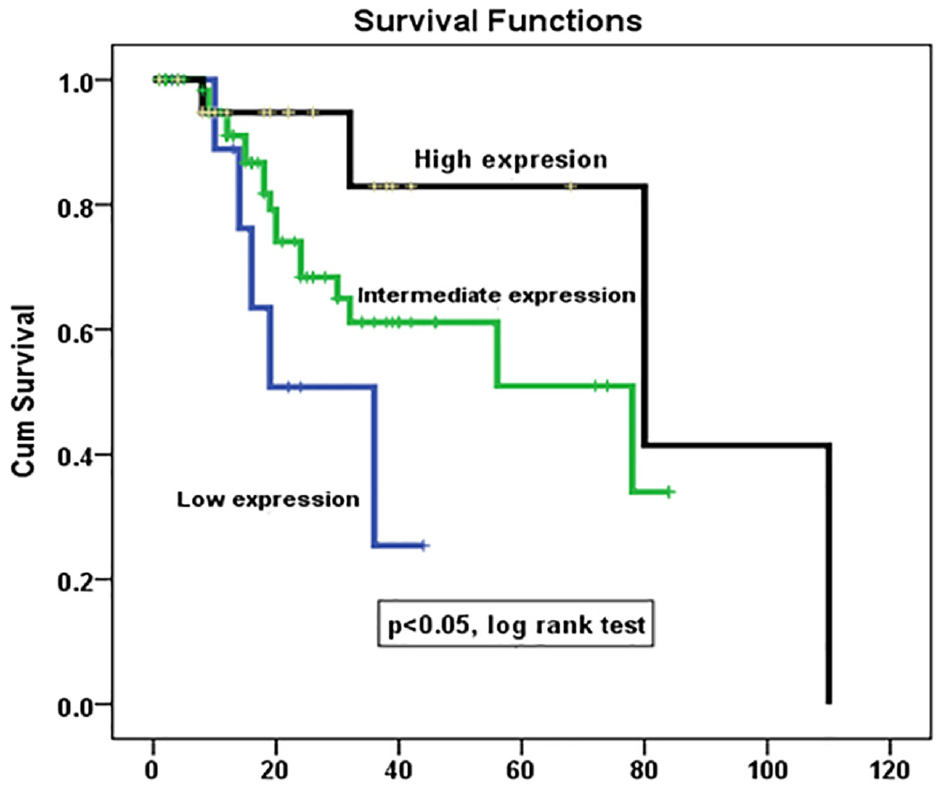
SPP1 protein cytoplasmic expression pattern profile (low, intermediate, and high expression) as a determinant of disease-free survival (DFS) of CRC in univariate (Kaplan–Meier) analysis (p = 0.05, log rank test).

SPP1 protein cytoplasmic expression patterns profile (low vs. high expression) as a determinant of disease-free survival (DFS) of CRC in univariate (Kaplan–Meier) analysis (p = 0.09, log rank test).
DFS outcomes of CRC patients according to OPN expression patterns profile.

DFS: disease-free survival; OPN: Osteopontin; CRC: colorectal cancer.
p < 0.05.
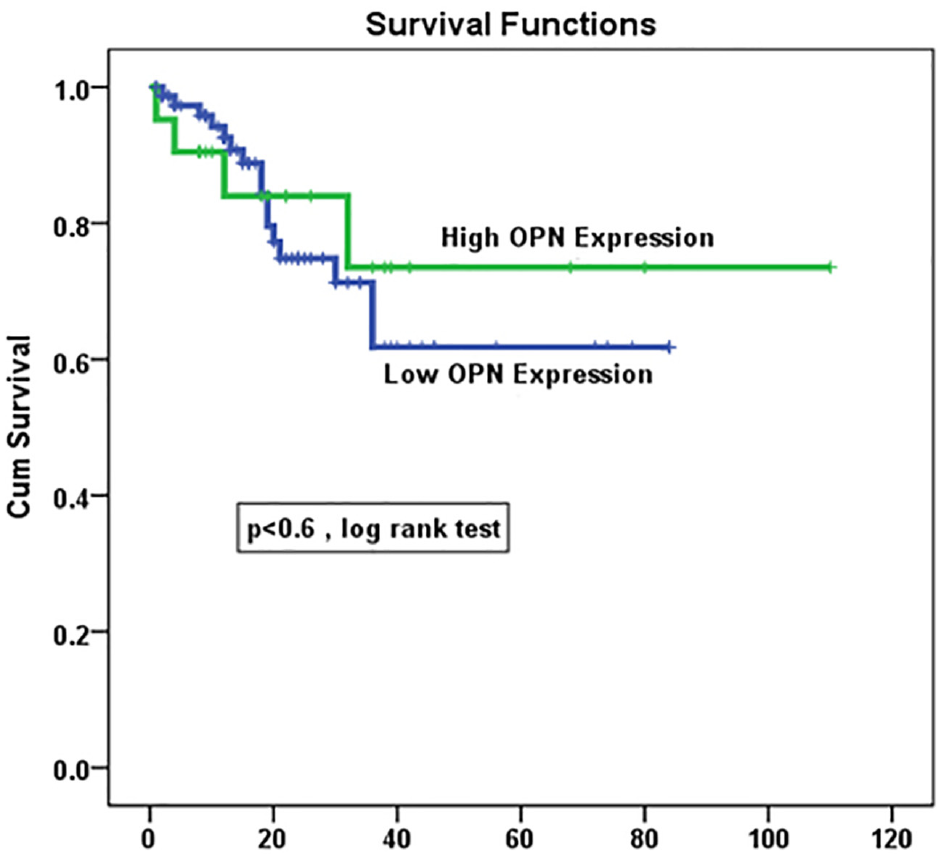
SPP1 protein cytoplasmic expression patterns profile (low vs. high expression) as a determinant of disease-specific survival (DSS) of CRC in univariate (Kaplan–Meier) analysis (p = 0.6, log rank test).
Discussion
Despite some achievements, the precision oncology approach launched since the completion of the human genome project with several initiatives and consortia is still in its infancy. 1 Thus, in order to better estimate an individual patient’s chances of harboring clinically silent micrometastatic disease and to assess recurrence risk, the integration of reliable prognostic information provided by genomic testing and clinicopathological factors is critical for bedside tangible outcomes.9,25 However, it is highly challenging task particularly for cancers with higher rate of worldwide occurrence and those characterized by various histotypes such as CRC.3,4 These histotypes demonstrate high level of variability in cancer onset and progression, metastatic pattern, chemotherapeutic response, resistance development, and clinical outcome. The use of conventional multimodal treatment approach for CRC, directed by the TNM staging system, 5 showed a lack of enough resolution to accurately predict the outcome of patients within the same stage. It is well-established in clinical practice that a subgroup of patients within stage II is at high risk of disease recurrence during their life time and should be considered for adjuvant chemotherapy as well as watchful follow-up. 6 Therefore, finding additional molecular markers that can help in pinpointing the survival outcome and/or treatment response of a group of patients within the same stage will be extremely valuable toward better management and personalized treatment. 8 A large number of biomarkers with potential diagnostic, prognostic, and/or predictive value were investigated.9–11 Among these biomarkers, SPP1 (OPN, 34 kDa protein) has been reported to be involved in tumor progression, metastasis and suggested as a promising prognosis/therapeutic target biomarker.15,22,23,13 In this context, this study was tailored to investigate the SPP1 expression profiles in Saudi CRC patients to assess its prognostic value and to obtain additional insights on possible molecular mechanisms influencing its expression and molecular functions.
The IHC expression patterns of our CRC patients’ cohort and their correlations with the survival outcomes results suggested SPP1 cytoplasmic overexpression as a significant favorable prognostic marker (Figures 2 and 3). For SPP1 nuclear expression, no prognosis value has been shown. In fact, SPP1 cytoplasmic expression in CRC was higher compared with normal mucosa. Interestingly, lower cytoplasmic expression of SPP1 in Saudi CRC patients was significantly associated with tumor invasiveness and disease recurrence. Therefore, CRC patients of our cohort with higher SPP1 cytoplasmic expression exhibited significantly improved DFS compared with those with low SPP1 levels. In addition, RNASeq data performed on Saudi fresh CRC samples showed that SSP1 mRNA expression was 4 times overexpressed in cancer samples compared with normal colorectal mucosa (Unpublished data). These findings may have significant clinical impact since CRC patients with low SPP1 cytoplasmic expression patterns require special clinical attention in terms of follow-up, management, and treatment. In clinical context, for example, stage II CRC patients with low SPP1 cytoplasmic expression who have undergone surgical resection could be advised to be subjected for adjuvant therapy with frequent follow-ups.
Strikingly, our results are in contrast with most of the previous studies that reported SPP1 overexpression in CRC to be associated with shorter survival and more aggressive phenotypes.14,26–29
Unfortunately, most of these studies did not consider the SPP1 intracellular localization (cytoplasmic vs. nuclear), which might bias their findings. Our results showed different SPP1 immunostaining patterns. In normal mucosa, the SPP1 expression is mainly apicolateral, whereas it was mainly apical with weak nuclear expression (Figure 1(a) and (b)). On the other hand, cancer and metastatic tissues showed diffused immunostaining at both cytoplasmic and nuclear levels (Figure 1(c) and (d); Table 3). This differential gradient of expression and localization is expected to affect SPP1 molecular functions. In fact, the protein localization of a biomarker (e.g. Beta-Catenin) was shown to impact its prognostic value. 30 Other studies have also reported bad prognosis results with higher SPP1 serum levels in CRC patients. 31 The results obtained in our study may partly be attributed to the molecular pathophysiology of CRC in Saudi Arabia (and the Arabic Peninsula in general), which arises as a consequence of a specific genomic background. These specific genomic mutations observed in Saudi CRC patients combined with particular environmental factors lead to a distinctive molecular roots of tumorigenesis. 32 These molecular signatures can manifest either at the genomic, transcriptomic, epigenomic, posttranslational, and/or the signaling pathways underlying the molecular onset and progression of CRC. This assumption is supported by a previous study published by our group where we investigated mutational status of 2800 COSMIC (catalog of somatic mutations in cancer) mutations in 50 oncogenes and tumor suppressor genes in our CRC cohort using NGS (next-generation sequencing). Results showed a particular genomic signature that was remarkably different from COSMIC patterns. In fact Saudi CRC tissues harbor both common and unique repeated mutations in genes such as TP53, APC, KRAS, PIK3CA, PTEN, EGFR, SMAD4, and FBXW7 with different frequencies compared with those reported in COSMIC (v70; Aug 2014). Significantly, higher frequencies of mutations in TP53, EGFR, and PIK3CA were reported while APC mutations were lower. 33 This genomic instability (mutation, amplification, or deletion) is expected to have substantial consequences in terms of the molecular events and signaling pathways driving the onset and progression of CRC. 22 In fact, the lower frequencies of APC mutations with different mutational sites (compared to COSMIC catalog) have been previously reported to be necessary for decreased SPP1 expression. 17
In addition, our group reported a lower CD44 expression levels in 70% of our same Saudi CRC cohort. 34 It is established that SPP1 functions through binding to its receptors CD44 and integrins in order to stimulate several CRC-promoting-kinase-based pathways (ERK, JNK1, and PI3K/Akt).19,35,36 Therefore, despite SPP1 overexpression, the lack of sufficient CD44 expression may hamper its pro-oncogenic downstream intracellular signal transduction. Thus, it may be speculated that SPP1 overexpression together with CD44 downregulation leads to less aggressive CRC tumors with lower clonogenicity and reduced tumor progression. Given the complexity of SPP1 expression and functions (SPP1 involved in tumorigenesis, calcium deposit, inflammation and immunity), other intricate molecular pathways of SPP1 may also be involved. In fact, key player genes shown to be mutated in our cohort studies and reported to interact with both SPP1 upstream and downstream pathways (e.g. EGFR, APC, TP53, PIK3CA, and SMAD4)37–39 may have contributed to this particular prognosis outcome.
This broad spectrum of SPP1 functions can be attributed to its extensive distribution in body fluids and tissues under different splicing isoforms (SPP1a, b and c), 40 intracellular localization and/or posttranslational modifications (phosphorylation and glycosylation). 41 Therefore, it is important to understand the localization and the diverse functions of various SPP1 isoforms within the tumor microenvironment and association of SPP1 gene (SPP1) with cancer-related genes in order to gain insights on molecules that mediate multiple functions of SPP1 13 (Figure 5). In addition, SPP1 genetic polymorphism has also been shown to affect its expression, secretion, and function within the tumor microenvironment.42,43 In fact, SPP1 isoforms mainly SPP1c was associated with worse survival outcomes.44–47 While the -156G>GG polymorphism of spp1 gene is associated with high cancer risk, the presence of -66T>G SNP may act as a protective factor for human cancers; whereas -443T>C mutation in spp1 promoter is not associated with cancer risk. 46 In case of CRC, mutations in spp1 promoter (rs9138 and rs1126616) were shown to be significant contributors to increased risk of developing CRC.42,44 Similarly, the presence of spp1 promoter SNPs -443 (rs11730582) and -1748 (rs2728127) was associated with the aggressiveness of breast cancer. 48

Overview of the complexity of SPP1 expression regulation and its downstream molecular functions in cancer.
Taken together, several SPP1 molecular subtypes with different structures, intracellular localization and functions are, therefore, released according to each specific tissue and/or pathophysiological context as summarized in Figure 5. 49 Such SPP1 expression and molecular functions in tumor cells and various stromal cells can act to promote tumorigenesis or suppress progression of the disease depending upon cell types and tumor microenvironment. 13 Therefore, a more individualized approach for CRC studies and particularly SPP1 prognosis outcomes’ assessment is highly recommended toward precision oncology.32,50
Furthermore, different techniques have been used so far to assess SPP1 expression levels in cancer patients along with diverse cut-offs and interpretation approaches. This context made the assessment of SPP1 as potential prognostic biomarker more challenging. For instance, the commercially available antibodies for immunohistochemistry (IHC) are general and unfortunately not SPP1 isoform-specific. Therefore, only the total SPP1 protein expression could be assessed although each isoform may have its specific localization, level of expression, and molecular function. Similar to IHC, the SPP1 expression level cut-offs is another variability contributing factor because several studies using same detection method (RT-PCR) have reported SPP1 as either suitable or unsuitable biomarker for prognosis of CRC patients.51,52 Therefore, and regardless of the used technology, additional efforts are required to enhance the technology resolution (depth), specificity, and standardization so the studies from different populations worldwide could be compiled and compared to gain better understanding of the molecular pathways of SPP1 and cancer in general.
Finally, all these interconnected factors discussed here might explain the discrepancies observed in association of SPP1 expression and prognosis outcome in our patients’ cohort. However, the small size of our cohort may be a limitation of this study and, therefore, should be expanded to confirm these findings. Moreover, the use of integrative technological approaches and cross-platforms validation is required to draw meaningful conclusions. The presence of isoforms, genetic polymorphisms, genomic instability, epigenomic variations, and posttranslational modifications (protein structure and relevant receptors) should be carefully addressed in a comprehensive way to extract personalized and tangible clinically relevant outcomes toward individualized oncology.53,54 Therefore, for considering SPP1 as prognostic biomarker and therapeutic target in cancer, its diverse functions, multiple isoforms, and genetic polymorphism should be taken into account. For example, an isoform-specific antibody is required for IHC assessment of SPP1 protein localization and expression.
It is to note that the more the target biomarker has multifunctions in several tissues, the more variability and inconsistencies according to the disease, tissue type, population genomic makeup, environment, and lifestyle are expected. These discrepancies are reinforced by the profound lack of our understanding of the intricate factors and complex molecular mechanisms involved in initiation, progression, and metastasis. These large-scale, multidisciplinary and cross-platforms studies are crucial to speed up our transition toward precision oncology.
Footnotes
Author contributions
M.A. and A.B. contributed in study design, statistical and data analysis, and manuscript drafting; W.G. contributed in TMA design and construction, immunostaining, statistical and data analysis, and manuscript revision; M.H. contributed in immunostaining; M.A.Q., M.A.J., M.A.A., and P.P. contributed in data interpretation and manuscript drafting, technical and administrative support; A.A.H. contributed in clinical data collection and statistical analysis; J.M. in study design and supervision of the whole team and contributed in TMA design. All authors critically reviewed and agreed on the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the National Plan for Science, Technology and Innovation (MAARIFAH)—King Abdulaziz City for Science and Technology—the Kingdom of Saudi Arabia—award number (11-BIO1524-03). The authors also acknowledge Science and Technology Unit, King Abdulaziz University for technical support.