
Abstract
Prostate cancer presents itself in a heterogeneous way with both aggressive and indolent forms. Despite the controversy surrounding its use, prostate-specific antigen screening ultimately leads to a greater number of diagnosed patients. One of the biggest challenges in clinical practice is to select the right patients for biopsy and, among diagnosed patients, to differentiate tumors with an indolent course from those with an unfavorable prognosis, in order to determine the best therapeutic decision for each case, avoiding unnecessary interventions. Currently, several types of biomarkers are available for clinical use in patients with prostate cancer, which include blood-based (prostate-specific antigen, Prostate Health Index®, 4K score®); urine sample-based (PCA3, SelectMDx®, ExoDx Prostate IntelliScore®); and biopsy, transurethral resection, or radical prostatectomy tissue-based (ConfirmMDx®, Oncotype®, Prolaris®, Decipher®). The aim of this review is to provide an overview of the current state of evidence and to highlight recent advances in the evaluation and diagnosis of prostate cancer, with emphasis on biomarkers related to diagnosis and to prognostic evaluation of localized prostate cancer.
Keywords
Introduction
Prostate cancer (PCa), excluding non-melanoma skin tumors, is the most prevalent cancer among men.1–3 Despite the US Preventive Services Task Force’s recent recommendation to restrict through serous dosage of prostate-specific antigen (PSA) screening for only selected populations, 4 many institutions still use it indiscriminately in all men over the age of 50.1,3 Patients with high PSA levels and/or with suspicious findings upon digital rectal examination (DRE) undergo prostate biopsy guided by transrectal ultrasonography with or without magnetic resonance imaging (MRI) for diagnostic confirmation.1,5 Prostate biopsy itself carries with it several risks as an invasive procedure with potential adverse events including rectal bleeding, macroscopic hematuria, hematospermia, fever, infection, and urinary retention.1,5,6
In the current environment of increased PSA screening, urologists still face a well-stablished dilemma: a greater number of patients receiving unnecessary treatments.3,7,8 That is because a large proportion of diagnosed tumors are considered low risk and thus clinically insignificant, with no signs of metastatic dissemination and with no survival benefit when radically treated.3,5,7,8 Indeed, one of the biggest challenges in urologic clinical practice is to screen only those patients whose overall survival would benefit from biopsy, and, among further diagnosed patients, to differentiate tumors with an indolent course from those with an unfavorable prognosis, in order to determine the best therapeutic decision for each case, avoiding surgery or radiotherapy for those cancers that will not progress further.2,8
PCa has a very heterogeneous behavior and, despite Gleason’s pathological classification being well-established and with well-accepted prognostic value, it is perceived in clinical practice that some patients in the same ISUP (International Society of Urological Pathology) group have cancers with different aggressive potentials. This leads experts in the field to believe that the existence of molecular factors driving outcome cannot be identified with conventional histopathological analysis. 9 With the objective of refining diagnosis and prognostic evaluation of patients with PCa, there is more research in emerging biomarkers now more than ever before. In addition to novel protein and cell-free DNA-based markers still in initial evaluation,10,11 there are currently several commercially available tests for use in PCa patients that feature well-validated biomarkers. These biomarkers utilize different types of samples, such as blood, tissue (biopsy, transurethral resection, and radical prostatectomy obtained specimen), and urine.
The objective of this literature review is to gather published studies of the biomarkers validated for clinical use, and to analyze reports of their use in the diagnostic and prognostic evaluation of localized PCa.
Methods
The present study is a literature review based on published articles subsequently indexed in the National Center for Biotechnology Information (NCBI) PubMed database. Articles of greater relevance were selected according to data citation and our authors’ assessment.
To determine which articles were to be included in this review, each one was critically assessed by two independent researchers (A.C. and P.P.K.). The researchers independently extracted data, using tables created for this purpose. The following data were obtained: author, year, journal, biomarker, clinical use (diagnosis or prognosis), sensitivity, specificity, and method accuracy.
Biomolecular markers in localized PCa
A biomarker is defined as any substance, molecule, or reaction that can be measured in the organism or in its products and that is able to influence or to predict the incidence of a specific consequence or disease.8,12 Several such categories include susceptibility, diagnostic, and prognostic markers.7,8 These biomarkers are mostly based on protein expression, mRNA expression, or detection of altered alleles at the DNA level, and these can be measured or evaluated in variety of sample types amenable to urologic practice, such as tissue, blood, and urine.7,8,13
In localized PCa, biomarkers are being increasingly studied and used, especially in four specific scenarios: (1) screening, (2) diagnosis and risk stratification, (3) decision between definitive treatment or active surveillance, and (4) evaluation of the necessity of adjuvant treatment. The development and the validation of a biomarker are complex procedures and normally demand technology, time, and a great number of patients for adequate statistical power in discovery and validation cohorts.
To obtain an adequate level of evidence (at least IB, see Table 1 in section “PCA3”) and to validate for clinical use, four requirements have to be met: (1) sufficient quantity of sample type (serum, urine, or tissue) and sufficient number of studied participants in prospective studies (primarily randomized), so the studied population can be representative and have statistical power; (2) the test has to be analytically and pre-analytically validated for use with archived specimens to guarantee its reproducibility (e.g. better anticoagulant or reagent to preserve the sample, storage time, and temperature); (3) the planning of the marker’s evaluation must be completely specific, done before the beginning of the study in archived specimens and must focus in the evaluation of only one test based on the marker; and (4) the results originated from the archival specimen analysis have to be validated in other populations in different studies. 14
Test descriptions.
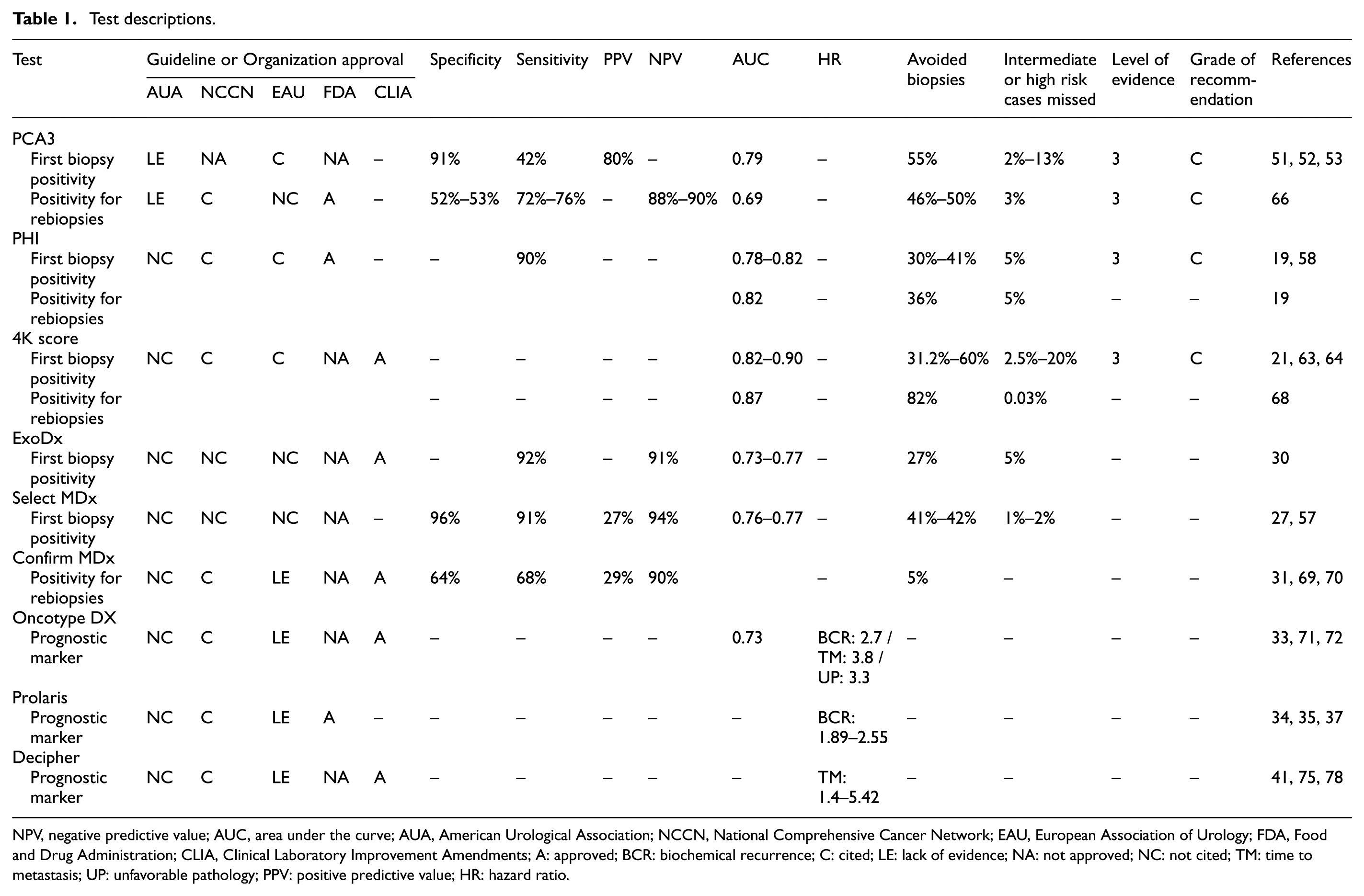
NPV, negative predictive value; AUC, area under the curve; AUA, American Urological Association; NCCN, National Comprehensive Cancer Network; EAU, European Association of Urology; FDA, Food and Drug Administration; CLIA, Clinical Laboratory Improvement Amendments; A: approved; BCR: biochemical recurrence; C: cited; LE: lack of evidence; NA: not approved; NC: not cited; TM: time to metastasis; UP: unfavorable pathology; PPV: positive predictive value; HR: hazard ratio.
Serum markers
PSA
PSA has been used since the 1980s when Stamey et al. 15 published an article showing higher sensitivity and relationship with tumor volume and aggressiveness, when compared to prostatic acid phosphatase. Since then, PSA has had an important role in detecting, staging, and monitoring of men with PCa, which led to a significant increase in early diagnosis. Because PSA is organ specific, it may be altered due to other diseases of the prostate gland that are not cancer, such as benign prostatic hyperplasia (BPH) and prostatitis. The increase in PSA serum level occurs because of greater production of PSA driven by the KLK3 (kallikrein related peptidase 3, ID354, 19q13.33) gene, which in turn is dependent upon the function of testosterone-bound androgen receptor (AR). 15
The distinction between increases in PSA caused by benign or malignant pathology is difficult. Therefore, PSA analysis refinement strategies have been applied to reduce this bias by correcting for orthogonal factors specifically affected or unaffected by tumorigenesis (such as PSA density, PSA growth rate, PSA according to age, free to total PSA ratio). 16 PSA dynamic analysis is also important, because fluctuations in its values can occur physiologically, although some studies have shown that rapid and progressive PSA rise are generally related to PCa. 17 In general, PSA produced by neoplastic cells is not subjected to intracellular proteolytic cleavage, which results in a higher fraction of PSA-ACT (alpha 1-antichymotrypsin) and a lower percentage of free-PSA, thus being a key measurement. 18 Details of the results regarding PSA analysis refinement strategies, which are already widely studied, are not going to be scrutinized in this article.
Prostate Health Index (PHI)
Free-PSA is composed of three molecular forms (proPSA, benign PSA, and intact PSA) that exist in equal serum concentrations. The precursor form of PSA (proPSA) contains a peptide of seven amino acids that, when cleaved by Hk2 (Human Kallikrein 2), results in the active form of PSA. However, the partial cleavage of this peptide can lead to inactive forms of PSA ([–2]proPSA, [–4]proPSA and [–5]proPSA), all of which are expressed in the prostate’s peripheral zone. The [–2]proPSA form is elevated in PCa, being an important independent predictor of the disease in biopsy. 19 The Beckman Coulter® PHI is a Food and Drug Administration (FDA) approved test, which combines in one mathematical formula the values of total PSA, free-PSA, and [–2]proPSA. Studies have showed that PHI was related to increased accuracy in the detection of PCa for high risk disease in comparison to total PSA or to free-PSA percentage in patients with PSA between 4 and 10 ng/mL and with normal DRE. 20
4K score
The 4K score is a panel composed of 4 kallikreins (4K), which combines total PSA, free-PSA, intact PSA, and Hk2. It was developed in laboratory by OPKO® (Miami, Florida, USA) and is used along with clinical data (age, DRE findings, and biopsy results). Studies have shown that this test not only improves the accuracy in predicting the chances of a clinically significant disease but also the selection of candidates for biopsy. 21
Urinary markers
PCA3
PCA3 is a long noncoding RNA that is not expressed outside of the prostate and that has higher levels detected in neoplastic tissues in comparison to benign tissues. Its biological function is not well-established. 22 The Progensa PCA3 assay® (Gen-Probe, San Diego, California, USA) measures the concentration of the PCA3 gene and the concentration of PSA gene (KLK3) RNA molecules in the urine through an algorithm that calculates the “PCA3 score.” To increase the test’s detection sensitivity, urine is collected after prostate massage, sweeping laterally to medially toward the median sulcus each prostate lobe three times. One hour after the prostate massage, the first 20–30 mL of urine is collected. The test helps to detect PCa, especially in those patients with a previously negative biopsy. However, its relationship with tumor aggressiveness and with prognostic value is still controversial.23–25
SelectMDx®
SelectMDx® (MDxHealth, Irvine, California, USA) is a reverse transcription followed by polymerase chain reaction (RT-PCR) test that measures the level of messenger RNA of the DLX1 (distal-less homeobox 1, ID1745, 2q31.1) and HOXC6 (homeobox C6, ID3223, 12q13.13) genes and that uses KLK3 expression as internal reference. The protein coded by the DLX1 gene is located in the cell nucleus, where it can act as a transcriptional regulator of signals from multiple members of the TGFβ superfamily. 26 The HOXC6 gene encodes a transcription factor, which can have an important role in tissue morphogenesis. 26 The KLK3 gene is one of the 15 members of the kallikrein subfamily, located in a cluster on chromosome 19.
Increasing evidence suggests that kallikrein expression is related to carcinogenesis and some kallikreins, the potential of being a tumor or other disease marker. KLK3’s coded protein PSA functions as an active protease in seminal plasma. 26 The increase in DLX1 and HOXC6 expression is associated to a rise in the probability of PCa with Gleason greater or equal to 727 and studies of cost-effectiveness are being performed to evaluate the use of SelectMDx in clinical practice. 28
ExoDx Prostate IntelliScore®
The ExoDx Prostate IntelliScore® (Exosome Diagnostics, Waltham, MA, USA) is a urine test that does not require previous DRE. It evaluates the gene expression derived from urine-based exosomes containing PCA3 mRNA from ERG mRNA that originated from the fusion between the AR-regulated TMPRSS2 (transmembrane protease serine 2) gene and the ERG (ETS transcription factor, ID2078, 21q22.2) oncogene. 29 Exosomes are cell-free membrane-bound vesicles that are present in nearly every bodily fluid, including urine. The ERG gene codes transcription factors of the ETS (erythroblast transformation-specific) family that are key regulators of embryonic development, cell proliferation, cell differentiation, angiogenesis, inflammation, and apoptosis. 26 This test increases the detection of patients with clinically significant diseases among men with a rise in PSA and could reduce the number of unnecessary biopsies. 30
Genetic tissue markers
ConfirmMDx®
The ConfirmMDx® test (MDxHealth, Irvine, California, USA) is a DNA hypermethylation test of three markers (GSPT1, APC, and RASSF1) performed in tissue derived from formalin-fixed, paraffin-embedded prostate biopsy with negative result for PCa. It evaluates epigenetic alterations of DNA from cells that could be nearby cancer cells that were missed on biopsy, but would be influenced by unsampled tumor. This exam was developed to help identify patients that would need a new biopsy and that potentially benefit from radical treatment. 31
The GSPT1 (G1 to S phase transition 1, ID2935, 16p13.13) gene is responsible for the G1 to S phase transition in the cell cycle. The APC (APC, WNT signaling pathway regulator, ID324, 5q22.2) gene codes a tumor suppressor protein that acts as a Wnt signaling pathway antagonist. It is also involved in other functions, such as cell migration and adhesion, transcription activation, and apoptosis. The RASSF1 (Ras association domain family member 1, ID11186, 3p21.31) gene codes a protein that is similar to the RAS proteins. The loss or alteration of these genes’ expression, which is often influenced by hypermethylation of the genes’ promoters, has been associated with tumor pathogenesis. 26
Oncotype DX for Prostate Cancer®
The Oncotype DX® (Genomic Health Inc, Redwood City, California, USA) is a GPS (Genomic Prostate Score) composed of five reference genes and of 12 neoplastic related genes that represent different mechanisms of tumor origin: androgen response (AZGP1 (alpha-2-glycoprotein 1, zinc-binding, ID563, 7q22.1); KLK2 (kallikrein related peptidase 2, ID3817, 19q13.33); SRD5A2 (steroid 5 alpha-reductase 2, ID6716, 2p23.1), and FAM13C (family with sequence similarity 13 member C, ID220965, 10q21.1)); cell organization (FLNC (filamin C, ID2318, 7q32.1); GSN (gelsolin, ID2934, 9q33.2); TPM2 (tropomyosin 2, ID7169, 9p13.3), and GSTM2 (glutathione S-transferase mu 2, ID2946, 1p13.3)), proliferation (TPX2 (TPX2, microtubule nucleation fator, ID22974, 20q11.21)) and stromal response (BGN (biglycan, ID633, Xq28), COL1A1 (collagen type I alpha 1 chain, ID1277, 17q21.33), and SFRP4 (secreted frizzled related protein 4, ID6424, 7p14.1)). 32
It was specifically developed to be performed in biopsy specimens of patients diagnosed with low risk (ISUP 1 and 2) PCa to help decide the course of treatment. 33 Studies showed that an elevated GPS correlates with unfavorable pathology in prostatectomy and biochemical recurrence (BCR) in 5 years. 33
Prolaris®
Prolaris® (Myriad Genetics, Inc., Salt Lake City, UT, USA) is performed on RNA extracted from tissue of prostatic biopsies or prostatectomies. It evaluates 31 cell cycle progression (CCP) genes: CDKN3, RRM2, RAD54L, RAD51, CDC20, CDC2, BUB1B, PLK1, TOP2A, PTTG1, FOXM1, KIF11, KIAA0101, NUSAP1, CENPF, ASPM, DLGAP5, BIRC5, KIF20A, TK1, PBK, ASF1B, C18orf24, CDCA3, MCM10, PRC1, DTL, CEP55, CENPM, CDCA8, and ORC6L.
It was developed and validated to offer prognostic information in patients with PCa of all risk groups. In undiagnosed or untreated patients, studies showed that it could be useful in the prediction of prostate cancer–specific mortality within 10 years. Among patients subjected to surgery, it has a further a role in predicting the risk of BCR (in 10 years) and of metastasis.34–38
Decipher®
The Decipher® test (GenomeDx Biosciences Inc., Vancouver, BC, Canada) is an assay that can be performed using RNA from biopsy or radical prostatectomy specimen that are evaluated on an Affymetrix Human Exon microarray. Probe-level expression data from 22 genes are used to compute a Decipher score. 39 These are genes related to CCP (NUSAP1, ZWILCH, UBE2C, CAMK2N1, RABGAP1), cell proliferation and differentiation (LASP1, IQGAP3, NFIB, S1PR4), cell adhesion and motility (THBS2, ANO7, PCDH7, MYBPC1, EPPK1), immune system evasion functions (TSBP, PBX1), and unknown functions (PCAT-32, GLYATL1P4/PCAT-80, TNFRSF19).
Decipher was developed to predict the risk of metastasis development in 5 years in patients with PCa after prostatectomy for assessing the timing of hormone therapy or radiation therapy. 40 Recent studies have also showed its role in the selection of patients that are candidates for active surveillance. 41
Applications of biomolecular markers in clinical practice
Imaging studies and biomolecular markers’ role in PCa diagnosis
Multiparametric magnetic resonance imaging (mpMRI) and CT-guided biopsy with MRI fusion have been increasingly more utilized among patients that have a previously negative biopsy and even among patients that are biopsy naive. Recent meta-analysis showed that the median negative predictive value (NPV) for any type of PCa is approximately 82.4% and 88.1% for clinically significant neoplasia. 42 However, there is still tremendous variability among many studies, which is due in part to PCa prevalence in each studied population, with greater PCa prevalence populations having greater NPV. 42
Furthermore, the test specificity is moderate, with a substantial number of false-positives in patients with PI-RADS (Prostate imaging reporting and data system) 3 and 4. The positivity rate in these cases, with fusion biopsy, is approximately 15.8% and 29.8%, respectively. 43 Even though the studies are being conducted in big centers, with a large number of cases in which mpMRI are done, mpMRI reproducibility analysis is still moderate due to variability among readers. 44
Given the caveats of mpMRI, the detection of biomarkers can still have an important role, especially in patients without mpMRI-visible lesions that are candidates for rebiopsy. Studies showed that this combination can increase NPV to around 91%, for example, among patients with PSA density lower or equal to 0.2 ng/mL. 45
Biomolecular markers related to first biopsy positivity
PCA3
Detection of PCA3 is neither validated nor cleared by the FDA in this scenario. The European Association of Urology (EAU) recommendation, with a level of evidence “3” and a grade of recommendation “C,” 46 is to offer a risk evaluation using this marker in asymptomatic patients with PSA between 2 and 10 ng/mL, before doing a biopsy. The American Urological Association (AUA) recognizes that this test can be used as an adjunct to help decide the need for biopsy, but emphasizes the lack of evidence concerning the increase in benefits provided by this test. 47 The NCCN (National Comprehensive Cancer Network) guidelines state that this test is not appropriate in this clinical scenario. 46
Some studies have showed the test’s value in the first biopsy scenario.48–50 Wei et al. evaluated the PCA3 test value in both the occasion of initial biopsy and of rebiopsy. It revealed a positive predictive value (PPV) of 80% for PCA3 scores over 60, a sensitivity of 42%, and a specificity of 91%. The rise in PCA3 was correlated with a greater probability of PCa, independent of PSA level. When the test was analyzed with the “Prostate Cancer Prevention Trial” (PCPT) risk calculator, 51 the use of PCA3 rose the AUC (area under the curve) from 0.68 (PCPT) to 0.79 (PCPT associated with PCA3). With regard to high risk cancer, AUC rose from 0.74 to 0.78. This study showed that in this scenario among patients with PCA3 scores lower than 20, only 13% of patients with high risk PCa were not going to be diagnosed. 52
To evaluate the positivity rate in the first biopsy, PCA3 would be best indicated if associated with risk calculators.53–56 A study showed that if we considered a test value lower than 30 as the cutoff value, less than 2% of high risk neoplasia were not going to be diagnosed and 55% of biopsies could thus be avoided 53 (Table 1).
ExoDx Prostate IntelliScore®
The ExoDx Prostate IntelliScore® was validated in studies to be used in biopsy naïve patients, but it is still not approved by the FDA. This diagnostic method is neither cited nor recommended by current guidelines.
McKiernan et al. reported a validation study with 255 cases, in which ExoDx Prostate IntelliScore® was associated with current parameters used to evaluate the risk of unfavorable pathology (PSA, age, race, and family history). Inclusion of ExoDx Prostate IntelliScore presented an improvement in the AUC, going from 0.66 to 0.77. In an independent validation study with 519 patients, a gain in the AUC going from 0.63 to 0.73, was again shown when using ExoDx Prostate IntelliScore® associated with the current considered parameters. 30
ExoDx Prostate IntelliScore® has a sensitivity of 92% and a NPV of 91.3%. The test revealed that about 27% of biopsies could have been avoided and that only 5% of patients with Gleason 7 or more would not have been diagnosed. 30 The initial biopsy scenario is ideal for its application, using a value of 15.6 points as a threshold to determine the performance of a biopsy or not. 30
SelectMDx®
SelectMDx® is validated to be used before the first biopsy and is cleared by the CLIA (Clinical Laboratory Improvement Amendments). However, it is not yet approved by the FDA and is neither cited nor recommended by current guidelines (AUA and EAU).
Leyten et al. 57 performed a validation study which indicated improved accuracy for detecting high risk neoplasia, with AUC of 0.77, in comparison to PSA alone (AUC 0.72) and PCA3 (AUC 0.68). Van Neste et al. 27 published a study with 905 patients showing a sensitivity of 91%, a specificity of 36%, a NPV of 94%, a PPV of 27%, and an AUC of 0.76, thus demonstrating that its use leads to a 42% decrease in the total number of biopsies and that only 2% of high risk neoplasias would not be diagnosed. Dijkstra et al. 28 showed in a cost-effectiveness study that the use of SelectMDx® in the selection of patients to perform a biopsy led to a 41% decrease of unnecessary biopsies and that these patients only had a 1% chance of not being diagnosed with high risk PCa. In addition, it led to a cost reduction of $128 (USD) per patient.
PHI
PHI is validated to be used before the first biopsy and is cleared by the FDA for patients over 50 years of age, PSA between 4 and 10 ng/mL, and DRE not suggestive of neoplasia. The European Association of Urology (EAU) recommendation, with a level of evidence “3” and a grade of recommendation “C,” 44 is to offer a risk evaluation using this marker in asymptomatic patients with PSA between 2 and 10 ng/mL, before doing a biopsy. The NCCN guidelines instruct that consideration of this marker could increase biopsy specificity in patients with PSA over 3 ng/mL. 46
In a multi-center case-control clinical study, Catalona et al. reported on 892 patients without a PCa history, with a normal DRE and a PSA between 2 and 10 ng/mL. By including PHI, the authors showed better accuracy in PCa detection and in ISUP 3 diagnosis with AUC of 0.78 and 0.82 in comparison to the use of free and total PSA. A cutoff value of 25 points could have avoided between 36% and 41% of unnecessary biopsies and between 17% and 24% of overdiagnosis, while only 5% of PCa with Gleason 7 or greater would not be diagnosed. 19
Loeb et al. 58 showed in a study of 658 patients with PSA between 4 and 19 ng/mL that, with a sensitivity of 90% and PHI score lower than 28.6 points, 30.1% of biopsies could have been avoided compared to 21.7% if only the value of free-PSA was used. Increases in PHI values predict higher risk of clinically significant disease on biopsy and also worse prognosis upon prostatectomy. 59 When compared to other available tests, studies showed higher detection rate of clinically significant diseases when using PHI in comparison to PCA3.60,61
4K score
The 4K score is validated in the pre-first biopsy scenario and is cleared by CLIA, but it is not approved by the FDA. The EAU recommendation, with a level of evidence “3” and a grade of recommendation “C,” 62 is to offer a risk evaluation using this marker in asymptomatic patients with PSA between 2 and 10 ng/mL, before doing a biopsy. The NCCN guidelines instruct that considerations can be done about this marker in order to increase biopsy specificity in patients with PSA higher than 3 ng/mL. 46
Vickers et al. in a cohort of 2186 patients, showed that, when using the 4K score, there is a better accuracy to detect PCa with a rise in the AUC to detect high risk neoplasia from 0.87 to 0.90. His study concludes that the test presents a 60% reduction in the number of biopsies among men with a PSA increase, not diagnosing only a small number of patients (31 out of 152 patients) with low risk PCa and only 1 out of 40 patients with high risk PCa. 63
Parekh et al. 21 in a cohort of 1012 patients showed an improvement in the accuracy to detect clinically significant PCa with an AUC of 0.82, given that a cutoff value greater or equal to 9% avoids 31.2% of biopsies. Nordstrom et al. 64 showed that a 4K score could avoid 44% of biopsies when a high grade PCa risk value of 15% is accepted, with a risk of not diagnosing approximately 20% of high grade tumors.
Markers related to positivity in rebiopsies
PCA3
The PCA3 test is validated to be used in patients who are candidates for a rebiopsy and is cleared by the FDA. The EAU recommends the test with a level of evidence “3” and a grade of recommendation “C” 46 and reinforces that the role of the exam is still uncertain and probably not cost-effective. 65 The AUA recognizes that this test can be used as an adjunct to help decide the need for biopsy, but emphasizes the lack of evidence concerning the increase in benefits provided by this test. 47 The NCCN guidelines instruct that considerations can be done about this marker in order to increase biopsy specificity in the scenario of rebiopsy. PCA3 values lower than 25 points indicate low risk for PCa and are used to not indicate rebiopsy. 46
Luo et al. 66 in a meta-analysis with 11 clinical trials reported a sensitivity of 72% and a specificity of 53% related to the use of PCA3 with a cutoff value of 20 points. The study showed a NPV of up to 90% in various populations, suggesting its potential use in PCa exclusion. A decrease in unnecessary biopsy was also observed in more than 50% of the cases. These findings were also observed in multicentric prospective studies in Italian and American cohorts.52,67
PHI
As discussed above in section “PHI” under “Imaging studies and biomolecular markers’ role in PCa diagnosis,” PHI was initially studied in the context of patients without previous biopsies and of patients with a previously negative biopsy. However, its FDA approval is only for patients without a previous biopsy. Catalona et al. showed better accuracy for PCa detection and for ISUP 3 with an AUC of 0.82, in comparison to the use of free and total PSA (AUC of 0.78). A cutoff value of 25 points could avoid between 36% and 41% of unnecessary biopsies and between 17% and 24% of overdiagnosis, while not diagnosing only 5% of PCa with ISUP 2 or higher. 19
4K score
Gupta et al. showed an increase in diagnostic accuracy of tumors with Gleason 7 or higher when 4K score was associated with currently utilized models, which include age, DRE, and total PSA. The AUC for high grade neoplasia detection rose from 0.76 to 0.87. It was concluded that the test reduces the number of biopsies in 82% and does not diagnose only a small percentage of patients with low risk (64/1000 patients) and high risk (3/1000 patients) PCa. For each 272 men in whom we avoid the biopsy, only 1 high risk patient is lost. 68
ConfirmMDx®
ConfirmMDx® is validated in the rebiopsy scenario and is cleared by the CLIA, but it is not approved by the FDA. The EAU does not recommend it to be routinely used 62 given the small quantity of evidence in the literature. The test is not cited by the AUA guideline. The NCCN guidelines instruct that this test can be an option for men who consider repeating the biopsy, because it can identify individuals with higher risk of PCa diagnosis. 46
Stewart et al., in a retrospective study, evaluated 423 patients and showed a sensitivity of 68% and a specificity of 64%, but a NPV of 90% and a PPV of 29% when determining who would have PCa in a repeat biopsy. And when a multivariate analysis was done, alongside with age, total PSA, DRE, and histopathological result of the first biopsy, the test was an important independent predictor of PCa risk detection in 30 months with a chance of risk of 3.17. 31
Partin et al., 69 in a multicentric study with 350 patients showed a NPV of 88%, with the test being an important independent predictor of PCa risk detection, with a chance of risk of 2.69. Wojno et al., 70 also in a multi-center study, reported an approximate 5% reduction in the rebiopsy rate, considering a cohort of 138 patients with a previously negative biopsy.
Prognosis biomolecular markers
Oncotype DX
Oncotype DX for Prostate Cancer predicts the probability of an unfavorable pathology in prostatectomy. It is cleared by CLIA, but it is not approved by the FDA. The NCCN guidelines state that patients with very low risk and low risk localized tumors can consider using the test, but studies to compare effectiveness are still necessary to prove clinical utility and improve risk stratification. 46 The EAU does not recommend it to be routinely used. 62
In a study with 395 patients with ISUP 1 (76%) and 2 (24%) in biopsy, Klein et al. 33 showed that the GPS was an unfavorable pathology predictor in the specimen and that, for each 20 points increase in the GPS, the risk rose 1.85 times. Cullen et al. 71 showed that Oncotype DX GPS, after adjusting for NCCN risk groups, was an independent predictor of BCR (hazard ratio [HR]: 2.7), time to metastasis (HR: 3.8) and unfavorable pathology (OR 3.3).
In a meta-analysis, Brand et al. showed that the benefit of using the Oncotype was higher than any independent risk classifier (CAPRA score or NCCN risk group) using a decision curve. The AUC to predict favorable pathology rose from 0.68 to 0.73 when Oncotype DX was used in combination with the NCCN risk scale. The proportion of patients with chance of favorable pathology of over 80% rose from 11% to 23% using the test associated with NCCN risk and achieved 31% using Oncotype DX associated with CAPRA risk. 72
Prolaris
Prolaris CCP is validated for prognostic evaluation and is cleared by the FDA to be used in men with low risk PCa according to the NCCN and in post-prostatectomy patients with a higher risk of recurrence. NCCN guidelines state that patients with very low and low risk localized tumors can consider using the test, but studies to compare effectiveness are necessary to prove clinical utility and improve risk stratification. 46 The EAU does not recommend it to be routinely used. 62
Cuzick et al., in a retrospective cohort of 366 American patients undergoing radical prostatectomy and of 337 British patients subjected to transurethral resection of prostate, showed that a 1 point increase in the Prolaris value in the American cohort led to an increase in BCR risk with HR of 1.89. In a multivariate analysis using the Prolaris test value, Gleason score, pathological stage, pathological grade, surgical margins, extra-capsular extension, seminal vesicle invasion, lymph node involvement, and age of surgery, each 1 point increase in the Prolaris value led to an increase in BCR risk with HR of 1.77. 37
Cuzick et al. also evaluated the role of Prolaris as a cancer mortality predictor in a retrospective study of 442 cases. The univariate analysis revealed that for each 1 point increase, the cancer mortality risk rose 2.02 times. That corresponded to a HR of 2.56, going from the first to the third quartile. In the multivariate analysis, the HR was 1.65 for each 1 point increase in the score. 35
Cooperberg et al. validated this test in prostatectomy specimens from 413 patients and concluded that Prolaris was a BCR predictor after prostatectomy in a univariate analysis with a HR of 2.1 for each 1 point increase in the test. Prolaris was also concluded to be an independent predictor of BCR in an adjusted multivariate analysis for CAPRA with a HR of 1.7. 34
In a study with 141 men who received only radiotherapy or radiotherapy combined with androgen deprivation, Freedland et al. showed that the use of Prolaris was associated with BCR with a HR of 2.55 by univariate analysis. In the multivariate analysis including PSA, Gleason score, hormone therapy, and positivity rate in the fragment, the significance of its use remained with a HR of 2.11. Furthermore, it was also independently related to cancer-specific mortality. 73
Crawford et al. reported the decision-making process in a study performed with providers. The decision to choose definitive treatment after analysis of results from Polaris, showed a shift toward treatment recommendation in ~65% of the cases, and a treatment “decrease” in ~40% of the cases (favoring active surveillance instead of definitive treatment). 74
Decipher
Decipher is validated in this scenario and is cleared by the CLIA, but it is not approved by the FDA. The NCCN guidelines state that the test can be considered to be used in patients with localized tumors, but studies to compare effectiveness are necessary to prove clinical utility and improve risk stratification. 46 The test is not cited by the EAU guidelines. 62
In a study to validate Decipher, in which the test was performed in biopsies from 57 out of 169 patients subsequently undergoing radical prostatectomy, Klein et al. 41 showed that for each 10% increase in the Decipher value, HR increased by 1.72 for metastasis risk in 10 years after prostatectomy when combined with NCCN’s risk stratification. Likewise, in a single center study that evaluated 100 patients who received both radiotherapy and hormone therapy for 6 months, in order to evaluate time to metastasis, Nguyen et al. showed that each 0.1 unit increase in the test score was associated with the time of metastasis onset in the univariate (HR 1.4) and multivariate (HR 1.36) analysis. The c-index for metastasis after 5 years was 0.63 for the NCCN risk scale and 0.76 for Decipher. The cumulative incidence for metastasis for a Decipher value over 0.6 reached 20% in 5 years after radiotherapy. 75
In a prostatectomy specimen analysis, Cooperberg et al. compared CAPRA and Decipher as cancer-specific mortality predictors in men with high risk of recurrence (PSA > 20 ng/mL, Gleason greater or equal to 8 or pT3b pathological stage) after radical prostatectomy. CAPRA and Decipher showed to be independent cancer-specific mortality predictors, with HR of 2.36 and of 11.26, respectively, with a cumulative incidence of death related to cancer in 10 years of 45%. The authors suggested that the Decipher can be used to better classify high risk patients who would benefit from a more aggressive adjuvant treatment, given that 60% of patients were reclassified as low risk. 40
Decipher was also validated as a predictor of metastasis in 5 years after prostatectomy by Karnes et al., in a cohort of 1010 patients. The results showed an increase in accuracy, with AUC of 0.79, which is greater than the current clinical models used. A multivariate analysis confirmed it to be an independent predictor of metastasis in 5 years after prostatectomy, with a cumulative incidence of 2.4% for patients with a low Decipher score (<0.4), and of 22.5% for a high score (>0.6). 76
Den et al. evaluated this marker’s utility to predict which patients would benefit from adjuvant RT or from salvage RT (only when a PSA increase occurs). In the cases with low Decipher score (<0.4), there was no difference between cumulative incidence of metastasis, but in the cases with high Decipher score (>0.6), the cumulative incidence of metastasis within 5 years was significantly lower in patients who received adjuvant RT when compared to those who received salvage RT (6% vs 23%). The authors suggest that patients with high Decipher score would benefit from adjuvant RT (with an 80% risk reduction), while those with low score could be treated with salvage RT, if necessary. 77 Likewise, Ross et al. evaluated the efficacy of post-operative radiation in a prostatectomy cohort of 422 men adjusted for CAPRA-S and Decipher score. This study revealed in multivariable analyses that salvage RT and no RT were associated with an increase of 4.31 and 5.42 in increased rate of metastasis, respectively, when compared with adjuvant RT or salvage RT in minimal residual disease (PSA 0.2–0.49 ng/ml). 78
Discussion and final considerations
Clinicopathological nomograms are widely used in risk stratification of patients with PCa and, even though useful in clinical practice, there is still limited accuracy. As we improve our knowledge of a PCa’s genetic signature and identification of biomolecular characteristics that can help us better understand tumor biology, we can significantly impact the clinical handling of men under investigation of PCa and best treatment indication for those already diagnosed.
The process of developing and validating a biomolecular marker is complex and requires, in general, large investments, significant number of patients, and an adequate follow-up time to analyze the outcome in question. One of the main limiting factors of many biomarker’s use is their cost, especially in underdeveloped countries.
Currently, in the primary guidelines governing urological practice, some markers are validated and recommended in certain situations (Table 1).
PHI and 4K score can be used as a tool to select patients who are candidates for biopsy with the objective of decreasing the frequency of unnecessary biopsies (PHI use would avoid 30%–41% and 4K score 31.2%–82%) and increasing the accuracy of clinically significant tumor detection (PHI use would miss 5% of intermediate or high risk cases in comparison with 0.03% to 20% if 4K score was used). ExoDx use would avoid 27% of unnecessary biopsies and would miss 5% of intermediate or high risk cases and SelectMDx 41% and 1%–2%, respectively. PCA3 (sensitivity of 76% and specificity of 91%) and ConfirmMDx (sensitivity of 68% and specificity of 64%) can be used to evaluate patients with PCa suspicion who had a previously negative biopsy, which in turn impacts the recommendation to rebiopsy.
Oncotype DX and Decipher, through biopsy specimen analysis, have a prognostic value and help determine treatment (conservative or radical). Decipher and Prolaris were developed for post-prostatectomy prognosis, informing on the decision and timing of adjuvant radiation therapy.
We can conclude that, even though it is promising, the routinely clinical use of PCa biomarkers still lacks strong evidence in order to be incorporated in the daily practice of the majority of urologists and oncologists. Our goal should be that with sufficient evidence, we can integrate it to our existing nomograms and to define the scenario in which each test will be most beneficial for decision-making.
Footnotes
Acknowledgements
Ariê Carneiro and Paulo Priante Kayano are joint first authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.