
Abstract
Lung cancer is a malignant tumor with high metastatic ability and bone is the most common site of distant metastasis of it. However, the independent risk factors for bone metastases of lung cancer remain largely to be elucidated. Here, we conducted a retrospective study to evaluate the correlation between clinical–pathological parameters, serum levels of neuron-specific enolase and CYFRA21-1, and bone metastases in lung cancer patients. The results revealed that patients with bone metastases were younger than those without metastases. Adenocarcinoma was the most frequent type of histopathology in patients with bone metastases. And the incidence of bone metastasis in patients with adenocarcinoma was significantly higher than those with other histopathological subtypes (p < 0.001). Furthermore, the serum concentration of neuron-specific enolase was significantly higher in patients with bone lesions than those without bone metastases. Multivariate logistic regression analysis showed that patients’ age (odds ratio = 1.024, p < 0.001), concentrations of neuron-specific enolase (odds ratio = 1.212, p = 0.004), and histopathological types (odds ratio = 0.995, p = 0.001) were the independent risk factors for bone metastases in patients with lung cancer. Thus, physicians should pay attention to these factors in order to identify bone metastasis earlier while patient was primarily diagnosed as having lung cancer.
Introduction
Lung cancer is one of the most common malignant tumors and the leading cause of human cancer deaths worldwide. It accounts for 20.6% of cancer mortality.1,2 Bone is the common site of distant metastasis in lung cancer. Bone metastases are often complicated with skeletal-related events (SREs) which lead to serious morbidity. 3 The SREs decrease the quality of patients’ life by affecting physical, functional, and emotional well-being. And they seem to represent a negative prognostic factor for patients with lung cancer.4,5 Therefore, early diagnosis of bone metastases is an important challenge to increase the survival rate in lung cancer. Several tumor biomarkers contributing to bone metastases of lung cancer were evaluated by basic research.6–8 However, clinical biomarkers dedicated to bone metastases in lung cancer remain unclear.
Recently, several serum tumor markers, including neuron-specific enolase (NSE) 9 and cytokeratin-19 fragments (CYFRA21-1), 10 have been extensively investigated and considered to be potentially predictive and prognostic factors for non-small-cell lung cancer. However, little is known about the correlation between the serum levels of the tumor markers and bone metastases in patients with lung cancer.
In this retrospective study, we investigated the correlation between clinical–pathological parameters, biomarkers, and bone metastases in lung cancer at the time of diagnosis to identify the potential independent risk factors for bone metastases.
Materials and methods
This study was approved by the ethics committee of the hospital. After that, a retrospective study was carried out and a series of consecutive patients who were diagnosed as lung cancer by histopathology between January 2005 and October 2016 were included. Patients’ demographics, radiological data, and serum concentrations of CYFRA21-1 and NSE were reviewed. Bone metastasis was diagnosed by computed tomography (CT) scan and/or magnetic resonance imaging (MRI). If necessary, radionuclide bone scan will be performed to confirm the diagnosis. The serum levels of CYFRA21-1 and NSE were measured in serum obtained from peripheral venous blood by radioimmunoassay. According to the instruction of the laboratory, 3.3 ng/mL was considered to be the upper normal limit for CYFRA21-1 and 16.3 ng/mL for NSE. The correlation between clinical parameters and bone metastases was analyzed, and the risk factors for bone metastases in lung cancer were identified.
Statistical analysis
Univariate analysis was used to identify the potential factors associated to bone metastases in patients with lung cancer. The gender and histopathological types in patients with and without bone metastases were analyzed byChi-square test. Independent sample t-test was performed to evaluate the differences in concentrations of NSEand CYFRA21-1 between patients with and withoutbone lesions. The independent risk factors related tobone metastases were analyzed by multivariate logistic regression analysis model. Statistical analysis was conducted by SPSS 19.0 software (Chicago, IL, USA). A p value less than 0.05 was considered to be statistically significant.
Results
Demographic characteristics
A total of 1115 patients with lung cancer were included in this study. The demographic data of them are displayed in Table 1. Of these patients, 264 (23.7%) were found with bone metastases at the time of diagnosis. The distribution of bone metastases was demonstrated in Table 2.
Characteristics of patients with lung cancer.

The distribution of bone metastases in patients with lung cancer.

The clinical–pathological parameters in patients with and without bone metastases
In order to investigate the differences between patients with and without bone metastases on clinical-pathological parameters, chi-square test was performed. The results showed that patients with bone metastases were significant younger than those without metastases (p = 0.006). Additionally, statistically significant difference was found between patients with and without bone metastases on histopathological types (p < 0.001) (Table 3). And patients with adenocarcinoma had the highest incidence (158 cases, 59.8%) of bone metastases among the histopathological subtypes. No significant difference was found on gender between patients in the two groups (p = 0.551).
Univariate analysis for the potential factors related to bone metastases in lung cancer patients.
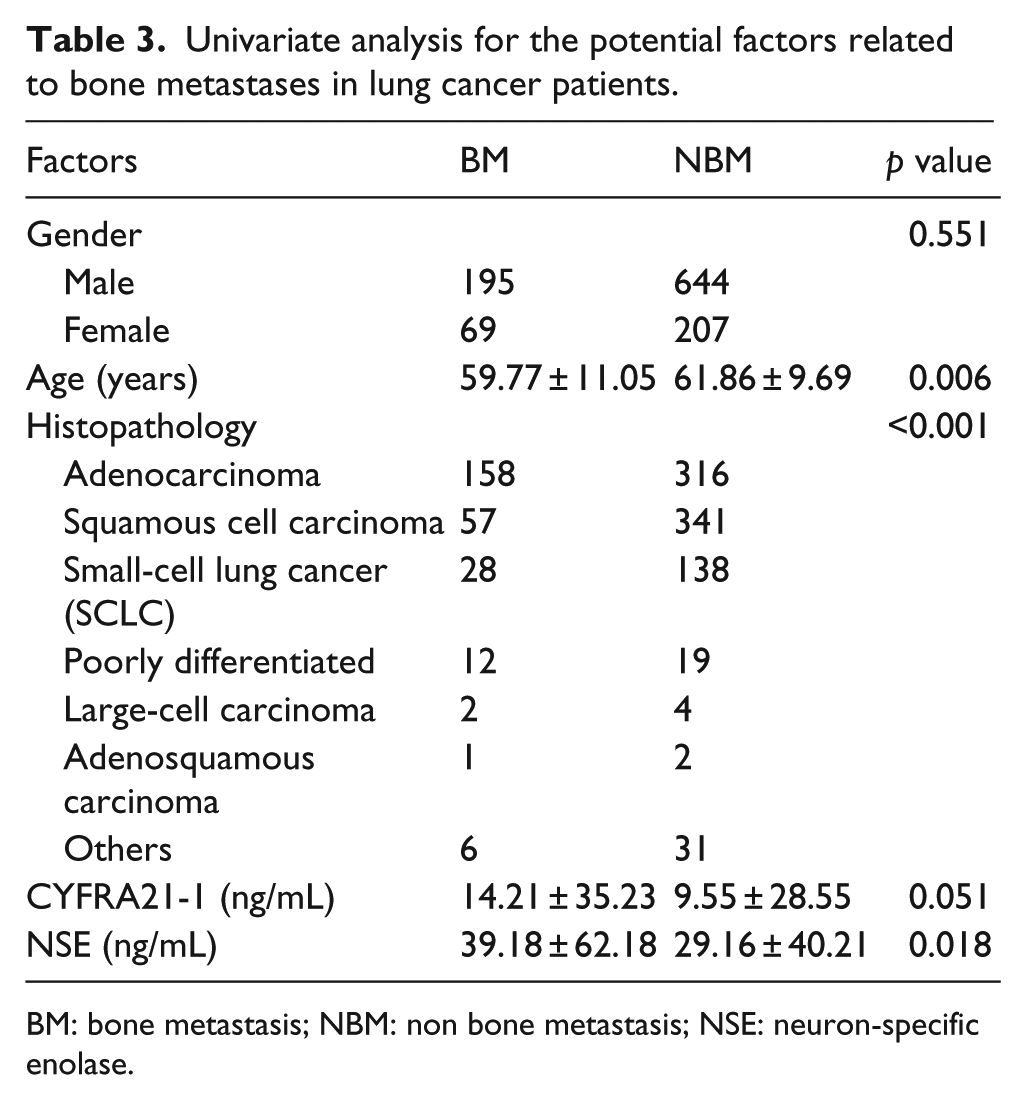
BM: bone metastasis; NBM: non bone metastasis; NSE: neuron-specific enolase.
The concentrations of biomarkers associated with bone metastases in lung cancer
The average serum concentration of CYFRA21-1 was 14.21 ± 35.23 ng/mL and 9.55 ± 28.55 ng/mL in patients with and without bone metastases, which was not significantly different (p = 0.051). The concentration of NSE was significantly higher in patients with bone metastases (39.18 ± 62.18 ng/mL) compared with patients without bone metastases (29.16 ± 40.21 ng/mL) (p = 0.018; Table 3). These results indicated that the serum concentration of NSE was potentially related to the bone metastases in patients with lung cancer.
The risk factors of bone metastases in lung cancer
Finally, multivariate logistic regression analysis was carried out to identify the potential risk factors for bone metastases in lung cancer. The results showed that patients’ age (odds ratio (OR) = 1.024, p < 0.001), the concentrations of NSE (OR = 1.212, p = 0.004), and histopathological types (OR = 0.995, p = 0.001) were the independent risk factors for bone metastases in patients with lung cancer (Table 4).
Multivariate logistic regression analysis for the independent risk factors of bone metastases in patients with lung cancer.

CI: confidence interval; OR: odds ratio; B: coefficient of regression; NSE: neuron-specific enolase.
Discussion
Distant metastasis is a common phenomenon in malignant tumors. Lung cancer, also known as lung carcinoma, is a malignant lung tumor and easy to spread to nearby organs. Previous studies showed that lung cancer was the third most common forms of cancer to spread to bone. 11 Studies also reported a high incidence of bone metastases in lung cancer, which ranged from 15% to 40% at the time of diagnosis.12,13 Lots of researches have focused on the predictive factors of prognosis in patients with lymphatic and bone lesions and the mechanisms of lung cancer metastasis.14–16 In this study, the incidence of bone metastases at initial diagnosis was 23.7%, and patients with adenocarcinoma and younger age were easier to develop bone metastatic lesion than patients with other histopathological subtypes and older age. Moreover, our results revealed that patients’ age and histopathological types were the independent risk factors for bone metastases, which were in accordance with previous studies. 17 And we also found that the serum concentration of NSE was an independent risk factor for bone metastases in lung cancer.
NSE, a γ–γ or γ–δ dimer isoenzyme of enolase, was found mainly in mature neurons and cells of neuronal origin by Schmechel et al. 18 and Tapia et al. 19 Various studies suggested that NSE was not only a useful marker for tumor aggressiveness, but also a prognostic factor for distant metastasis.9,20,21 Dong et al. 22 indicated that NSE was a potential biomarker for non-small-cell lung cancer diagnosis. Darlix et al. 23 found that the serum NSE levels were independent prognostic factors for brain metastases in breast cancer patients. In addition, Windrichova et al. 24 detected that serum levels of NSE were significantly higher in patients with bone metastases compared with metastasis-free patients. In consistence with previous studies, our study indicated that serum NSE was an independent risk factor for bone metastasis in lung cancer patients. However, further study is needed to make clear whether NSE is a specific risk factor for bone metastasis in lung cancer.
As CYFRA 21-1 is an important tumor marker for lung cancer diagnosis, we determined the relationship between the concentration of CYFRA 21-1 and bone metastases in lung cancer in this study. CYFRA 21-1 was first described as a tumor marker and prognosticator for squamous cell carcinomas of head and neck. 25 Studies showed that elevated concentration of CYFRA 21-1 was shown to be associated with poor prognosis in patients with lung cancer. 26 Pierga et al. 27 revealed that CYFRA 21-1 was correlated with detection of cytokeratin positive (CK+) cells, which remained a strong independent prognostic factor in primary breast cancer. However, the relationship between CYFRA21-1 and bone metastasis in lung cancer is still unclear. The results of our study showed that there was no significant difference in the serum concentrations of CYFRA21-1 between patients with and without bone lesions, which suggested CYFRA21-1 was not an independent risk factor for bone metastasis in lung cancer.
There were also some limitations in this study, including retrospective design and insufficient data, which made some patients to be excluded from this study. In addition, some tumor markers were not included in this study because of missing data. And this may result in some risk factors as the bone metastases were not detected in the analysis. Moreover, patients included in this study just came from one single medical center, and multi-center study is necessary to confirm the results.
In summary, our results suggested that younger age, adenocarcinoma subtype, and the serum concentration of NSE were the independent risk factors for bone metastasis in patients with lung cancer. Physicians should pay attention to these factors and try to identify bone metastasis earlier while patients were primarily diagnosed as having lung cancer. Also, there were also some limitations in this study, and a multi-center study with a large population and sufficient clinical data are necessary to verify the results.
Footnotes
Acknowledgements
The first author (Y.Z.) and second author (W.-Z.C.) contributed equally to this study and share the first authorship.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the Department of Science and Technology Program of Jiangxi Province, China (Nos 20162BCB22022, 20162BCB23057).