
Abstract
Esophageal neuroendocrine neoplasms are rare. With the improvement and popularization of diagnostic methods, the morbidity statistics have increased annually in recent years. There are currently no treatment guidelines for esophageal neuroendocrine neoplasms, and surgery is the only cure. This usually involves radical surgery when the tumor is limited to the primary site or when only regional lymph node metastasis occurs. Surgical treatment is key to treating esophageal neuroendocrine neoplasms, but combined treatment with chemotherapy and radiotherapy can significantly improve patient survival. The effect of radiotherapy alone on this disease is poor. However, targeted endocrine therapy can improve endocrine hormone symptoms. The prognosis of patients with esophageal neuroendocrine neoplasms is mainly determined by the pathological stage. With the development of molecular biology techniques, the combination of targeted drugs and traditional chemotherapy is expected to provide novel ideas and directions for the treatment of esophageal neuroendocrine neoplasms in the coming years. In this article, the status of esophageal neuroendocrine tumor treatments was reviewed in detail.
Keywords
Introduction
Neuroendocrine neoplasms (NENs) originate from the diffuse neuroendocrine system and the amine precursor uptake and decarboxylation (APUD) function of neuroendocrine cells (APUD cells). They are a heterogeneous group of tumors with biological behaviors that include slow growth, inertia, low-grade malignancy, significant malignancy, high invasiveness, and metastasis.1–3 Some types of NENs have a genetic predisposition and may be associated with genetic mutations, such as multiple endocrine neoplasia type 1 and 2 (MEN-1 and MEN-2), familial paraganglioma syndrome, von Hippel–Lindau syndrome, and Carney–Stratakis syndrome. 4 NENs are divided into two categories according to the clinical symptoms and levels of hormone secretion: functional and non-functional. 5 Over the past 15 years, the incidence of NENs has increased each year, although this may be due to the availability of improved diagnostic techniques; it further demonstrates that the incidence continues to rise. 6 NENs can occur in all age groups, but they are rare in children and young people. According to Feldman and Eiden, 7 NENs can occur in patients aged 10–93 years old, with a mean age of 55 years and a median age of 57 years. NENs can occur in multiple organs and tissues in the human body, including the gastrointestinal tract, pancreas, liver, gallbladder, bile duct, bronchus, lung, thyroid, parathyroid, adrenal medulla, paraganglia, and other neuroendocrine cells. The most common form is gastroenteropancreatic NENs (GEP-NENs), which account for about 55%–70% of all NENs. 8 The liver is the most frequent site of GEP-NEN metastases. The primary site, staging, and grading standards are used to determine the appropriate treatment or combination therapy.
Esophageal neuroendocrine neoplasms
Neuroendocrine neoplasms (NENs) of the esophagus are rare; an American study found that only 42 cases have been reported in the past 20 years, 9 accounting for 1.26% of esophageal malignancies and 1% of gastrointestinal endocrine tumors. 10 Using the World Health Organization (WHO) 2010 grading system, E-NENs are classified according to the criteria for GEP-NENs and are further divided into well-differentiated neuroendocrine tumors (NETs), poorly differentiated neuroendocrine carcinomas (NECs), and mixed adenoneuroendocrine carcinomas (MANECs). Almost all NECs are small cell neuroendocrine carcinoma (SCNEC) or large cell neuroendocrine carcinoma (LCNEC). MANEC refers to the occurrence of both NET and adenocarcinoma simultaneously, with the formation of ductal adenocarcinoma and NET morphology characteristics of epithelial tumors, with one component comprising at least 30%. The grading of E-NENs is usually based on histology and proliferative activity and is divided into G1, G2, and G3 (Table 1). In general, the classification corresponds with the grading. The lesions are usually located in the middle and lower parts of the esophagus.11,12 E-NENs rarely secrete hormones, and their clinical manifestations are similar to those of other types of esophageal cancer. 13 Common symptoms of SCNEC are dysphagia, weight loss, gastroesophageal reflux, and chest pain. The morphological features of small cell carcinoma include positive staining for NEN markers. Therefore, it is difficult to distinguish the clinical manifestations of NENs from other esophageal cancers. 14 However, a small number of cases can be identified as hormone-related syndromes, such as antidiuretic hormone secretion disorder syndrome. 15
Grading of neuroendocrine neoplasms.

HPF: high power field.
Pathology
The main clinical manifestations of NECs of the esophagus are dysphagia and chest pain. 16 In recent years, physicians have gained an understanding of the different types of NECs in terms of anatomy and morphological characteristics. The most common type is medullary, followed by mushroom, and ulcerative. 17 These tumors can be divided into different subtypes according to their histopathological and morphological characteristics and degree of differentiation. The majority are NECs and MANECs. 18 Small cell–type tumors have similarly sized small cancer cells: The nucleus is round or short and spindle-shaped; the nucleoli are not obvious; the cells are arranged in a row with unclear boundaries; there is no necrosis; and the cells are extruded or exhibit a wire-drawing phenomenon. 19 LCNECs have a slightly larger cancer cell volume compared with pure, small cell–type, with at least three-fold the size of tumor cells as that of lymphocytes, less cytoplasm, and round, oval, or spindle-shaped nuclei. The cancer cells are arranged in sheets or nests, and cluster structures that resemble chrysanthemums can be seen in some areas. 20 Mixed cell–type tumors contain two types of cancer cells in a diffuse distribution; they can be arranged in an irregular shape or form solid nests or cord-like arrangements. Some cases also present with adenoid or squamous differentiation and often stain positive for neuron-specific enolase, cytokeratin, chromogranin, and synaptophysin on immunohistochemical staining. The combined detection of these markers can improve the disease diagnosis rate. 21 The structures of neuroendocrine granules and desmosomes have been observed under an electron microscope. Neuroendocrine granules are the basis for the diagnosis of SCNEC by electron microscopy; these granules are round or oval with a clear boundary and a high electron density. The cytoplasm is rich in ribosomes, mitochondria, vacuoles, and vesicles, with a rough endoplasmic reticulum and a low content of Golgi complexes and lysosomes.
Diagnosis
The most commonly used clinical imaging methods are ultrasound, computed tomography (CT), and magnetic resonance imaging. Esophageal radiography can accurately show the extent and length of the lesion, the interruption or destruction of mucosal folds, irregular filling defects, and mass shadows that may be associated with lesions of the upper esophagus or stenosis. CT and enhanced CT may provide useful information regarding tumor location, density, relationship with adjacent organs, and metastasis, as well as facilitate the elimination of primary small cell lung cancer. 22 Of course, the final definitive diagnosis still depends on pathological immunohistochemical staining.
Somatostatin receptor imaging (SRS) is currently the gold standard functional imaging technique for NENs. SRS relies on NENs and metastatic lesions that express high levels of the somatostatin receptor of the cell surface. It combines radionuclide-labeled somatostatin analogs and tumor imaging, usually multifinger 111In-labeled octreotide single-photon emission CT imaging. It is worth noting that the value of endoscopic ultrasonography is superior to traditional imaging for the diagnosis of NENs. At present, the E-NENs diagnosis technology relies on the most advanced angiography techniques; it is mainly performed using specific vein intubations and analyzing specific hormones using radioimmunoassays, which can help to verify the position of the tumor. 23
Treatment
The treatment of E-NENs includes chemotherapy, radiotherapy, and surgery; surgical treatment is the main method used to cure the disease (Figure 1).
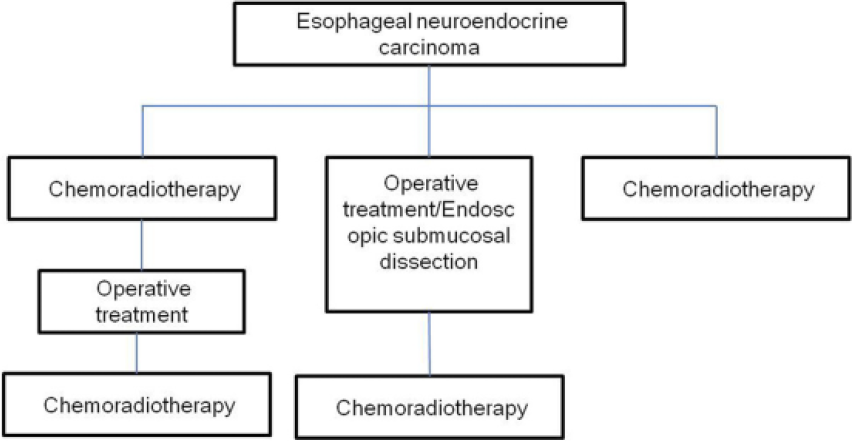
The main treatment methods for esophageal neuroendocrine carcinomas.
Surgical treatment
E-NENs are a group of heterogeneous, mild, malignant digestive tract tumors, and surgery is the only curative option. The type of surgical procedure used depends on the location of the NENs, the depth of invasion, the tumor size, regional lymph node metastasis, and distant metastasis in the liver. The principle of the operation is to remove the primary tumor as far as possible and to clean up all the metastatic lymph nodes and metastases. 24
There is currently no consensus regarding the treatment of SCNEC of the esophagus, which may be related to the lack of a large number of cases and large-scale clinical studies. In recent years, as the number of treatments has increased and treatment experience has accumulated, the importance of operations has been accepted and multidisciplinary treatment modalities including surgical treatment and postoperative adjuvant chemotherapy have received more and more attention. It is widely believed that the choice of treatment is mainly based on clinical stage. The disease is subdivided into limited and extensive lesions according to the scope of the lesion and the presence of lymph node metastasis. Limited lesions are confined to the esophagus and the surrounding tissues with or without local lymph node metastasis. In contrast, extensive lesions extend beyond the limited scope of the index and involve distant organ or lymph node metastasis.
The combination of radical resection, radical lymph node dissection, and chemotherapy achieves significantly better effects than radiotherapy and chemotherapy alone or in combination and can prolong survival, improve quality of life, and improve the prognosis of patients with limited-stage disease.25,26 Brega-Massone et al. 27 reported three cases of esophageal SCNEC. All patients underwent radical surgery but received no postoperative treatment. Two of the cases survived for 219 months and 193 months, confirming the efficacy of surgical treatment. Situ et al. 28 analyzed 44 cases of small cell esophageal carcinoma that received resection of the esophageal carcinoma and lymph node dissection. They concluded that esophageal cancer resection and lymph node dissection should be the first choice for limited-stage small cell esophageal carcinoma, especially for patients with no regional lymph node involvement.
Like other gastrointestinal malignancies, the liver is the most common site of distant metastasis of esophageal NENs. The treatment of NETs associated with only liver metastases remains controversial. There have been reports that surgery or radiofrequency ablation surgery can improve the survival of patients with NETs with liver metastases.29,30 Nagahama et al. 31 reported the case of a patient with esophageal SCNEC and liver metastasis who underwent esophageal and gastric resection plus hepatic artery catheterization and postoperative hepatic artery perfusion chemotherapy with cisplatin and fluorouracil. The patient survived for 4 years without recurrence. In addition, GEP-NENs are currently treated using interventional methods such as radiofrequency ablation, local freezing, partial arterial ligation, and chemical embolism to reduce the tumor burden directly or indirectly. These methods are often used in patients who do not have or are unable to tolerate surgery. It improves symptoms and is less invasive than surgery, but there are complications.
Endoscopic treatment
As digestive tract endoscopy and treatment technologies continue to improve, treatment with gastrointestinal endoscopy can achieve excellent results with early-stage tumors with a small diameter and a shallow depth. 32 Yagi et al. 33 reported a rare case of esophageal carcinoid tumor with endoscopic esophageal submucosal tumors of ~3 mm in diameter, a rosy glossy surface, and no ulceration or erosion on magnifying endoscopy with narrow-band imaging. Magnifying endoscopy with narrow-band imaging showed a submucosal microvascular network structure. Endoscopic ultrasonography revealed a hypoechoic tumor within the muscularis propria, and CT demonstrated that there were no signs of tumor or other organ metastasis. Endoscopic submucosal dissection (ESD) was used to resect the tumor. Enlargement of the endoscopy revealed that the tumor was rich in reticular blood vessels. Immunohistochemistry showed that the esophageal carcinoid tumor (NET, grade 1) had no lymphatic or vascular invasion. Li reported 24 cases of endoscopic foregut NENs that received ESD treatment: 23 of the 24 cases were G1 or G2, and the mean follow-up was 24.4 months. 34 There were no cases of lymph node or distant metastasis during the follow-up period. In addition, only one NEC patient (G3) experienced damage to the submucosa with a 3-cm lesion that was resected using ESD surgery; the patient survived till the 18-month follow-up. Therefore, ESD is an effective and low-risk treatment for NENs limited to mucosal lymph node metastasis. However, because NECs often have a high degree of malignancy, lymph metastasis cannot be excluded even in lesions confined to the mucosal layer. ESD surgery cannot be used for lymph node dissection, and the postoperative risk for local recurrence and metastasis may be high; therefore, some specialists recommend chemoradiation before and after the operation.35–37 Casas et al. 38 reported that the median survival of patients with E-NENs treated with topical therapy alone versus topical therapy combined with chemoradiation is 5 months versus 20 months, respectively. Other studies have also shown that the therapeutic effect of topical therapy combined with chemoradiation is better than that of topical therapy alone.39–41
Chemotherapy
There is a high probability of recurrence and metastasis in patients with esophageal NEC who receive surgery alone or even complete resection. As such, preoperative or postoperative chemotherapy may be critical in improving the survival rate. 41
There is currently no standard choice of chemotherapy. Ding et al. 39 reported 106 cases of limited SCNEC who received different treatments. Surgery alone or radiotherapy alone had 5-year survival rates of 0%, and the median survival time was 11 months. In comparison, surgery combined with chemotherapy or radiotherapy achieved a combined 5-year survival rate of 27.2% and a median survival time of 22 months. Surgery combined with chemotherapy and/or radiotherapy achieved better survival than surgery alone or radiation therapy (p = 0.001). Univariate and multivariate survival analyses showed that chemotherapy is an independent prognostic marker for survival. Chen et al. 42 reported 40 patients with limited-stage SCNEC. Patients who underwent radical surgery and postoperative chemotherapy exhibited better survival. The most common chemotherapy drugs were platinum-based two-drug combinations. 43 The treatment of extensive esophageal neuroendocrine cancer is based on systemic chemotherapy. However, the therapeutic effects of chemotherapy are very limited, which may be related to the low mitotic rate, high expression of the antiapoptotic protein Bcl-2, and drug-resistant genes in poorly differentiated tumors.44,45
Radiotherapy
There is no uniform standard for the indication of radiotherapy for esophageal NEC, and it is generally suggested that the appropriate dose of radiotherapy and the target area for patients with tumor infiltration and regional lymph node involvement should be selected based on the principle of radiotherapy for esophageal cancer.46,47 The decision as to whether to treat patients with esophageal endocrine tumors remains controversial. At present, many patients with G1 disease do not receive radiotherapy, whereas the appropriate radiotherapy is selected for G2 and G3 patients based on the tumor location and the patient’s condition. Because of the high expression of somatostatin receptors in NETs, somatostatin analogs such as 111In-octreotide, 117Lu-octreotide, 90Y-octreotide, and 90Y-lanreotide are usually used in radiotherapy. Previous studies demonstrated that 117Lu-octreotide is the most effective because of its increased survival rate and decreased adverse reactions in the liver and kidneys.48,49 For some advanced cancers, when surgical therapy is not an option, chemoradiotherapy becomes the first choice of effective treatment. 50
Biological therapy
Somatostatin analogs and interferons (IFNs) are mainly used as biological therapeutics. Many neuroendocrine cells secrete hormones. Somatostatin regulates hormone secretion by binding to its receptor and inhibiting the activity of adenylate cyclase and reducing calcium channel opening to block hormone synthesis and secretion. The somatostatin analog octreotide is a long-acting agent that can inhibit disease progression and improve the survival time in patients with well-differentiated metastatic NET. Octreotide can also significantly improve the clinical symptoms of NENs such as diarrhea, wheezing, and flushing, which may be related to its ability to inhibit 5-hydroxytryptamine receptor (5-HT) and neuropeptide K synthesis and release. 51
IFN-α not only plays an important antiviral role but can also inhibit the growth of tumor cells by inhibiting angiogenesis. IFN-α can maintain the NEN tumor volume and even make some tumors shrink. IFN is mainly used in digestive tract NENs with a low proliferative capacity, especially a Ki67-positive index <2%; however, it is not recommended in patients with a Ki67-positive index >100. 52
Targeted therapy
Targeted molecular mechanisms involve various growth factor receptors expressed by esophageal endocrine tumors, such as vascular endothelial growth factor and epidermal growth factor. Specific binding to these receptors is used to block the downstream signaling pathways, reducing tumor cell growth and proliferation. 53 Molecular targeted drugs do not harm normal cells. Research shows that bevacizumab targets vascular endothelial growth factor to inhibit the growth and proliferation of tumor cells. In addition, bevacizumab can also be used in combination with other chemotherapy drugs such as capecitabine to synergistically enhance the curative effects. Monoclonal antibodies are a hot topic of current research for tumor treatments because of their high specificity and fewer adverse reactions.
Conclusion
In summary, NETs of the esophagus are very rare. Compared with other digestive tract NETs, NECs are invasive with a high degree of malignancy and poor prognosis. 54 The clinical symptoms are similar to those of more common esophageal cancer; therefore, pathology is the gold standard for diagnosis. Immunohistochemistry is an important complement to pathological diagnosis. The key to improving the curative rate is early detection and the selection of a reasonable and comprehensive treatment. Surgery is essential in the treatment of local esophageal NENs, but combined treatment with chemotherapy and radiotherapy can significantly improve the survival time. The effects of radiotherapy alone are poor, but targeted endocrine treatments can improve the outcome of patients with endocrine hormone symptoms. Patient prognosis is mainly determined by the pathological stage. In recent years, the development of molecular biology–based targeted drugs combined with traditional chemotherapy is expected to provide novel directions for the treatment of this disease.
Footnotes
Acknowledgements
All authors contributed to the data analysis. Z.M. prepared the manuscript preparation; H.C. edited the manuscript editing; and Y.C. reviewed the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.