
Abstract
Brachyury has been characterized as a driver of epithelial–mesenchymal transition process which is regarded as an important mechanism of cancer cell invasion and metastatic progression. The status of tumor-infiltrating lymphocytes has been proposed to predict response to neoadjuvant chemotherapy in breast cancer. We investigated the clinical significance and value of tumor-infiltrating lymphocytes and brachyury as biomarkers to predict treatment responses to neoadjuvant chemotherapy in breast cancer. We also examined the correlation of the Neo-Bioscore with tumor-infiltrating lymphocytes and brachyury to indirectly predict long-term outcome. This retrospective study included a series of 44 consecutive patients treated between January 2011 and December 2015. All patient samples were obtained using core needle biopsy before neoadjuvant chemotherapy. The relationship of expression of Brachyury and tumor-infiltrating lymphocyte subsets (CD8+, forkhead box protein 3 tumor-infiltrating lymphocytes) with clinicopathological factors was assessed to identify its predictive role with respect to tumor response to neoadjuvant chemotherapy and the outcome. Of 44 patients, 6 showed no response, 31 had partial response, and 7 demonstrated pathological complete response. Forkhead box protein 3 was significantly higher in the response group than in the no response group (no response = 2.6, partial response = 7.0, complete response = 9.7, p = 0.020). Brachyury expression was inversely associated with response to neoadjuvant chemotherapy, but the difference was not statistically significant (p = 0.62). We also observed a significant association between forkhead box protein 3 (p = 0.001) and the Neo-Bioscore, while only a marginal difference was observed with CD8+ expression (p = 0.074). This study demonstrated that forkhead box protein 3 expression has value as the only independent marker that predicts a good response to neoadjuvant chemotherapy and that it is related with a good prognosis according to the Neo-Bioscore. Brachyury was significantly associated with estrogen receptor positive and human epidermal growth factor receptor 2 negative status; further study would be needed to clarify how it affects treatment prognosis.
Keywords
Introduction
Recently, many patients with breast cancer have undergone neoadjuvant chemotherapy (NAC), which facilitates conservative surgery and the early systemic treatment of micrometastases. It can also evaluate the degree of tumor response to chemotherapy, which is helpful for further treatment. Additionally, pathologic measures of disease burden and/or biological characteristics of the primary tumor, including pathological complete response (pCR), have been found to be significantly related to patient prognosis.1–4
Tumor-infiltrating lymphocytes (TILs) have been known as a prognostic factor for treatment response. In particular, high expression of TIL subpopulations such as CD3, CD4, CD8, and forkhead box protein 3 (FOXP3) is known to predict the pCR rate after NAC.5–8 Cytotoxic CD8+ T lymphocytes have the ability to destroy cancer cells. FOXP3, a marker of Treg cells, plays a role in controlling the transition and function of Treg cells. Treg cells deactivate CD8+ T lymphocytes and consequently decrease the function of co-stimulatory proteins in antigen-presenting cells. In other words, Treg cells inhibit the induction of cytotoxic CD8+ T lymphocytes. Based on this theoretical background, it has recently been reported that the CD8+/FOXP3+ ratio (CFR) has high predictive power as an indicator of a high pCR rate after NAC.9,10
Epithelial–mesenchymal transition (EMT) is a normal developmental process during which cells lose epithelial characteristics and obtain properties of mesenchymal cells in the normal formation of the fetus.11,12 Recent studies have shown that similar changes in the course of tumor development lead to the loss of polarity and intercellular connections of cancer cells, tumor invasiveness and metastatic potential, and resistance to chemotherapy.13–15
Brachyury is a member of the T-box family of transcription factors, characterized by a highly conserved DNA-binding domain named the T-domain, which was first discovered in 1927. 16 T-box transcription factors, including brachyury, are known to be involved in EMT and cancer formation, and high expression of brachyury messenger RNA (mRNA) has been found to be associated with a high likelihood of recurrence and distant metastasis.17–20 Moreover, brachyury-expressing cells have enhanced ability to invade the extracellular matrix and become resistant to chemotherapy.21,22 However, there have been no studies regarding the correlation between brachyury expression and tumor response in patients with breast cancer undergoing NAC.
We evaluated TIL subsets (CD8+ and FOXP3+) and the expression of the EMT marker brachyury in pre-chemotherapeutic breast tumor biopsy specimens. We then investigated the clinical significance and value of CD8+, FOXP3+, the CFR, and brachyury as biomarkers to predict treatment responses to NAC in breast cancer. We also examined the correlation of the Neo-Bioscore with TILs and brachyury to indirectly predict long-term outcome.
Materials and methods
This retrospective study included a series of 44 consecutive patients treated at our institution (Kangbuk Samsung Hospital, Seoul, Korea) between January 2010 and December 2015 for operable breast carcinoma with NAC followed by surgery. All patient samples were obtained before NAC using core needle biopsy and fixed in 10% formaldehyde solution and then embedded in paraffin. Medical records, pathology reports, hematoxylin and eosin (H&E)-stained sections, and immunohistochemical (IHC) slides for basic biomarkers were reviewed to acquire clinicopathological information, including patient age, sex, initial clinical T and N stages (based on Union for International Cancer Control/American Joint Committee on Cancer (UICC/AJCC), 7th edition), pathological T and N stage after NAC, histological subtype (by World Health Organization (WHO) classification), histological grade (by Bloom and Richardson grading system), lymphovascular invasion (L/V invasion), estrogen receptor (ER) status, progesterone receptor status, human epidermal growth factor receptor 2 (HER2) status, Ki-67 proliferation index, and menopausal status.
Therapeutic effects were assessed according to the Response Evaluation Criteria in Solid Tumors (RECIST). 23 The tumor responses after NAC were classified into three groups: pCR, partial response (PR), and no response (NR). pCR was defined as the absence of invasive cancer cells and lymph node metastasis, regardless of the presence or absence of noninvasive cancer cells. PR was regarded as a decrease in tumor size of at least a 30% in the sum of the longest diameter (LD) of target lesions, taking as reference the baseline sum LD. NR was considered as a concept including progressive disease (PD) and stable disease (SD), as defined in RECIST. The study protocol was approved by the Institutional Review Board of Kangbuk Samsung Hospital, the Sungkyunkwan University of Korea, on 30 August 2016 (KBSMC 2015-06-029-008).
Neoadjuvant therapy regimens
All patients underwent core needle biopsy before NAC. Of the 44 patients, 27 (61%) were treated with the AD regimen, consisting of 50 mg/m2 doxorubicin intravenous (i.v.) on day 1 and 75 mg/m2 docetaxel i.v. on day 1 every 3 weeks for four cycles; 2 (5%) received the AC regimen, consisting of 60 mg/m2 doxorubicin i.v. on day 1 and 600 mg/m2 cyclophosphamide i.v. on day 1 every 3 weeks for four cycles; and 15 (34%) received sequential adjuvant chemotherapy (ACT) comprising four cycles of AC followed by four cycles of 100 mg/m2 docetaxel. All patients with HER2+ breast cancer also received trastuzumab triweekly (6 mg/kg) with docetaxel treatment. The patients underwent breast surgery about 3–4 weeks after the last chemotherapy cycle.
IHC scoring
Scoring for each IHC marker was performed by an experienced breast histopathologist (D.S.-I.) who was blinded to the results of other markers and patient identity. IHC staining was performed on 3-µm-thick paraffin block sections. Briefly, the sections were dehydrated and deparaffinized in xylene and then rehydrated in a graded series of alcohol solutions. Staining was optimized using positive and negative controls and primary antibodies directed against ER (1:200; SP1; Lab Vision Corporation, Fremont, CA, USA), progesterone receptor (1:200; PgR636; Dako, Glostrup, Denmark), HER2 (1:1; clone 4B5; Ventana Medical Systems, Tucson, AZ, USA), Ki-67 (1:200; MIB-1; Dako), CD8 (1:100; clone C8/144B; Dako), and FOXP3 (1:100; clone 236A/E7; Abcam, Cambridge, UK). Immunostaining was performed using a compact polymer method (Bond Intense Detection Kit; Leica Biosystems, Newcastle upon Tyne, UK). The primary antibodies were detected with Dako EnVision+ Systems (HRP; DakoCytomation, Glostrup, Denmark), according to the manufacturer’s instructions. The Dako EnVision+ Detection Systems, Peroxidase/DAB (DakoCytomation, Glostrup, Denmark) was used to perform chromogenic visualization. The slides were then counterstained with hematoxylin, and coverslips were applied. To evaluate CD8 and FOXP3 expression, five stained areas were selected, and the number of TILs in stroma surrounding the stained cancer cells was measured quantitatively in each field under 200× magnification (Figure 1). The CFR was defined as the number of CD8+ TILs divided by the number of FOXP3+ TILs. 9

Examples of main tumor CD8 and FOXP3 expression as assessed with immunohistochemistry in breast cancer. (a) CD8 immunohistochemistry (IHC) stain in breast carcinoma highlights abundant CD8+ T lymphocytes (200× magnification). (b) FOXP3 IHC stain in breast carcinoma highlights FOXP3+ lymphocytes (200× magnification).
To evaluate brachyury expression, we used a rabbit monoclonal anti-brachyury antibody (MAb 54-1) at a 1:500 dilution. 24 For each slide, three to five random fields were evaluated; for each field, the percentage of positive tumor cells was calculated as ((number of positive tumor cells/total number of tumor cells) × 100). Nuclear staining was scored, with observation of brachyury in the nucleus. The relative staining intensity was scored as weak (+) for pale brown intensity, moderate (++) for intermediate brown intensity, and strong (+++) for intense, dark brown immunoprecipitate (Figure 2). We used the brachyury index to evaluate the immunoreactivity of brachyury. The brachyury index was calculated by multiplying the percentage of positive cells by the staining intensity. 25
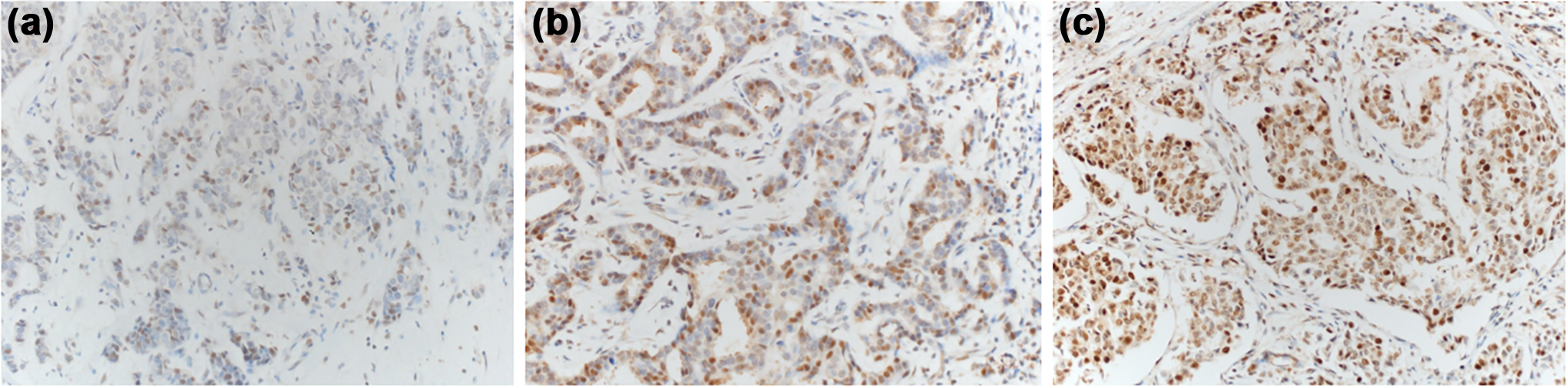
Immunohistochemical analysis of brachyury expression in breast cancer. (a) Weak nuclear expression of brachyury (200× magnification). (b) Moderate nuclear expression of brachyury (200× magnification). (c) Strong nuclear expression of brachyury (200× magnification).
Neo-Bioscore
The Neo-Bioscore was created due to a limitation of the CPS + EG staging system, which was designed to predict the prognosis of patients receiving NAC by presenting clinical stage, final pathological stage, and the biological markers ER and grade. As the routine use of trastuzumab in treating patients with HER2-positive breast cancer results in higher pCR rates and improved outcome than those achieved with chemotherapy alone, the CPS + EG staging system is not useful in predicting the prognosis of patients with HER2-positive cancer. Therefore, a study on predicting disease-free survival (DFS) and overall survival (OS) by adding HER2 status to the pre-existing CPS + EG staging system was conducted. The superiority of the new system was acknowledged, and this was named the Neo-Bioscore staging system. 2 It was demonstrated that the Neo-Bioscore stratified patients with respect to disease-specific survival (DSS), with 5-year DSS estimates ranging from 48% to 99% (p < 0.001; Table 1). In this study, we used the Neo-Bioscore calculated with 0–2 points or 0–1 points given to six clinicopathogical factors, including clinical and pathological stage, ER status, HER2 status, and nuclear grade, and each score was added to determine a total score between 0 and 7 (Table 2). In this study, because of the limitation of the small sample size, the Neo-Bioscore values were divided into two groups: scores of 0 to 2 points were defined as the low group and scores of 3 to 7 as the high group based on prognostic differences of each point. We compared the differences in TIL and brachyury values between the groups and analyzed the correlation with prognosis indirectly.
Five-year DSS outcomes by Neo-Bioscore.

CI: confidence interval.
Point assignments for Neo-Bioscore staging systems.

ER: estrogen receptor.
Statistical analyses
All statistical analyses were performed using IBM SPSS version 24.0 software (IBM Corp., Armonk, NY, USA). Associations among variables were evaluated using Fisher’s exact test or the Chi-square test for category variables and one-way analysis of variance (ANOVA) or Student’s t-test for continuous variables. To detect independent predictive factors for pCR, multinomial logistic regression was performed for univariate and multivariate analyses. All tests were two-sided, and p < 0.05 was considered statistically significant.
Results
Clinicopathological factors and their association with response to NAC
The study population consisted of 44 patients; all were women. pCR was achieved in 7 (15.9%) patients and PR was achieved in 31 (70.5%), with the remaining patients demonstrating NR. The clinicopathological characteristics of the patients are summarized in Table 3. As expected, high Ki-67 index (>14) significantly differed among the three groups (p = 0.044), but there were no statistical differences according to histological grade (p = 0.077). ER status (p = 1.000), L/V invasion (p = 0.387), menopausal status (p = 0.599), and age (p = 0.515) were also not associated with tumor response after NAC (Table 3).
Clinicopathological characteristics of the patients.
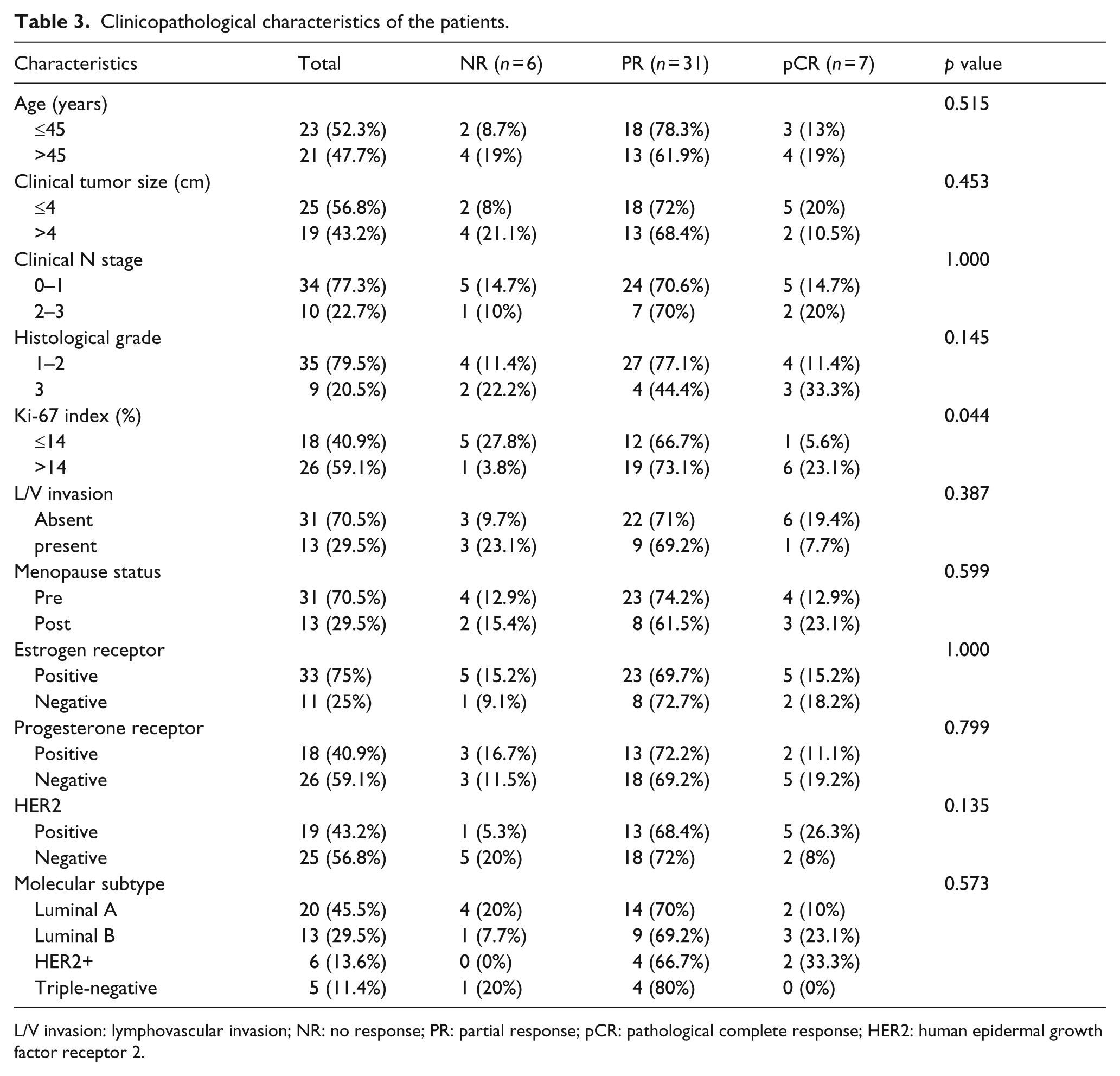
L/V invasion: lymphovascular invasion; NR: no response; PR: partial response; pCR: pathological complete response; HER2: human epidermal growth factor receptor 2.
Correlations between CD8+, FOXP3+, CFR, brachyury, and response to NAC

Relationships between (a) CD8+, (b) FOXP3+, (c) CFR, and (d) brachyury index and tumor response group.
We performed a multinomial logistic analysis to confirm whether FOXP3+ is an independent predictor of pCR. The results showed that FOXP3+ was still considered to be an independent predictor, even after adjusting for Ki-67, ER, HER2 status, L/V invasion, and histological grade, which were possibly associated with tumor response in other studies (p = 0.035; odds ratio = 1.664; 95% confidence interval (CI) = 1.036–2.675; Table 4).
Predictive factors for PR and pCR in multinomial logistic regression analyses.
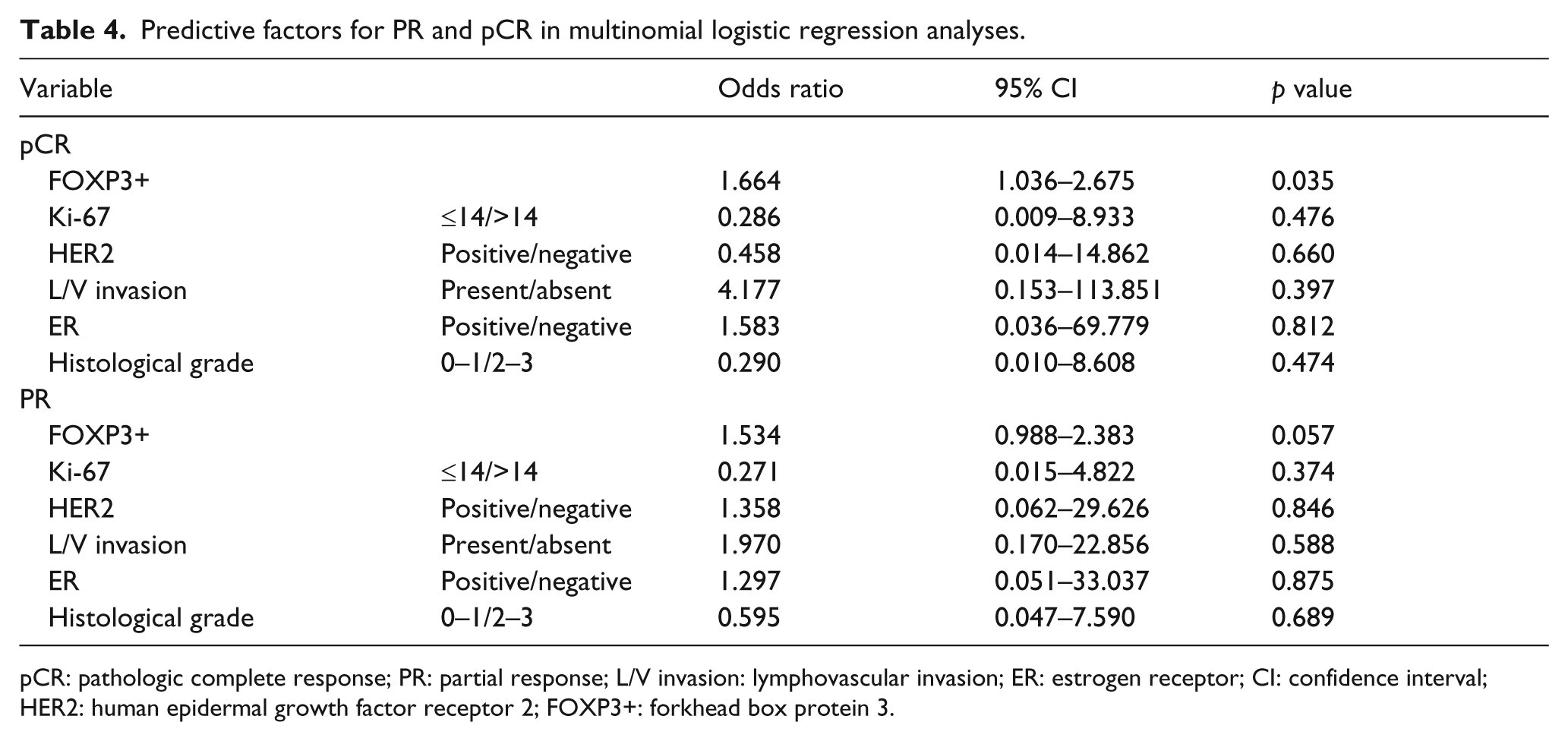
pCR: pathologic complete response; PR: partial response; L/V invasion: lymphovascular invasion; ER: estrogen receptor; CI: confidence interval; HER2: human epidermal growth factor receptor 2; FOXP3+: forkhead box protein 3.
Predictive value of CD8+, FOXP3+, CFR, and brachyury for long-term outcome using Neo-Bioscore
In this study, the Neo-Bioscore of patients ranged from 1 to 5 points: 1 in 15.9% of patients, 2 in 25%, 3 in 36.4%, 4 in 15.9%, and 5 in 6.8%. Therefore, 18 of 44 patients (40.9%) were included in the low group (score = 1–2), representing better prognosis, and the others were in the high group (score = 3–5). We hypothesized that high values of FOXP3+ and CD8+ might correlate with good outcome and the high expression of brachyury with poor outcome, based on previous reports. Indeed, we observed significant associations between FOXP3+ (p = 0.001), CFR (p = 0.016), and the Neo-Bioscore, while CD8+ demonstrated a marginal difference (p = 0.074). In the high group, the brachyury index was higher than that in the low group, as expected, but the difference was not statistically significant (p = 0.684; Figure 4). The tumor response rate, which was defined as pathologic tumor size divided by clinical tumor size, was significantly higher in the high group (p = 0.003). This finding may allow the presumption that the degree of tumor size response after NAC may be related to prognosis even without pCR.

Relationships between (a) CD8+, (b) FOXP3+, (c) CFR, (d) brachyury index, and (e) response rate and Neo-Bioscore. Error bars correspond to standard deviation.
Association of CD8+, FOXP3+, and brachyury with pathological factors
We compared the levels of TIL subsets and the brachyury index with various pathological factors commonly associated with prognosis. HER2-positivity was significantly associated with high levels of CD8+ (p = 0.025) and FOXP3 (p = 0.049) and low brachyury index scores (p = 0.032). Only the brachyury index showed a statistically significant difference according to ER status (p = 0.005). FOXP3+ was higher in tumors with a high Ki-67 index (p = 0.038), and the brachyury index tended to be high in tumors with L/V invasion, but this finding was of only marginal significance (p = 0.059). There were no statistical differences in TILs and the brachyury index for each tumor grade (Figure 5).
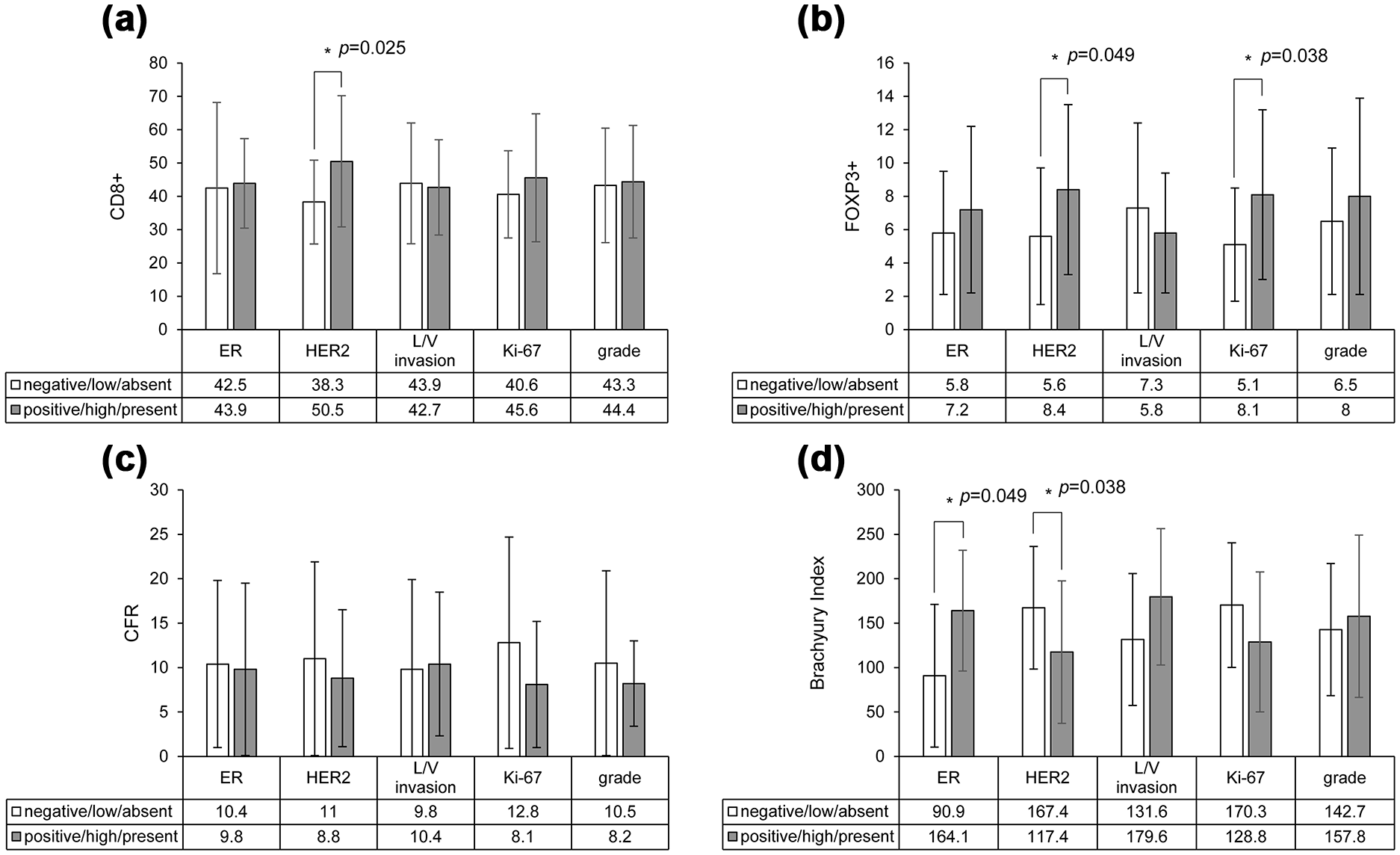
Relationships between (a) CD8+, (b) FOXP3+, (c) CFR, and (d) brachyury index, response rate and pathological factors. The mean values of each variable are displayed in tables.
Discussion
Based on the knowledge that brachyury has been shown to be associated with cancer cell invasion, metastatic progression, and chemoresistance in previous reports, we performed the first study comparing the tumor response to NAC to the expression of brachyury.21,22 We also tested the predictive values of expression of TILs and brachyury by analyzing how they relate to the Neo-Bioscore, a tool to predict long-term outcome. Additionally, we investigated the associations of prognosis with biological/pathological factors related to subtypes of breast cancer, which were demonstrated in previous studies.6,9,26,27
Recently, NAC has been increasingly used in operable breast cancer. There are several advantages to this approach, including decreasing the tumor size and eradicating nodal disease, resulting in minimization of the surgical extent.1,28 However, it is known that the therapeutic response to NAC is different according to each subtype and biologic marker. For example, ER-negative status and high Ki-67 index have been shown to be strongly associated with pCR. 6 It is important to select patients who are likely to experience high benefit from NAC, and many studies have been ongoing regarding potential predictive factors. TILs are indicators of the tumor immune microenvironment in the host against a cancer. Cytotoxic CD8+ T lymphocytes, a subset of TILs, lead to tumor cell death, while Treg cells deactivate CD8+ T lymphocytes. Although Treg cells were initially characterized as CD4+ and CD25high, 29 further investigation revealed that the transcription factor FOXP3 plays a role in controlling the transition and function of Treg cells. Since CD8+ T cells and Treg cells have a paradoxical role in anti-tumor immunity, CFR was used to predict a pCR after NAC in several studies.9,10 However, the relationship between FOXP3+ and outcome has shown diverse results inconsistent with the initial hypothesis.9,10,30–34 One study reported that FOXP3+ was only associated with good outcome only in ER− tumors. 30 In this study, FOXP3+ was significantly higher in the response group than in the NR group (p = 0.020), and no differences were observed in CD8+ between the groups (p = 0.474). As a result, the CFR was lower in the high-response group (p = 0.025), which was not the expected result given previous studies. The explanation for these findings is the fact that FOXP3+ was more apparent than CD8+ in the differences between the groups. A few studies found that FOXP3+ was associated with a good prognosis, and the explanation for this finding was that FOXP3+ T cells may inhibit tumor-promoting inflammatory responses to microbes. 34 Another study has suggested that FOXP3+ is expressed in a heterogeneous population of cells that have both regulatory and non-regulatory T-cell functions. Thus, these cells produce cytokines such as transforming growth factor beta-1 (TGF-β1) and interleukin-10 from Treg cells and interferon gamma and interleukin-17 from non-Treg cells, which is why FOXP3+ shows a variety of results in relation to cancer prognosis. 35 Additionally, neither FOXP3+ nor CD8+ was associated with ER status, but both were significantly higher in HER2+ tumors. FOXP3+ also showed a statistically significant difference according to the Ki-67 index. These results may explain a part of why FOXP3+ was higher in the good response group, because HER+ and high Ki-67 are known common findings in cancers that show a good response to NAC.
Mechanisms by which CD8+ T cells induce EMT in human mammary epithelial cells are known to include exposure to TGFβ or transfection with EMT-inducing transcription factors. 36 Immune cells such as CD4+ Treg cells, CD8+ T cells, and macrophages produce diverse arrays of cytokines through inflammatory responses, among which TGFβ, tumor necrosis factor alpha (TNFα), and interleukin-like EMT inducer (ILEI) act as EMT mediators. Therefore, CD8+ T cells entering tumor cells cause an immune reaction, producing various EMT mediators or producing cytokines or chemokines that can induce an immune reaction, resulting in EMT. 37
Brachyury, known as a driver of tumor EMT, has been studied as a targeting protein as interest in immune therapy has increased recently. In particular, brachyury shows predominantly high expression in the triple-negative breast cancer (TNBC) subtype tumors that have a high rate of tumor metastasis and a poor prognosis. 38 It has also been found to be associated with recurrence, distant metastasis, and resistance to chemotherapy.17,20–22 A recent report showed that brachyury mediates tamoxifen resistance by regulating Sirtuin-1. 39 Therefore, brachyury-targeting immunotherapy approaches for the treatment of TNBC are currently undergoing clinical evaluation. 40 Our data showed that high expression of brachyury was strongly associated with HER− status, similar to previous study results (p = 0.032). However, this expression was also statistically significantly related to ER+ status, in contrast to the findings of previous studies (p = 0.005).25,38 An association between the subtypes of breast cancer and brachyury seems to be present, but there have been few studies on this topic, and further research is needed in the future.
The brachyury index was highest in the NR group (mean = 171.7; SD = 67.9) and lowest in the pCR group (mean = 130.0; SD = 84.3), but this difference was not statistically significant (p = 0.625), although the finding might be related to the poor treatment outcome, similar to previous study results. 22 This result was considered to indicate that brachyury may be associated with tumor resistance to anti-cancer drugs, but otherwise it may indirectly reflect that the brachyury index was strongly associated with ER+ and HER2− cancer, which is known to have a poor tumor response to NAC.
We used the Neo-Bioscore as an indirect prognostic measure in this study. The Neo-Bioscore is a recently introduced scoring system to predict DSS by adding HER2 status to the existing CPS + EG system. According to the authors who suggested this system, each score has a DSS ranging from 48% to 99% and has a significant statistical power (p < 0.001). 2 We used this method to investigate the effect of TIL, brachyury, and response rate on prognosis. Similar to the results of Correlations between CD8+, FOXP3+, CFR, brachyury, and response to NAC, showing that high FOXP3+ and low CFR were statistically related to the low group, which is expected to have a good prognosis, brachyury and CD8+ also showed the expected trends, but the findings did not reach statistical significance. The response rate was high in the low group, which was consistent with previous study results showing that the smaller the residual tumor burden, the better the prognosis.
This study was the first to demonstrate the association of brachyury with tumor response to NAC and the relationship between TILs, brachyury, and the Neo-Bioscore. The first limitation of this study concerns the relatively low number of samples (N = 44), which does not allow us to perform subgroup analysis of the breast cancer subtypes. Furthermore, since EMT-associated markers, including overexpression of mesenchymal proteins, such as vimentin and smooth-muscle-actin, and cadherin switching (reduced E-cadherin and overexpression of N-cadherin), were not investigated together, we could not confirm the association of EMT with brachyury and other biomarkers. Additionally, NAC has been in use in our institution since 2010, meaning that the follow-up period for the patients was too short to allow direct measurement of prognosis. Therefore, the prediction of the prognosis using the Neo-Bioscore may differ from the actual prognosis.
In conclusion, this study demonstrated that FOXP3+ has value as the only independent marker that predicts a good response to NAC and that it is related to a good prognosis according to the Neo-Bioscore. Brachyury was significantly associated with ER and HER2 status. Further study would be needed to clarify how these factors affect treatment prognosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.