
Abstract
Uterine leiomyomas, also called uterine fibroids or myomas, represent one of the most common benign tumour types in women of a fertile age. Leiomyomas arise due to transformation of the layer of smooth muscle cells of corpus uteri – the myometrium. Despite frequent occurrence of this disease, the molecular mechanisms behind the origin and development of leiomyomas are still relatively unknown. Most predisposed are obese women and women of African origin. In more than half of cases, leiomyomas remain asymptomatic. Genetic factors also have an important impact on the development of these hormone-dependent tumours. However, the clinical and molecular characteristics of familiar and sporadic leiomyomas can widely differ. The main reason is the heterogeneity of this disease and the abundance of factors which can underlie their tumourigenesis. Clinical diagnosis of uterine leiomyomas without surgical interference can be hindered in the case of small, mostly submucosal leiomyomas or if it is necessary to avoid potential malignancy of tumour. Also, medical treatment of uterine leiomyomas cannot be nowadays considered sufficient with many medical agents still being tested only within clinical research. The main goal of this article is to summarise known facts about the aetiology of leiomyomas, risk factors that contribute to their development, known molecular-genetic aberrations connected with the presence of leiomyomas as well as the possibilities of their diagnosis and treatment
Introduction
Uterine leiomyomas are the most common tumour type in pelvic minor with prevalence reaching up to 60% of women in their reproductive years. 1 The prevalence increases with age, peaking in women in their 40s. Leiomyomas arise due to monoclonal transformation of smooth muscle cell layer of uterus, myometrium, and consist of large amounts of extracellular matrix (ECM) that contain collagen, fibronectin and proteoglycan. 2 Leiomyomas remain in almost 60% of cases asymptomatic; 1 nonetheless, it is possible to expect that this number could be even bigger, because worldwide there still remains a large subset of undiagnosed women, mostly in developing countries. Furthermore, in many cases, uterine leiomyomas are diagnosed incidentally on clinical examination or imaging. Clinical presentation can lead to decrease in quality of life and includes dysmenorrhoea, pelvic pain, menorrhagia, infertility and complications during pregnancy. 3 The complications include shoulder dystocia, abnormal postnatal bleeding, ectopic pregnancy or even miscarriage. 3 All these mentioned symptoms can have secondary negative impact on sexual life, performance at work and relationships with other people. 4 Uterine fibroids are currently the most common indication for hysterectomy, which represents the second most common type of surgical intervention for women after caesarean section. 1 This high prevalence of leiomyomas constitutes indeed a great economical issue, particularly in the United States, where the annual costs for complete procedure for all patients with diagnosed leiomyomas, including surgical procedures, hospital admissions, outpatient visits and prescriptions, are estimated to range from US$4.1 to US$9.4 billion. 5 Indeed, there is significant disparity in costs between ethnic groups, with higher rates of hospitalisation and surgery in African-American women than in White women. 1 African-American women, or generally women with African origin, are more predisposed to develop leiomyomas and prevalence can reach up to 80%. 1 Leiomyomas can be considered as a quite heterogeneous group of diseases. 6 The size of bulks can vary from millimetres to tens of centimetres, or in other words, from almost microscopic to that which can fill the whole uterine cavity. Leiomyomas can be solitaire as well as multiple within the same uterus. 6 Furthermore, due to their monoclonal origin, 7 two myomas within the same uterus can differ in molecular-genetical background. Depending on their localisation, leiomyomas can be divided into four groups: subserous, intramural, submucosal and pedunculated (which can be further divided into pedunculated submucosal and pedunculated subserous). 2 Leiomyomas occur as well-differentiated structures, usually without any signs of degeneration. 6 This can be observed mostly in cases, when leiomyomas grow through their own venous system. The most typical type of degeneration is hyalinisation, though myxoid, haemorrhagic or cystic degradation types can also be observed. 8 Even though there are benign uterine lesions generally also referred to as leiomyomas (myomas, fibroids, etc.), there are variants with less or more non-typical traits, namely, mitotically active leiomyoma (MALM), atypical leiomyoma (ALM), cellular leiomyoma (CLM) and leiomyoma with uncertain potential (smooth muscle tumour of uncertain malignant potential (STUMP)). 9 Finally, even though there is an accepted assumption that benign leiomyomas should not be connected with the formation of malignant mesenchymal tumours, like leiomyosarcomas, in a few cases, structures with a dual character (containing structures typical for leiomyomas, as well as sarcomas)10,11 have also been found. It is also known that in the case of about 0.2% of patients with diagnosed leiomyomas, leiomyosarcomas have later also been diagnosed. 10
Factors affecting development of leiomyomas
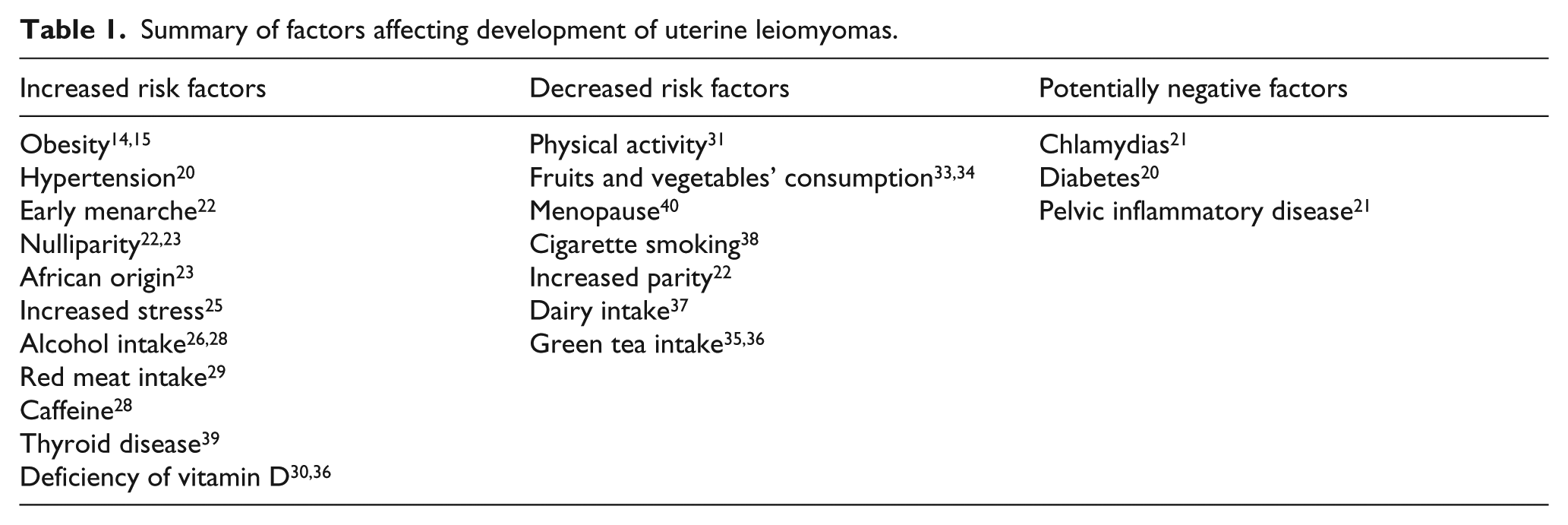
Among a plenty of factors, hormonal imbalance, mostly increased levels of oestrogens, 12 has a most significant impact on the development of uterine leiomyomas. Leiomyoma tissue is more sensitive to oestradiol or has more oestrogen receptors. These oestrogen receptors, presented within leiomyomas, bind 20% more circulating oestradiol compared to circumjacent myometrium. 13 Thus, leiomyomas can be considered in general as an oestrogen-dependent tumour. 13 This fact is connected to the higher frequency of leiomyomas within obese women. In such cases, the risk of developing leiomyomas is increased by 20% with every 10 kg over the normal value of body mass index (BMI). 14 Shikora et al. 15 generalised these facts and assessed analogical value in women in which body fat constitutes more than 30% of weight. Adipose tissues convert androgens from the adrenal gland and ovaries to oestrogens, whereas another mechanism associated with obesity decreases levels of hormone gonadal steroids, which bind globulin. 16 Development of leiomyomas is also affected by levels of progesterone, 17 of aromatase, which participates in synthesis of oestrogens, 18 and angiogenic growth factors, 19 which are involved in the vascularisation of leiomyomas. A higher occurrence of leiomyomas has been also observed in women with hypertension, 20 diabetes mellitus 20 and chlamydia infections 21 or within nulliparous women. 22 Women who have given birth to at least one child are less susceptible to development of leiomyomas probably due to remodelling processes of ECM. This process is associated with specific expression of steroid and peptide hormone receptors. 16 Development of leiomyomas is also statistically associated with early menarche – women who have menarche in an advanced age are affected less frequently. 22 No influence of postmenopausal hormonal therapy on leiomyomas formation has yet been detected. 23 Importantly, there are significant differences in the frequency and development of leiomyomas as such between women of African and non-African origin. In the case of women with African origin, collateral symptoms are more aggressive and these women are more predisposed to development as such, even by 300%. 24 Within this ethnic group, there are also typical more significant differences in growth patterns within the uterus of the same patient with non-solitaire leiomyomas. 12 As was mentioned, higher frequency of leiomyomas can be connected with negative aspects, which can be considered as non-strictly predisposed, like obesity or hypertension. Thus, it can be expected that proper living habit should potentially decrease frequency of occurrence of leiomyomas. A few studies have been concerned with such assumptions. Simplified, it can be claimed that women should avoid stress, adjust meal plan and increase physical activity. Psychological stress can be rated as a trigger of many tumour diseases, including leiomyomas, even this association cannot be considered as a strong positive, without evident presence of an increasing trend or dose effect. 25 Importantly, there were no significant difference among African and White women and impact of stress situations on tumourigenesis. Another, generally disfavourable factor alcohol can also contribute to the development of leiomyomas. Study performed on a group of pre-menopausal Japanese women revealed that the mean alcohol intake is statistically significantly higher among women with fibroids than among those without fibroids. 26 Study performed on a group of American women with African origin achieved similar results. 27 Caffeine intake can also negatively affect development of myomas; however, these connections were observed as significant only within group of women who intake more than 500 mg of caffeine per day. 28 Redundant consumption of red meat and ham can also negatively contribute to tumourigenesis of myomas – most of 843 Italian women with diagnosed leiomyomas reported (counter to women without leiomyomas) more frequent consumption of beef, other red meat and ham and less frequent consumption of green vegetables. 29 Ordinary presence outside, mostly during sunny days, should be also a protective factor against leiomyomas, as deficiency of vitamin D is also connected with higher prevalence of leiomymas. 30 Furthermore, regulation of amounts and effects of vitamin D represents nowadays very potential way to treatment of leiomyomas. However, besides general unhealthy aspects that contribute to development of leiomyomas, there are also generally known positive aspects that can reduce tumourigenesis of leiomyomas. Logically, anticipation can be a positive effect of sufficient physical activity. Fact that regular exercise might help women prevent fibroids has been documented by Baird et al., 31 who found out that women in the highest category of physical activity were significantly less likely to have fibroids. This trend was seen for both African-American and White women. Also, in different study, 32 authors found out that non-athletes were found to be 1.4 times more likely than former athletes to develop benign uterine tumours. Furthermore, women who consume enough amounts of fruits and vegetables are also less susceptible to occurrence of leiomyomas. 33 Consequently, it has been observed that vegetarians 34 have lesser risk of leiomyomas due to changes in oestrogen metabolism – they exhibited 15%–20% reduced oestrogen levels in plasma. Another beneficial situation should happen if women drink enough green tea. Even anti-proliferative effect of green tea extract – epigallocatechin-3 gallate – was proven first only in vitro, 35 and further studies 36 have proven that application of enough dose of this extract can force shrinkage of leiomyomas. Very interestingly, enough dairy intake is also inversely associated with leiomyoma growing pattern. 37 Mostly, in the past, effect of smoking on tumourigenesis of leiomyoma has been discussed. However, besides a plenty of negative effects, it can be really alleged that smoking has paradoxically at least one positive effect – antiestrogenic effect – which results in decrease in leiomyoma volume (Table 1). 38
Summary of factors affecting development of uterine leiomyomas.
Molecular-genetic background of tumourigenesis of leiomyomas
Our knowledge about the genetic background of the tumourigenesis of uterine leiomyomas can be considered quite imbalanced. There are known relatively large packs of aberrantly expressed genes,41–43 among which important oncogenes and tumour-suppressor genes are present. In any case, even notable aberrant expression of these genes should not be passably used as a typical sign of tumourigenesis of leiomyomas, because a lot of other factors can trigger these differences. Nonetheless, due to the monoclonal origin of leiomyomas, there can be differences in gene expression between two leiomyomas originated in the uterus of one patient. Different studies have established that about 40% of leiomyomas include some cytogenetic mutation. Some of these mutations cannot be considered as a random, but as a leiomyoma-specific. 44 Thus, a particular aberration could be connected with a particular abnormality in leiomyoma. The most frequent aberration presented in leiomyomas is rearrangement of 12q14-15, and within this group, translocation t(12;14)(q15;q23-24) dominates. 45 Quite often is also a paracentric inversion. 45 This particular translocation affects expression of the HMGA2. 45 This gene is evolutionarily highly conserved and belongs to the non-histone chromosomal high-mobility group A protein family. Members of this family are able to regulate transcription without the need for any structural changes in DNA strains. In other words, they act as factors that allow other regulatory proteins to bind to their target sequence. 46 While the expression of HMGA2 is abundant in developing tissues, in healthy differentiated adult tissues it is minimal. 47 In the case of uterine leiomyomas with mentioned translocation, HMGA2 is usually overexpressed. Particularly, in this case, chromosomal break points have been assigned to regions outside the open reading frame of HMGA2 gene, thus primarily affecting its expression, rather than its protein sequence. 48 Another, quite usual aberration is translocation 14q24 which affects functionality of RAD51B gene. 49 The product of this gene, as a member of RAD51 family, is essential for DNA repair by homologous recombination. 50 Coupled rearrangements between this locus and HMGA2 in leiomyomas have been also observed. 51 The most common deletion in uterine leiomyomas is an interstitial deletion of chromosome 7 – 7q22. This deletion appears in about 7% of leiomyomas with aberrant karyotype. 52 In this case, it is a bit harder to assess particular genes that are affected, because this region is considered to be ‘gene-rich’; this means that within its sequence, several different genes are encoded which can be affected independently based on the span of the mutation. 53 Notwithstanding, CUXI is considered in this case as (at least very potentially) affected gene, which plays an important role in the regulation of transcription. 51 This deletion usually occurs simultaneously, but sometimes also together with t(12;14)(q15;q23-24). 53 Typical for these sole deletions is that leiomyomas are much smaller in size. 51 Rearrangements of 6p21 occur in less than 5% of karyotypically abnormal tumours. This type of rearrangement is in leiomyomas represented mostly by translocations occasionally involving 14q23-24 and inversions. 54 In this regard, the HGMA1 gene is very often disrupted. This gene belongs to the same gene family as HMGA2, thus contributing to proper regulation of transcription. HMGA1 expression is less affected, due to this aberration, when compared to change in the expression pattern of the translocated HMGA2 gene. 54 Different, less frequent aberrations connected with the development of leiomyomas are trisomy of 12, 55 which can also probably in its final effect upregulate expression of HMGA 2, and monosomy of chromosome 10. 52 Furthermore, translocation within chromosome 10 (10q22) may affect regular transcription of KAT6B gene, which encodes one of the histone-acetyltransferase types. 56 An overview of both the mentioned and other less frequent regions aberrantly affected by leiomyomas is summarised in Table 2.
Chromosomal aberrations connected with the presence of leiomyomas.

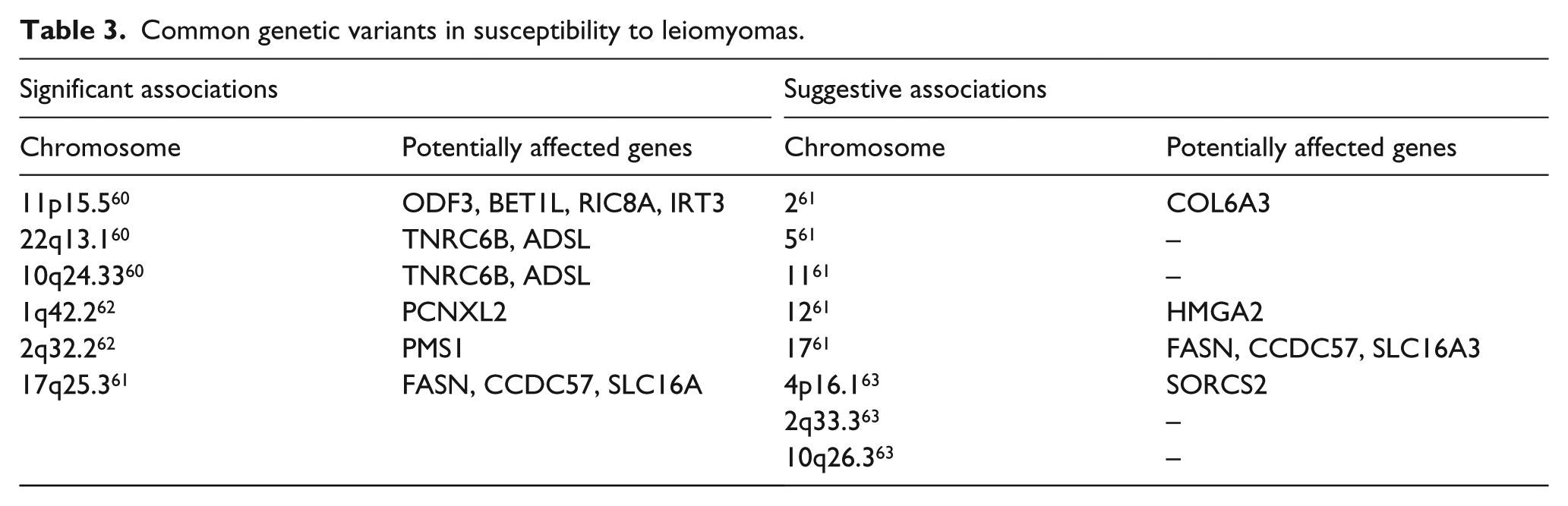
Besides the mentioned cytogenetic abnormalities, there is also a well-established knowledge about the impact of common low-penetrance risk variants in susceptibility to leiomyomas, which were achieved as a result of genome-wide association study (GWAS) examinations. After all, there can be discrepancies in the attempts to replicate previously achieved associations that are conducted by a different group of authors. Anyway, this can be caused due to the heterogeneity of leiomyomas in many aspects; in other words, tumourigenesis of leiomyomas can be dependent on a pack of multiple variants with a small effect. The very first wide and broad analysis was performed by Cha et al. 60 The authors, after genotypisation of more than 1600 patients from Japan, found three loci which were especially predisposed to structural changes among patients with leiomyomas. These loci were 10q24.33, 22q13 and 11p15.5. For the chromosome 10q24.33 region that showed the most significant association with uterine fibroids, the associated region was mapped to the 5′ region of SLK and OBFC1. Importantly, SLK gene encodes STE20 kinase, 60 which has a crucial impact on myogenic differentiation. For the chromosome 22q13.1 region, SNPs showing strong associations with uterine fibroids were mapped within a 200-kb linkage disequilibrium (LD) block, encompassing TNRC6B (trinucleotide repeat-containing gene 6B), encoding a component of the messenger RNA (mRNA)-degrading cytoplasmic processing (P) bodies that play a critical role in microRNA (miRNA)-mediated gene silencing and small interfering RNA–dependent endonucleolytic cleavage of complementary mRNAs. In the GWAS study of the European female population, 61 there was found another novel significant locus on chromosome 17q25.3, two significant linkage peaks on chromosomes 10p11.21 and 3p21.31 and then five suggestive peaks on chromosomes 2q37.1, 5p13.3, 11p15.5, 12q14.1 and 17q25.3. 17q25.3 spans fatty acid synthase (FASN), coiled-coil-domain-containing 57 (CCDC57) and solute-carrier family 16, member 3 (SLC16A3). Interestingly, the first named FASN was observed to be folded more than three times in leiomyomas within the same study. The list of both significant and suggestive associations based on the GWAS analysis is presented in Table 3.
Common genetic variants in susceptibility to leiomyomas.
Uterine leiomyomas are often accompanied with certain hereditary cancer-related syndromes, for instance, the hereditary leiomyomatosis and renal cell carcinoma (HLRCC) syndrome.64,65 Leiomyomas are associated with the explicitly specific traits of this syndrome, such as the early age of onset, higher prevalence, or a large nucleus with a prominent eosinophilic nucleolus surrounded by a clear halo. 65 HLRCC is caused by the heterozygous germline mutations of the fumarate hydratase (FH) gene. 66 X-linked Alport syndrome is also statistically associated with more frequent occurrence of leiomyomas. Alport syndrome arises due to defects in COL45A and COL46A genes. 67 Uterine leiomyomas are many times manifested together with Cowden syndrome, which is associated with defects in the PTEN gene, 68 or with Schwannomatosis, that is associated with defects in SMARCB1 gene. 69 The presence of leiomyomas spotted together with Gorlin syndrome (causative gene PTCH1) 70 or Tuberous sclerosis (causative genes TSC1, TSC2) is less often. 71 In either way, due to the high frequency of sporadic leiomyomas, it is necessary to take into account that simultaneous occurrence is often only a result of mere coincidence.
In the case of leiomyomas, the ECM is frequently affected by exposure to the increased levels of mechanical stress. The study of the pathogenesis of leiomyomas and their ECM has demonstrated that one of the most susceptible factors involved in this activity’s changes is transforming growth factor-β (TGF-β). 72 Particularly, the subunit β3, which is the only isoform expressed in mesenchymal cells, and its signal mediators are usually upregulated. 73 Also, the activity of this factor can negatively affect the activity of other growth factors. 72 No matter whether affected by TGF-β or not, the activity of several other growth factors, or their receptors, has been observed to be changing when leiomyomas have been presented. These are, namely, vascular endothelial growth factor (VEGF), epidermal growth factor (EGF), human heparin-binding epidermal growth factor-like growth factor (hHB-EGF), platelet-derived growth factor (PDGF), insulin-like growth factor (IGF), transforming growth factor-α (TGF-α), acidic fibroblast growth factor (aFGF) and basic fibroblast growth factor (bFGF). 74 BFGF and VEGF contribute to increased levels of angiogenesis. 74 EGF and PDGF positively modulate the synthesis of DNA via transient activation of different types of kinase pathways. 75 The previously mentioned TGF-β can affect the mitogen-activated protein kinase (MAPK)/extracellular signal–regulated protein kinase (ERK)/Smad signalling pathway, which can result in modulation of expression of various types of genes. 75 Finally, it is intriguing that the gene encoding this subunit is localised closely to 14q23-24 break points – one of the most common translocation sites identified in cytogenetic studies of fibroids. Unfortunately, there is a lack of connections between these two factors in case of leiomyomas. It would be of a great benefit to estimate whether an upregulation of TGF-β3 can potentially occur as a result of disruption of regulatory elements due to the translocation events, similarly as in the case of HGMA2 overexpression, or due to the somatic mutations unaffected by chromosomal rearrangements, as in the case of arrhythmogenic right ventricular cardiomyopathy (ARVC)-type disease. 76
Nowadays, the gene MED12 (mediator complex subunit 12) can be marked as a typical leiomyomas phenomenon, due to the mutations of this gene in almost 70% of fibroids with normal karyotype in patients from various ethnic and racial groups. The percentage was established as an outcome of whole-exome sequencing approaches.77–79 Notably, this mutation is also present in smaller proportions, within leiomyosarcomas, in about 10% of the cases, and in small portions of STUMPs.77,80 Nevertheless, this mutation can be still considered as strictly typical for leiomyomas. 80 Comparably, even there were observed different mutations of this gene, 81 the clear majority of MED12 mutations consists of missense mutations at codon 44, especially the amino acid change G44D. 81 Finally, MED12 has been shown to physically and functionally interact with b-catenin, the key effector of canonical Wnt signalling, to activate transcription of the target genes. 82 MED12 is also essential for embryonic development and its deletion disrupts both canonical Wnt signalling and Wnt/PCP. 83
A second somatic mutation, relatively typical for leiomyomas, can be considered mutation in FH gene. However, even aberrations in this gene are more likely to be associated with the deletions 1q43 or are considered as sporadic for HLRCC syndrome, and somatic mutations can be found in a smaller subset of nonhereditary leiomyomas. Particularly, based on immunohistochemistry (IHC) leiomyoma staining and subsequent MPS as well as Sanger sequencing approaches, 1% of all uterine leiomyomas should be FH deficient due to somatic inactivation. 57
Epigenetic background of tumourigenesis of leiomyomas
Epigenetic changes contributing to the development of leiomyomas are of various types. On the whole, the leading role in this case relates to the studies that are focused on the changes in the levels of DNA methylation. One of such wide-spectrum study has been conducted by Maekawa et al. 84 The authors of the study focused on mechanisms of deregulation of ER response genes using genome-wide DNA methylation and mRNA profiling in paired specimen of leiomyoma and adjacent healthy myometrium. Within the analysed genes, 120 of them showed differences in methylation levels between tumour and control specimens. Even these changes have not been gaping, they have been unambiguously present. Furthermore, 22 of these genes have consensus sequence of ER response elements. This group includes, for example, genes GSTM5, NUAK1, COL4A1 or DAPK1. Especially, DAPK1 aberrations are quite common in many cancer types due to the defect in methylation patterns within its promoter region. 85 These results prove the hypothesis that this gene should be aberrantly hypermethylated in case of leiomyomas, whereas in the previously conducted study, 86 there had been observed higher levels of methylation marks of this gene in sera of patients with leiomyoma, compared to healthy patients. In general, because leiomyomas are oestrogen-dependent tumours, it is possible to expect some intentions to connect epigenetic changes and the ER signalling pathway. One goal of such type of analysis can be identifying of changes in oestrogen receptor α (ERα), which is often abundantly expressed in cases of uterine leiomyomas. 87 Among the very first studies, dealing with this issue was a study conducted by Asada et al. 88 Using bisulphide sequencing approach, the authors gained much about expected results (if the higher expression is expected). Particularly, they sequenced and compared sequences downstream as well as upstream of ERα promoter and demonstrated that 49 CpG sites in the proximal promoter region showed no cytosine methylation in either healthy myometrium or tumour specimen. However, 7 CpG sites in distal regions showed variations in methylation levels between healthy and tumour specimens. However, the authors do not consider this variation as significant. Hori et al. 89 assume that changes in methylation status in the distal promoter region can be dependent on the phase of the menstrual cycle. Remarkably, when the same regions were analysed on the samples of endometrial diseases, there were observed discrepancies, because the levels of methylation of these promoter regions did not correlate with the lack of ERα protein in human patient samples with endometrial disease. 89 Furthermore, in the study by Sato et al., 90 an aberrant hypomethylation within sequences of X chromosome including TSPYL2 gene has also been demonstrated. These changes were connected to higher expression of this gene in normal myometrium, whereas expression was not upregulated in case of leiomyomas. In principle, similar analyses as made by Maekawa et al., 84 but using slightly different techniques were performed by Navarro et al. 91 carried out the similar analyses. The authors performed a comparison of the levels of DNA methylation and mRNA expression within a population of African-American women. Particularly, they found out that 55 of the candidate genes showed differences in the methylation pattern between leiomyoma and healthy specimens. These changes were concomitant with changes in levels of mRNA expression. Most significant changes were observed in DLEC1, KRT19 and KLF11 genes, which were significantly hypermethylated in leiomyomas. A study performed by Sato et al., 92 which has the purpose of assessing molecular markers that could reliably distinguish among healthy myometrium and leiomyomas, revealed 12 genes that could be potentially used as those markers. Furthermore, using hierarchical clustering system, the authors were able to discriminate uterine cancers and differentiate between uterine leiomyosarcomas and leiomyomas, with more than 70% accuracy. The genes that showed hypermethylation or hypomethylation in at least 70% of leiomyomas were ALX1, CBLN1, CORIN, DUSP6, FOXP1, GATA2, IGLON5, NPTX2, NTRK2 and STEAP4 (these genes were hypermethylated) and PART1 and PRL (hypomethylated genes; Table 4).
Aberrantly methylated genes (regulatory regions) in leiomyomas.

The disregulation of activity of genes caused by interaction with non-coding RNAs remains nowadays still a quite attractive domain within molecular biology. There have been made a few studies93–95 dealing with the effect of miRNA interaction on the development of different types of tumors, proving that miRNAs can affect essential processes in cells, including apoptosis, cell adhesion, cell proliferation Wnt signaling, and lastly that expression pattern of miRNAs can significantly differ. Nevertheless, only in the very first study dealing with this broad theme in the case of leiomyomas, 94 206 miRNAs were examined, whereas most overexpressed were miR-21, miR-23b, miR-27a and miR-30a and let-7 family members. MiR-29b, miR-32b, miR-144, miR-197 and mir-212 were shown to be significantly downregulated. Furthermore, Marsh et al. 95 identified 46 miRNAs, differently expressed in leiomyomas, whereas 19 of them were upregulated and 27 were downregulated. The most upregulated was miR-542-3b, which is proposed to target important anti-apoptotic factor survivin. 96 Pan et al. 97 used a multifaceted approach, incorporating paired myometrial and leiomyoma tissue, myometrial and leiomyoma isolated cells, as well as leiomyoma cell lines T-LSCM and SK-LMS-1. As a result, 91 miRNAs were identified as aberrantly downregulated as well as upregulated. A more recent study by Liu et al. 98 revealed that another almost 30 miRNAs can be differentially expressed in leiomyomas besides healthy myometrium, and more strikingly, significant differences in miRNA expression were observed among Caucasian women and women of African origin. However, miR-21, miR-27b, miR-29b, miR-197, miR-93 and let-7 family members are generally considered as very important miRNAs as these are connected to pathological processes leading to the development of uterine leiomyomas. Nonetheless, the final effect of mentioned miRNAs, as well as other miRNAs, is strongly associated, besides ethnicity, with tumour size and other secondary factors. 95 Elevated levels of miR-21 are very likely, in the case of leiomyomas, to be in inverse proportion with levels of PDCD4. 99 PDCD4 acts as an important tumour-suppressor gene, which is highly downregulated in many types of malignant tumours. 99 Although PDCD4 has been observed unexpressed in healthy myometrium and aberrantly overexpressed in leiomyomas, what makes this case quite unique, after knockdown of miR-21, the protein levels of PDCD4 increased in both leiomyomas and myometrium. 99 Furthermore, the expression of TGF-β receptor type II is probably the target of miR-21 in leiomyoma smooth muscle cells. Thus, lower expression of miR-21 in leiomyoma might represent the loss of one of the regulatory mechanisms, resulting in unregulated expression of TGF-β receptor and increased TGF-β activities. 100 The effect of miR-29b has been analysed within leiomyoma xenografts. 101 In this case, resumption of mir-29 affected the accumulation of ECM and the formation of solid tumours. Moreover, the authors suggest that abnormal production of ECM can be regulated by steroid hormones (17β-oestradiol and progesterone) via downregulation of miR-29b. Nonetheless, also other members of this family, namely, miR-29a and miR-29c, together with miR-29b, are downregulated in leiomyomas in vivo, which results in an increase in collagen III deposition. 102 Another abundantly expressed miRNA in leiomyomas – MiR-27b – targets human cytochrome P450, encoded by gene CYP1B1, which is an enzyme involved in oestrogen metabolism. A low level of miR-27b expression in MCF-7 cells has been inversely associated with CYP1B1 expression, and thus, vice versa, overexpression of miR-27b resulted in inhibition of CYP1B1 expression. 103 Let-7 family can strongly affect expression of HMGA2, 104 which is one of the most notable signs connected to leiomyomas. This relationship has been well described and documented as biologically significant for leiomyoma growth. 105 Chuang et al., 106 using a large cohort of leiomyomas and paired myometrium from untreated patients and patients exposed to hormonal therapies, demonstrated that miR-93/106b is differentially expressed in leiomyomas besides healthy myometrium. Particularly, the levels of expression of miR-93/106b were inversely proportional to the levels of expression of MCM7, its host gene, together residing at chr7q22. Additionally, through doxycycline-inducible lentiviral transduction in a microarray analysis, tissue factor (F3) and IL8 were identified as their possible targets. The gain of function of miR-93/106b dose dependently repressed F3 and IL8 through direct interactions with their respective 3′-untranslated region. Indirect interaction through tissue factor F3 was also ascertained; as a result, expression of CTGF and PAI-1 was inhibited. Furthermore, Chuang and Khorram 107 revealed that miR-200c also regulates IL8 expression, but in a different manner, via direct targeting of IKBKB and alteration of NF-κB activity in leiomyoma. At the same time, this miRNA can negatively affect the activity of ZEB1/ZEB2, TIMP2, VEGFA and FBLN5 genes in leiomyoma. 108 Another member of the mir-200 family, mir-200a, is supposed to target TUBB, CTBP2 and CYP1B1 genes. 105 Overexpression of miR-200a in UtLM cells led to growth inhibition, compared to mock infected controls, and reverted the fibroblastoid morphology towards more pronounced epithelial phenotypes.
MiR-197 has been identified to affect uterine leiomyoma cell proliferation, apoptosis and metastasis ability, though the responsible molecular mechanism has not been well elucidated. Nonetheless, it seems to be very presumable that aberrant expression of this miRNA could potentially dysregulate at least 17 genes (Table 5). 109
Dysregulated miRNAs and their targets in the uterine leiomyoma.

Cells were isolated and cultivated from fresh leiomyoma/myometrium tissue and subsequently transfected/transducted with desired elements. This tissue was also used for isolation of nucleic acid for conjoined analyses.
Besides analyses of methylation status and miRNA interaction, analyses focusing on changes in histone modification have also been performed, which aim to validate whether the modification type can also contribute to the development of leiomyomas. As an illustration, Bredfeldt et al. 110 revealed that rapid signalling from membrane-associated ER can regulate the histone methyltransferase enhancer of zeste homolog 2 (EZH2). EZH2, as a member of the polycomb repressive complex 2 (PRC2), catalyses trimethylation of lysine 27 of histone H3. 110 Particularly, in hormone-responsive MCF-7 cells, in response to xenoestrogen diethylstilbestrol (DES), ER signalling via phosphatidylinositol 3-kinase phosphorylates EZH2 at S21, which reduced the levels of trimethylation of lysine 27 on histone H3. In order to explicitly demonstrate the link between nongenomic ER signalling and modulation of EZH2 activity and H3K27Me3 levels in the developing uterus, the authors analysed nongenomic signalling in neonatal Eker rats exposed to DES. As a result, increased phosphoinositide 3-kinase (PI3K)/AKT signalling was consistently seen in all neonates exposed to DES. Furthermore, Greathouse et al. 111 found out that genistein and bisphenol A also induce ER signalling in the developing uterus; nonetheless, only genistein induce PI3K/AKT signalling to the EZH2. Genistein also causes oestrogen-responsive genes in the adult myometrium to become hyper-responsive. In other words, such a pattern of EZH2 engagement to decrease versus increase H3K27 methylation correlates with the effect of these xenoestrogens on tumourigenesis of leiomyomas.110,111 Summarily, based on this finding, it can be assumed, that environmental estrogens have distinct nongenomic effects in the developing uterus. Specifically, estrogens should have ability to engage the epigenetic regulator EZH2 what subsequently results in changes of levels of the repressive epigenetic histone H3K27 methyl mark in chromatin during developmental reprogramming. Thus, this mechanism could be connected with promotion of uterine (leiomyoma) tumorigenesis. Thus, if in utero environmental conditions are not optimal, this status can lead to epigenetic changes that can manifest tumourigenesis of leiomyoma in later stages of life. This fact had been analysed and suggested earlier by Greathouse et al. 112 In this study, Eker rats were exposed to (DES) as newborns. These animals later manifested permanent changes in gene expression of the myometrium throughout their adult lifetime. Particularly, based on the expression analyses, more than 170 genes were aberrantly expressed in leiomyoma, relative to normal myometrium.
Leiomyomas’ classification
Mostly used classification of leiomyomas is based only on their localisation within corpus uteri. Indeed, a more detailed and nowadays commonly used European Society of Gynaecological Endoscopy (ESGE)/Federation of Gynecology and Obstetrics (FIGO) classification system of leiomyomas is based not only on their localisation but also on their interaction with particular layers of uterine body. Based on these principles, three main grades can be assessed – primary, secondary and tertiary. 113 The primary grade is based only on the presence of at least one leiomyoma, regardless of its localisation, multiplicity or size. The secondary grade is primarily based on whether the particular fibroid is submucosal (SM) or not (O – other types); in other words, how much it affects the endometrial cavity. This division is based on the fact that submucosal leiomyomas are considered as a main factor in abnormal uterine bleeding. The leiomyoma tertiary classification system for hybrid lesions describes the endometrial relationship first and serosal relationship second, separated by a hyphen. In other words, if and how much leiomyoma deforms endometrium and, subsequently, if and how much deforms outer layer of serosa. Thus, tumour is first classified in accordance with submucosal classification and subsequently classified in accordance with subserosal localisation. 113

The FIGO leiomyoma classification subsystem. 113
Diagnosis of uterine leiomyomas
Lack in clinical diagnosis of uterine leiomyoma is often due to the absence of syndromes as well as reluctance to undergo gynaecological examination. Patients undergo examination usually after strong pain in the abdominal area or after abnormal bleeding. The first type of diagnostic examination is expectably bimanual examination. This type of examination is capable of diagnosing clinically significant subserosal and intramural leiomyomas. 114 However, more accurate diagnosis, mostly of submucosal leiomyomas, requires usage of advanced methods. Furthermore, nowadays, there is an accepted consensus to minimise invasive diagnosis techniques 115 because of the possibility of disruption of potentially malignant mass. Also, these methods can be besides that often false positive, as in the case of curettage. 115 Thus, mostly imaging methods are preferred to be used, or less invasive methods such as hysteroscopy, which is able to visualise large portion of uterine cavity and reveal submucosal leiomyomas, are used. 116 Applicability of imaging techniques based on their advantages and disadvantages is summarised in Table 6.
Summary of applicability of imaging techniques based on their advantages and disadvantages.
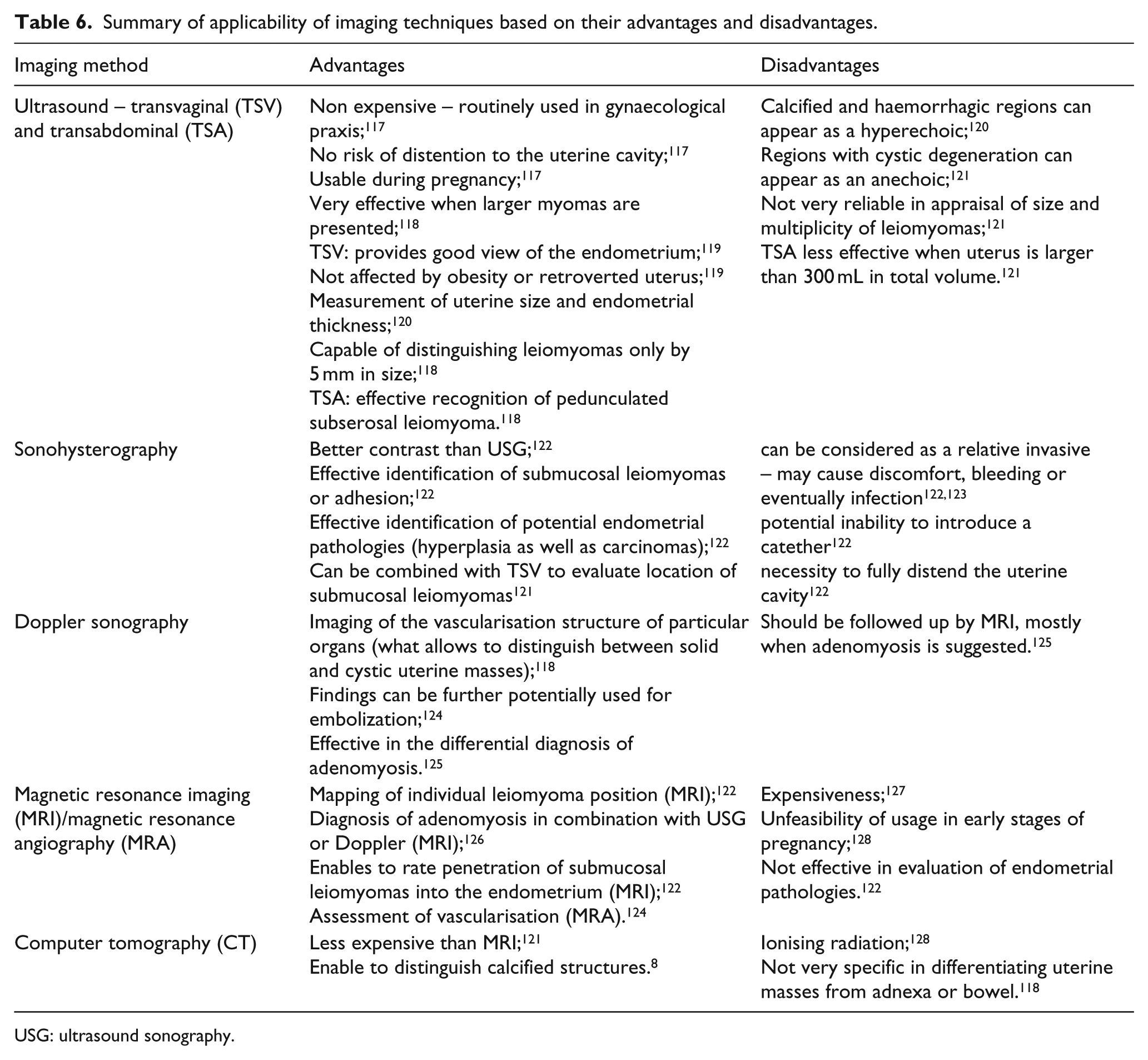
USG: ultrasound sonography.
The difficulty in diagnosis of uterine leiomyomas is differentiation between benign and malignant tumours. In many cases, this is possible only after invasive procedure. However, based on some studies, there is some possibility of distinguishing between leiomyomas and leiomyosarcomas when magnetic resonance imagination or transvaginal ultrasonography is used. 129 Through transvaginal ultrasonography, the structures that are typical of leiomyosarcomas can be visualised, such as echogenic structures or structures with central necrosis; however, these structures can be sometimes presented within leiomyomas. 129 Based on a study by Schwartz et al., 130 when magnetic resonance imaging (MRI) is used, the uncertain boundaries of a tumour can be considered as a significant marker of leiomyosarcomas. Interestingly, MRI with a gadolinium contrast medium showed predictive values of more than 50%. 131 Finally, X-ray examination of the lungs is often used to assess potential malignancy as a supplementary diagnosis because leiomyosarcomas often spread to this organ. 8
Potentials in medical treatment of uterine leiomyomas
Conventional treatment of uterine leiomyomas has been for quite a long period insufficient, with low efficiency and associated adverse levels. There are a few groups of medical products which differ in their final effects.
Gonadotropin-releasing hormone (GnRH) analogues inhibit release of gonadotropin, which results in a hypogonadal state. Leuprolide acetate in particular significantly reduced the bulk mass of leiomyoma compared to placebo. However, this effect was only temporary and the size of myomas increased again after treatment. Furthermore, leuprolide acetate had (together with other GnRHs) a negative effect on bone density. 130 Another GnRH analogue, triptorelin, positively reduced the size of leiomyomas after 8 weeks of treatment. 133 This study also showed that triptorelin’s effect is minimally changed when a normal or reduced dose is applied and how interestingly, in the case of a lower dose, it did not have any effect on bone density. Generally, GnRH agonist treatment is restricted to a 3- to 6-month interval, following which regrowth of fibroids usually occurs within 12 weeks. GnRH remains a quite effective pre-operative approach, which enables reduction of anaemia. 134
A GnRH antagonist does not downregulate GnRH receptors, but directly works in a competitive blockage manner. Importantly, it does not induce a hypogonadal state. One of these antagonists, cetrolexin acetate, is a very important target in many studies. Particularly, it has been proven that it can reduce the size of fibroids, 135 and besides that, it is also effective in treatment of other different diseases. 133 Another antagonist, danazol, competes with progesterone, androgens and glucocorticoids in receptor binding. Also, it is capable of decreasing levels of oestrogens by suppressing gonadotropin secretion and it inhibits ovarian steroidogenesis. 135 The final effect of these mechanisms becomes evident in a 25% reduction in volume of fibroids, 137 though only within cohort studies. Letrozole, as an aromatase inhibitor, inhibits the conversion of androgens into oestrogens. 138 A trial study involving 70 participants 138 has been performed comparing effects of letrozole and GnRH agonists. Use of letrozole reduced fibroid volume by 46% and use of a GnRH agonist by 32% after 12 weeks of treatment. A decrease in dysmenorrhoea was also achieved together with an increase in the haematocrit in symptomatic pre-menopausal women, without affecting the bone mineral density or serum levels of follicle-stimulating hormone and oestradiol. However, it remains important to point out the fact that these results were not statistically significant due to the lack of a control group, thus further investigation of letrozole effects needs to be done.
Application of ulipristal acetate, as a selective progesterone receptor modulator and also a factor that exhibits anti-proliferative effects on leiomyoma cells and the endometrium, 139 achieved quite positive results. When applied besides placebo, ulipristal acetate decreased the fibroid volume and levels of abnormal uterine bleeding. 140 There were also observed changes in the size of leiomyoma bulks. Finally, the authors claim that ulipristal acetate has no significant adverse effects. 140 Furthermore, it was shown not to be inferior to leuprolide acetate. In a parallel randomised controlled trial, ulipristal acetate appeared to be more or less effective as leuprolide acetate in controlling heavy menstrual bleeding. It has been able, at least partially, to control bleeding symptoms in 90% of the patients who consumed 5 mg of ulipristal acetate and 98% of the patients who consumed 10 mg. When leuprolide acetate was applied, it was effective only in 89% of patients. The median time to amenorhea was relatively similar in the case of all three groups, though reduction in uterine volumes was greater when leuprolide acetate was applied. Another study proved the positive effect of ulipristal acetate, since a reduction of bulk mass after 3-month treatment was observed. 141 The next selective progesterone receptor modulator, mifepristone, has, as an anti-progestin agent, antagonistic properties. Nowadays, mifepristone is used as an effective pre-surgical tool. 142 However, details about its mechanisms of reduction of leiomyomas are still not explained well. Nonetheless, the meta-study involving 780 pre-menopausal women 142 produced relatively positive results with a decrease in leiomyoma volume and alleviated leiomyoma-related symptoms. Also, in contrast with GnRH treatment, which is connected with a quite rapid return of symptoms, in the case of mifepristone application, reduction of symptoms lasts for up to 1 year after cessation of treatment. 143 Thus, this therapy can hide potential for patients who wish to avoid surgical intervention. Furthermore, mifepristone seems also to be dose-independent – there were no significant differences in leiomyoma size reduction between application of 5 and 10 mg doses. 143 Unfortunately, however, there are some indications that usage of mifepristone could contribute to development of hyperplasia. 144
Medical treatment of uterine leiomyomas (as well as other types of tumour diseases) can be limited due to patient aversion to clinical supervision or attempts at self-administered treatment, mostly with the help of Internet. In such cases, patients reach for products that are available online for treatment of uterine fibroids. Epigallocatechin gallate (EGCG) is one such product marketed for use alone or in combination with other herbal products. Fortunately, EGCG can really affect tumour growth. One of the first analyses of EGCG’s effect was performed on rat tumour cells by Zhang et al. 145 EGCG inhibited growth of tumour cells as well as induced apoptosis. Double-blind, 4-month, placebo randomised trial, in which 33 women with symptomatic leiomyomas participated, also provided relatively positive results. 36 In the case of a group of patients treated with 400 mg of green tea extract (containing up to 50% of EGCG), a reduction of leiomyoma volume was observed, while women within the control group experienced an increase in fibroid volume.
Vitamin D3 was shown to experimentally inhibit leiomyoma growth in vitro. 146 A linked study showed that its effect on leiomyoma cells is dose dependent. 147 These results can point to the fact that insufficient amounts of vitamin D can contribute to the development of uterine leiomyomas. In general, women of African origin, who are more susceptible to tumourigenesis of leiomyoma, are deficient in vitamin D in about 50% of cases, whereas only about 10% of White women are deficient. 148 Also, levels of serum vitamin D were detected to be significantly lower in the case of women suffering from leiomyomas than in healthy women. 149 However, there are no studies investigating vitamin D supplementation with regard to therapeutic benefits; thus, further investigation of the effect of vitamin D on the development of uterine leiomyoma is needed.
Conclusion
Uterine leiomyomas are nowadays the most frequent indication to perform hysterectomy. Hysterectomy, or at least myomectomy, is still roughly the only method that can in combination with consequent histopathological examinations provide sufficient information about the potential malignancy of tumours. Also, treatment of leiomyomas often ends with surgical interference due to underactive medical treatment. The main goal for the future is to develop methods that would help to distinguish uterine leiomyomas with a higher efficiency in situ as well as development of more effective medicaments that would minimise the necessity of hysterectomy, myomectomy or embolisation. In both of these aims, better knowledge about the molecular-genetical background and the origin and development of leiomyomas would be of great benefit. Leiomyomas as a tumour type of monoclonal origin forms a very heterogeneous group and even though heterogeneity can be widely observed in their aetiology and pathogenesis, the most heterogeneous feature is the genetic background of these tumours. In particular, tumours within the same uterus can be accounted for by aberrations in different genes, while tumours from two non-related patients can have almost identical defects. Thus, it is essential for us to determine more molecular-genetic factors and aberrations which will help us to gauge predisposition to tumourigenesis and the behaviour of the disease as well as to prevent the malignant potential of tumours.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Health of the Slovak Republic under the contract 2012/25-UKMA-2 and by the project Biomedical Centre Martin ‘ITMS code: 26220220187’ (the project is co-financed from EU sources).