
Abstract
Cancer is a disease with abnormally proliferating cells and therefore proliferation rate is an important index for assessing tumour growth. Ki-67 is a commonly used proliferation marker considered to be an unfavourable prognostic marker in some tumors, while Thymidine kinase 1 (TK1) is an interesting proliferation marker because its levels are highly dependent on the growth stage of cells. To define the immunohistochemistry (IHC) expression of the TK1 in patients with ovarian serous adenocarcinoma and establish its potential role as a new biomarker for progressive disease, we analyzed the expression patterns of TK1 and Ki-67 in 109 patients with ovarian serous adenocarcinoma. TK1 and Ki-67 expression both showed a statistically significant correlation to MD Anderson Cancer Center (MDACC) grade, but not to age, tumour size, lymph node metastasis or pathological TNM (pTNM) stages. TK1 expression, MDACC grades, pathological stages and lymph node metastasis correlate to relapse incident rate and overall survival, but Ki-67 does not. Although TK1 expression, MDACC grade, pTNM stage and lymph node metastasis significantly correlate to relapse in the Cox univariate analysis, in the multivariate Cox analysis only TK1 expression and lymph node metastasis were independent prognostic factors. The overall survival also correlated significantly to TK1 expression, MDACC grade, pTNM stage and lymph node metastasis in the Cox univariate analysis. However, only the pTNM stage was found to be an independent prognostic factor for survival in the Cox multivariate analysis. Therefore, though TK1 expression was an independent prognostic factor for relapse, but not for survival, TK1 is a more informative expression than Ki-67 for LI, relapse and overall survival rates. Thus, when TK1 is combined with MDACC grading, pTNM staging and lymph node metastasis, IHC determination of TK1 expression may improve the overall prediction of prognosis in patients with ovarian cancer.
Introduction
Ovarian cancer is the second most common gynaecological malignancy with a tendency to early distant metastases and a high mortality rate. The incidence rate of ovarian cancer in the United States is 0.012 with a mortality rate of around 67%.1,2 Corresponding values in China is 0.005 and 74%, respectively.3,4 Ovarian carcinomas comprise a heterogeneous group of tumours. Different epithelial subtypes of ovarian carcinomas have been defined: serous (50%–70%), endometrioid (10%–25%), clear cell (10%) and mucinous (5%). The serous subtypes can be subdivided into high-grade (75%) and low-grade (25%).5,6
In clinical practice, early and advanced serous ovarian cancer shows a large difference in prognosis because of the lack of typical symptoms and effective diagnostic methods for early ovarian cancers. Most patients are diagnosed at an advanced stage, and in about 70%–75% of these patients, the cancer has already spread throughout the whole peritoneal cavity.6,7 Recurrence of serous ovarian adenocarcinoma after treatment is high; therefore, assessment of risk of recurrence is an important issue for follow-up and further treatment.
One of the greatest obstacles to the detection of early-stage ovarian cancer was the poor understanding of its histogenesis and pathogenesis,8–11 but understanding of the underlying pathogenesis and initiating molecular events in the different tumour subtypes has greatly increased.
Studies on the biomarkers most related to ovarian cancer did not find specific markers to associate with the different ovarian carcinoma subtypes. 12 The expression of 21 biomarkers (CA125, CRABP-II, EpCam, ER, F-Spondin, HE4, IGF2, K-Cadherin, Ki-67, KISS1, Matriptase, Mesothelin, MIF, MMP-7, p21, p53, PAX8, PR, SLPI, TROP2 and WT-1) in 500 patients with ovarian carcinoma differed significantly between subtypes, but did not vary across stages within each subtype. The univariate Cox regression analysis for disease-specific survival of each subtype showed only three remaining prognostic markers (WT-1, MMP-7 and PR) in the high-grade serous subtype (n = 200) but none in the clear-cell subtype. The proliferation marker Ki-67 varied markedly between different subtypes and had no prognostic significance within any subtype. 12
Cancer is a chronic disease of abnormally proliferating cells, and therefore, proliferation rate is an important index for assessing tumour growth. Ki-67 is a commonly used proliferation marker.13,14 However, the expression of Ki-67 varies between different subtypes of ovarian carcinoma and is considered in some studies to be an unfavourable prognostic marker for ovarian serous adenocarcinoma.12,15 Thymidine kinase 1 (TK1) is an interesting proliferation marker because its levels are highly dependent on the growth stage of cells. 16 TK1 converts deoxythymidine (TdR) to thymidine monophosphate (TMP), and this is the only pathway to introduce TdR into DNA metabolism. TK1 is a key enzyme in synthesizing the deoxythymidine triphosphate (dTTP) needed for DNA synthesis and repair. 17 TK1 is absent in resting cells, is present at the G1/S boundary and increases dramatically by the late S-phase/early G2 phase during the cell cycle. 16 TK1 is degraded in mitosis. Therefore, TK1 was suggested for use in assessing of tumour cell proliferation. However, because there was a lack of optimal anti-TK1 antibodies, TK1 was not promoted for immunohistochemistry or for serology in clinical settings until new generation of anti-TK1 antibodies were developed over the last 10 years. Initial immunostaining using these TK1 antibodies showed that TK1 was an independent prognostic factor for survival in patients with cervical carcinoma, 18 pT1 adenocarcinoma of lung19,20 and malignant peripheral nerve sheath tumours. 21 A comparison between TK1 and Ki-67 showed that Ki-67 was not an independent prognostic factor for survival in patients with cervical carcinomas or lung pT1 adenocarcinoma.18,20 It was also demonstrated that serum TK1 was an independent prognostic factor for the risk of recurrence in breast carcinoma22,23 and for survival rates in breast carcinoma, 24 gastric carcinoma, 25 and Hodgkin’s lymphoma. 26
In this study, we investigated whether TK1 expression could serve as a prognostic factor for relapse and overall survival in serous ovarian adenocarcinoma patients and compared these results with those for Ki-67.
Materials and methods
Study outline
A retrospective study of 109 patients with ovarian serous adenocarcinoma was performed at the Nanjing General Hospital of Nanjing Military Region, from 1997 to 2010, with complete clinical and pathological data (including patient age, maximum tumour diameter, tumour site(s), regional lymph node metastasis and follow-up after surgery, with or without recurrence). The study was based on the World Health Organization (WHO) classification of breast and female genital cancer pathology and genetics to choose the tissue types diagnosed as serous adenocarcinoma (excluding other histological types such as mucinous carcinoma, endometrial carcinoma, clear cell carcinoma and undifferentiated cancer). 6 The MD Anderson Cancer Center (MDACC) classification system was used for histological grading. 10 A distinction was made between type I low-grade tumours and type II higher grade epithelial malignancies. 8
In standard pathological tumour–node–metastasis (pTNM) staging, the clinical stages are as follows: T1: tumours limited to the ovaries; T2: tumours involved in unilateral or bilateral ovaries with pelvic extension; T3: tumours involved in unilateral or bilateral ovarian, with microscopically confirmed metastases in pelvic peritoneum and/or regional lymph node metastasis and M1(T4): distant metastasis (peritoneal metastasis excluded).27,28
Patient characteristics
Patients’ mean and median age were 51.8 and 52.0 years, respectively (range = 22–79). The mean maximum tumour diameter was 7.5 cm (range = 2–22 cm); 41 cases were of unilateral tumour types, while 68 cases were of bilateral type; 52 cases were accompanied by regional lymph node metastasis and 45 showed no distant metastasis. The pTNM stages were distributed as T1 (n = 11), T2 (n = 11), T3 (n = 73) and M1 (n = 14), and MDACC grades were low level (n = 17) and high level (n = 92).
Treatment and follow-up
Of the 109 patients, 97 underwent radical hysterectomy plus pelvic lymph node excision, while the other 12 had radical hysterectomy without pelvic lymph node excision. In this group, 91 patients also received routine cisplatin-based chemotherapy. 10 Patients were followed up through medical records and telephone contacts. Information was obtained up to January 2013, including the time of surgery and whether the patient was still living.
The patients were followed up for 26–173 months, average 79 months. Information on relapse and overall survival were obtained during follow-up.
Immunohistochemistry
Tumour tissues were fixed with 4% neutral formalin and paraffin embedded. The tissues were immunohistochemistry stained with TK1 mAb (clone 5, dilution 1:800; SSTK Biotech., Inc., China) or with Ki-67 mAb (MIB1, dilution 1:200; Santa Cruz Biotechnology, USA). The EnVision two-step immunoassay (Dako, Denmark) was used in the staining procedure, following the product manual.
TK1 and Ki-67 expressions were examined under optical microscope. TK1 expression was found both in the cytoplasm and nuclei in 95% of the patients and only in the cytoplasm in the other 5%. Ki-67 was found only in the nuclei of the tumour cells. The number of TK1- or Ki-67-stained tumour cells was counted in 200 tumour cells in representative areas (no fewer than five high power fields) and expressed as percentage: ⩽5%, 6%–25%, 26%–50% and ⩾51% and were denoted as score 1, 2, 3 and 4, respectively. The score 1–2 was denoted as low level and score 3–4 was denoted as high level (see Figures 2 and 3).
Statistical data
Data analysis was performed with SPSS 16.0 (SPSS, UK). Pearson χ2 test was used to compare TK1-LI and Ki-67-LI expression in relation to the clinical parameters studied. To further evaluate diagnostic precision, intra-variability and the kappa coefficient were determined. A kappa value ⩾0.75 shows good consistency, while a kappa value ⩽0.4 is considered as poor consistency.28–30 The Kaplan–Meier method was used for overall survival analysis. Cox proportional hazards regression was used for univariate/multivariate analysis. A p value <0.05 was considered as statistically significant.
This study was conducted in accordance with the Helsinki Declaration of 1983 and was approved by the Ethics Committee of Jinling Hospital, Medical School of Nanjing University (No. 2015NZKY-013-01). The Chinese Clinical Trial Register number is ChiCTR-OOC-15006925.
Results
Immunohistochemistry
Ki-67 expression was found in the nucleus (Figure 1(a) and (b)) and LI was 82.0%. The 95% of TK1 protein staining was found both in nuclei and cytoplasm (Figure 1(c) and (d)), and only 5% was found in the cytoplasm (not shown in the figure), as previously described for several types of tumour cells. The LI for TK1 was 85.8%. The highest number of patients with TK1 and Ki-67 expressions were found in score groups 3 (TK1, n = 52; Ki-67, n = 28) and 4 (TK1, n = 28; Ki-67, n = 45).
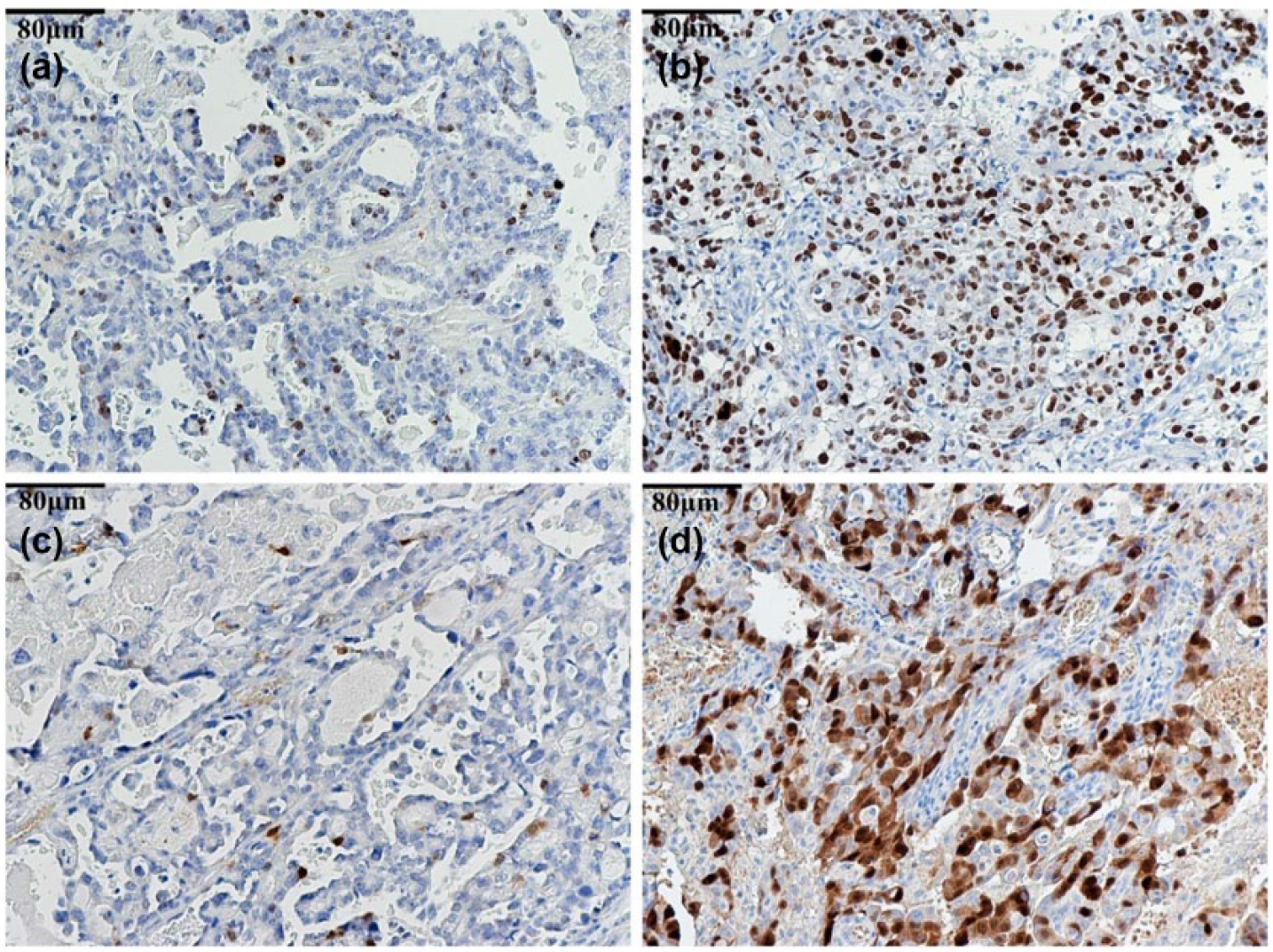
Expression of TK1 and Ki-67 in ovarian serous adenocarcinoma. TK1 shows cytoplasmic and nuclei staining, while Ki-67 shows staining only in the nucleus. (a) Ki-67 with low level (score 1; 200×), (b) Ki-67 with high level (score 4; 200×), (c) TK1 with low level (score 1; 200×) and (d) TK1 with high level (score 4; 200×).
The relationship between TK1 and Ki-67 expressions and the clinical parameters is shown in Table 1. The TK1 and Ki-67 expressions correlated significantly to the MDACC grade, but not to age, maximum tumour diameter, lymph node metastasis or pTNM stages.
TK1 and Ki-67 expressions in relation to clinical characteristics.
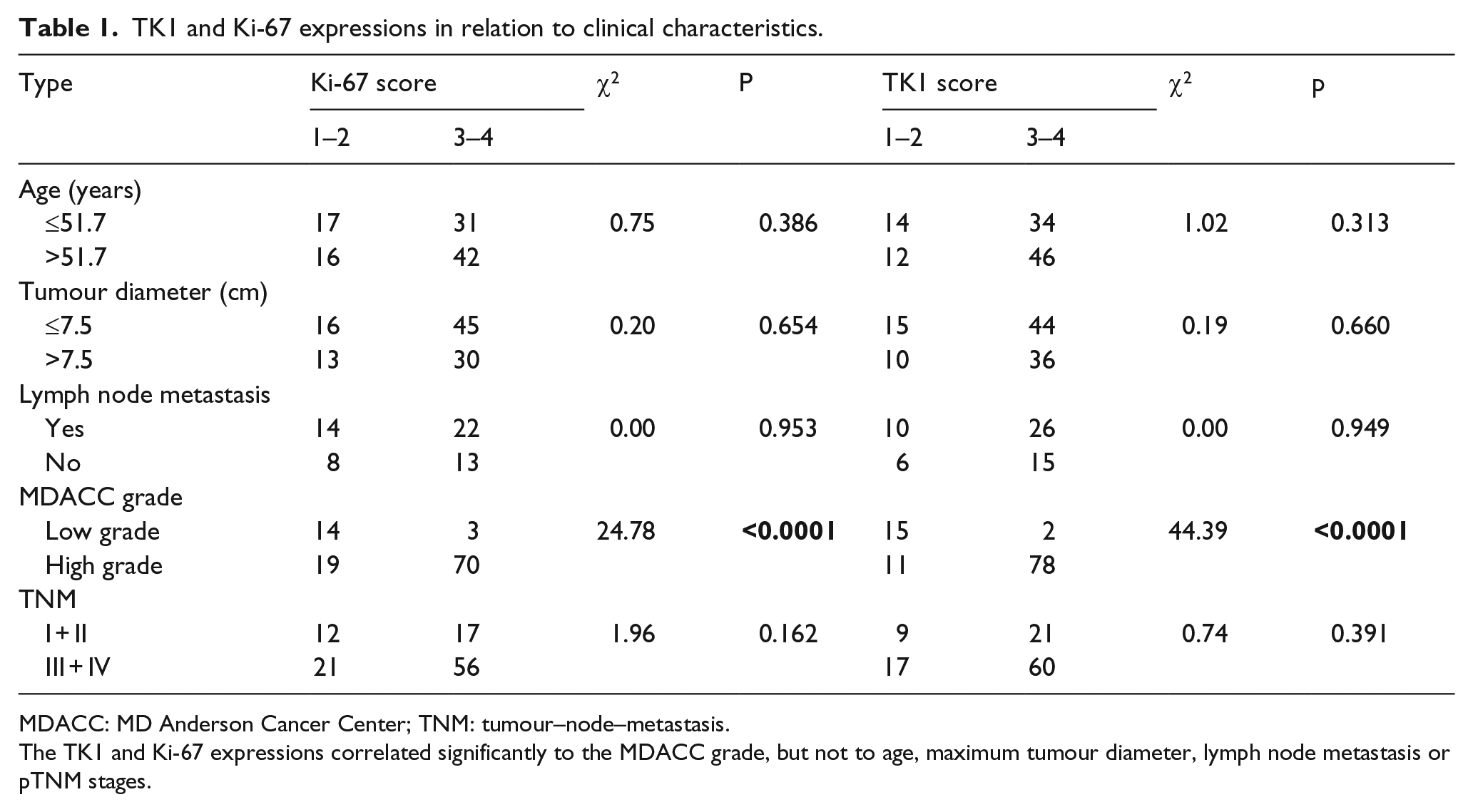
MDACC: MD Anderson Cancer Center; TNM: tumour–node–metastasis.
The TK1 and Ki-67 expressions correlated significantly to the MDACC grade, but not to age, maximum tumour diameter, lymph node metastasis or pTNM stages.
There was no correlation between TK1 expression and maximum tumour diameter (TK1: κ = 0.279, p = 0.034), nor between of TK1 and Ki-67 expressions and pTNM staging (TK1: κ = 0.222, p = 0.046; Ki-67: κ = 0.284, p = 0.022).
Prognosis
Relapse rate in relation to TK1, Ki-67 and clinicopathological features
Of 99 patients followed up, 74 patients showed relapse. The relapse incident rates in relation to TK1, Ki-67, MDACC grades, pTNM stages and lymph node metastasis are shown in Figure 2. Significant correlation between relapse and TK1 expression (p = 0.047), MDACC (p = 0.018), pTNM stages (p = 0.001) and regional lymph node metastasis (p < 0.001) were found, but not observed for Ki-67 (p = 0.314). The patients’ age, tumour location and maximum tumour diameter were not related to relapse (data not shown).

Relapse rates in relation to (a) TK1 expression, (b) Ki-67 expression, (c) MDACC grade, (d) pathological clinical stage TNM and (e) lymph node metastasis. The log-rank p values are given in the figures.
Overall survival rate in relation to TK1, Ki-67 and clinicopathological features
Of 107 patients followed up, 69 died after 3–173 months. The overall survival rate in relation to TK1, Ki-67, MDACC grades, pTNM stages and lymph node metastasis is shown in Figure 3. There were significant correlation between overall survival and TK1 expression (p = 0.021), MDACC (p = 0.014), pTNM stages (p = 0.001) and regional lymph node metastasis (p = 0.001), but no correlation with Ki-67 expression (p = 0.132). Patient’s age and tumour location and maximum tumour diameter were not related to overall survival (data not shown).

Overall survival rates in relation to (a) TK1 expression, (b) Ki-67 expression, (c) MDACC grade, (d) pathological clinical stage TNM and (e) lymph node metastasis. The log-rank p values are given in the figures.
Cox regression analysis
The univariate analysis showed statistically significant associations between relapse and TK1 expression (p = 0.05), MDACC grade (p = 0.023), pathological TNM stage (p = 0.001) and lymph node metastasis (p = 0.001); this was not observed for Ki-67 expression (p = 0.319) (Table 2). The analysis also showed statistically significant associations between overall survival and TK1 expression (p = 0.023), MDACC grade (p = 0.020), pathological TNM stage (p = 0.003) and regional lymph node metastasis (p = 0.001); an almost significant association with WHO stage (p = 0.0510); but no association with Ki-67 expression, tumour diameter or age (Table 3).
Characteristics of relapse by univariate and multivariate Cox regression analyses.

MDACC: MD Anderson Cancer Center; TNM: tumour–node–metastasis; CI: confidence interval; WHO: World Health Organization.
The univariate analysis and the multivariate analysis showed that TK1 expression was independent prognostic factors for relapse, but not observed for Ki-67.
Characteristics of overall survival by univariate and multivariate Cox regression analyses.
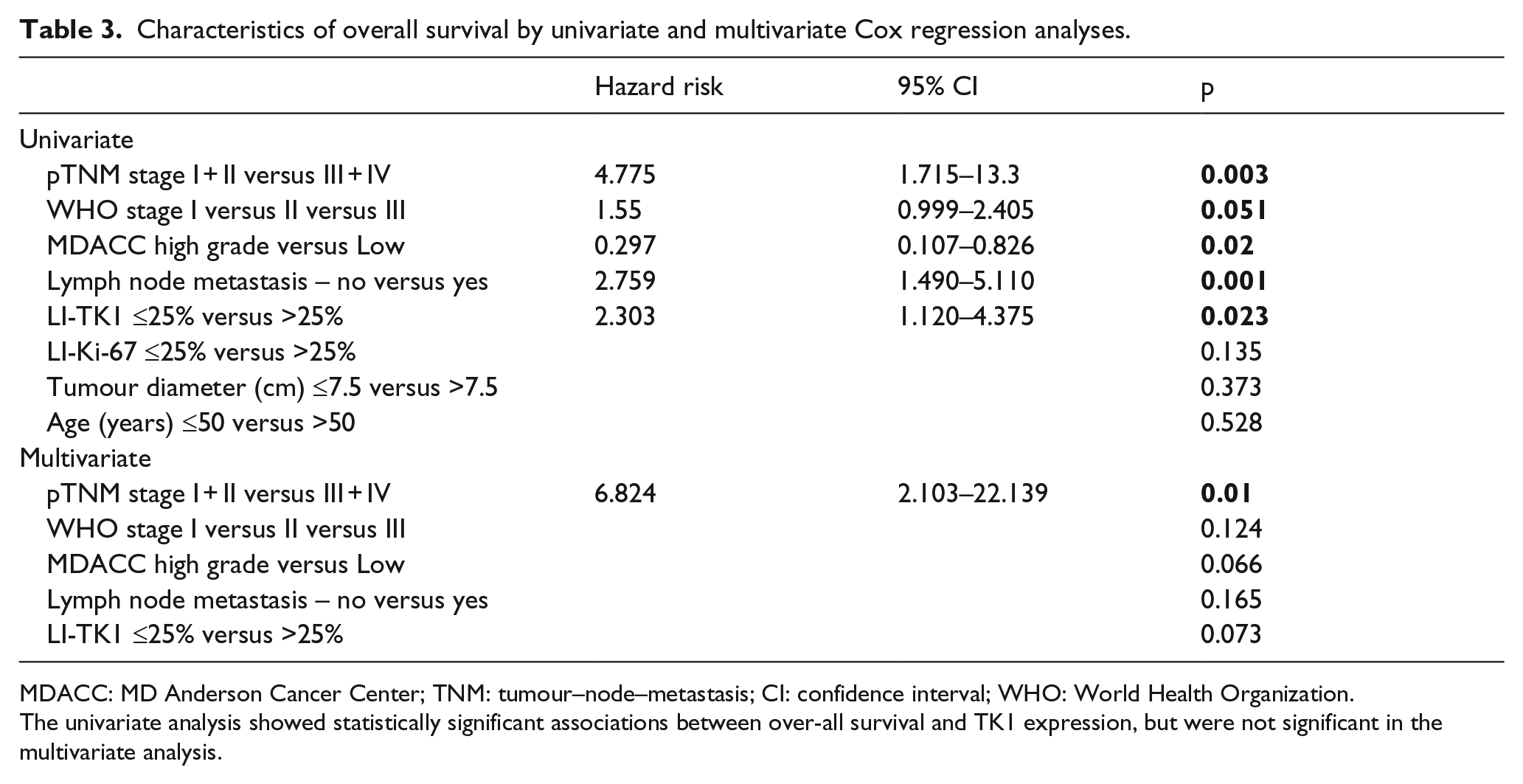
MDACC: MD Anderson Cancer Center; TNM: tumour–node–metastasis; CI: confidence interval; WHO: World Health Organization.
The univariate analysis showed statistically significant associations between over-all survival and TK1 expression, but were not significant in the multivariate analysis.
The multivariate analysis showed that only lymph node metastasis (p < 0.001) and TK1 expression (p = 0.021) were independent prognostic factors for relapse, while pTNM stage and MDACC grade were not (Table 2). In the multivariate analysis of survival, only the pTNM stage was an independent prognostic factor (p = 0.01), while WHO stage, MDACC grade, lymph node metastasis and TK1 expression were not (Table 3).
Discussion
Pathological TNM stage is the major diagnostic method for ovarian serous adenocarcinoma, and patients with high-grade serous carcinoma constitute 60%–80% of ovarian epithelial carcinomas.30,31 Although surgical techniques and chemotherapies have been developed, the prognosis remains poor, with a 5-year survival rate of 45%. Prognosis is more favourable in patients with stage I/II tumours; however, most patients are diagnosed with advanced-stage disease (stage III/IV).21,31 The number of pTNM stage III/IV patients in this study was 70.6%, the relapse rate was 74.7% and the death rate was 64.4%. Therefore, in our study, advanced stage and relapse were also important prognostic factors, resulting in treatment failure and death.
Although biomarkers for different subtypes of ovarian cancer are in use today, 12 only Wilms tumour gene 1 (WT-1) is considered as a relatively specific marker for the serous phenotype 32 and is a favourable prognostic biomarker for high-grade serous tumours. 12 Matrix metalloproteinase-7 (MMP-7) is an independent prognostic factor predicting longer survival in epithelial ovarian cancer. 33
The markers mentioned above might be associated with different natural histories of ovarian carcinoma subtypes, but they were not specific markers for tumour proliferation rates.
At present, decisions regarding surgery and adjuvant therapy are based mainly on tumour stage and grade rather than on ovarian carcinoma subtype; therefore, ovarian carcinomas have often been considered clinically as one disease. However, almost all high-grade tumours of serous epithelial ovarian cancers are bilateral and present in the advanced stages (stage III or IV). 5
Deficient regulation of tumour cell death and proliferation may result in unlimited proliferation leading to malignant tumour disease. In our study, the proliferation rate of ovarian serous adenocarcinoma cells was different in patients with different MDACC-grade tumours based on TK1 expression. When the tumour cell growth rate is high, there is an increased risk of metastatic disease leading to poor prognosis. Ki-67 is the most commonly used proliferation marker in oncology today. In a study on cultured dermal fibroblast proliferation, expression of Ki-67 and TK1 was determined during the cell cycle; the expression of TK1 in the G1 stage of the cell cycle was found to start hours before the onset of Ki-67 expression, 34 enabling the identification of a population of activated G1 cells with higher TK1 than Ki-67 expression. 34 In this study, although the LIs of TK1 and Ki-67 were similar (85.8% and 82.0%, respectively), TK1 expression correlated significantly with relapse and survival, while Ki-67 expression did not (Figures 2 and 3), supporting previous studies.17,19 Thus, TK1 is apparently a more sensitive prognostic biomarker than Ki-67 in ovarian serous adenocarcinoma.
Serum CA125 has been used in the diagnosis of all subtypes of ovarian carcinoma. CA125 levels were elevated in 80% of patients with advanced stage, and CA125 was expressed in 60% in patients with early stage. Cox analysis showed that pretreatment CA125 level is an independent predictor of progression-free survival in patients with advanced ovarian carcinoma. 35 Although TK1 expression was not an independent biomarker for survival in our study, TK1 expression was an independent prognostic marker for relapse of serious ovarian carcinoma. As we reported previously, serum TK1 is an independent predictor for risk of recurrence in breast carcinoma22,23 and for survival of breast carcinoma, 24 gastric carcinoma 25 and Hodgkin’s lymphoma. 26 A comparative study of serum TK1 and CA125 levels in patients with ovarian carcinomas seems therefore highly motivated and is now in progress.
Conclusion
TK1 showed a high correlation to relapse and survival, while Ki-67 did not. The new TK1 biomarker is therefore superior compared to Ki-67 for ovarian serous adenocarcinoma. TK1 combined with MDACC grade and pTNM stages might improve early prognosis in individual patients.
Footnotes
Acknowledgements
This study was made possible by the support of Nanjing Jinling Hospital, Nanjing University Medical School, China and Sino-Swed Molecular Bio-Medicine Research Institute, Shanghai, China and The International Development Cooperation Agency, Stockholm, Sweden and by a grant to S.E. from the Swedish Research Council. The anti-TK1 monoclonal antibody was supplied by SSTK Biotech., Inc., Shenzhen, China. J.W. and Q.L. have contributed equally to this work.
Consent
Informed consent was obtained from all individual participants included in the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.