
Abstract
Background
Immunotherapy has wholly changed how cancer is treated by using the body’s immune system to eliminate cancer cells. Cancer vaccines, chimeric antigen receptor T-cell (CAR-T) treatments, and immune checkpoint inhibitors (ICIs) are at the forefront, each with a unique method for boosting anti-tumor immunity. Despite its success, there are still issues with resistance mechanisms, limited effectiveness in some types of cancer, and optimizing combination treatments.
Purpose
The goal of this study is to give a comprehensive summary of the pharmacological approaches to cancer immunotherapy, such as cancer vaccines, CAR-T cell treatments, and ICIs. It overviews these treatments’ mechanics, clinical activity, ongoing clinical studies, difficulties, and potential prospects.
Materials and Methods
A thorough search of the available literature and clinical trial data was used to perform the narrative review. The study incorporated publications from several sources, including PubMed and clinical trial registries, to provide a current picture of the state of cancer immunotherapy. Critical therapeutic approaches were examined in light of new therapy paradigms, clinical findings, and molecular causes.
Results
ICIs, such as cytotoxic T-lymphocyte associated protein 4 (CTLA-4) and programmed cell death protein 1 (PD-1)/programmed death-ligand 1 (PD-L1) inhibitors, have shown promise, particularly in treating non-small-cell lung cancer (NSCLC) and melanoma. Trials are being conducted to assess the use of CAR-T cell therapy in solid tumors after it demonstrated efficacy in hematologic malignancies. The future is being transformed by cancer vaccinations, both preventative (like the human papillomavirus (HPV) vaccine) and therapeutic, with combination therapy showing promise in overcoming resistance and enhancing effectiveness.
Conclusion
ICIs, CAR-T cells, and cancer vaccines are driving the revolution in cancer immunotherapy. Even though the treatments offer much promise, additional research is needed to overcome the limitations of the present day, increase response rates, and expand their uses. Clinical trials and innovation will determine the future of cancer treatment.
Introduction
Cancer is still a leading cause of death worldwide, with 9.6 million deaths in 2018, as reported by the World Health Organization (WHO). Although traditional treatments such as surgery, chemotherapy, and radiotherapy have progressed a great deal, they are still far from being optimal in terms of efficacy, particularly in advanced and metastatic cancers. 1 Chemotherapy, as aggressive as it can be at times, is highly toxic to normal tissues, and adverse side effects such as loss of hair, gastrointestinal disturbances, and bone marrow suppression are encountered. Further, drug resistance continues to be a significant hindrance to the induction of long-term remission, particularly in advanced cancers. All these have led to the search to identify more specific and less toxic modes of treatment. Immunotherapy of cancer, which entails exploiting the body’s immune system to attack and destroy cancer cells specifically, has emerged as a leading contender. 2
Immunotherapy stimulates the immune system, in this instance, T-cells, natural killer cells, and macrophages, to recognize and kill cancer cells. This is in contrast to conventional approaches that target cancer cells specifically. 3 Immunotherapy aims to induce a long-lasting anti-cancer immune response. Although using the immune system to combat cancer was born in the early 20th century, it has picked up significantly recently. Of the numerous immunotherapeutic approaches that have been developed, immune checkpoint inhibitors (ICIs), chimeric antigen receptor T-cell (CAR-T) therapies, and cancer vaccines have been the most significant advances. 4
ICIs have revolutionized cancer therapy by targeting immune checkpoints that control immune responses and suppress hyperactivation. Tumors usurp these checkpoints, that is, programmed cell death protein 1 (PD-1)/programmed death-ligand 1 (PD-L1), and cytotoxic T-lymphocyte associated protein 4 (CTLA-4), to evade immune recognition. PD-1 and CTLA-4 are inhibitory regulators of T-cells, and their binding to ligands (PD-L1 and B7) suppresses T-cell function. 5 Tumors utilize PD-L1 to bind to PD-1 on T-cells, suppressing the immune response from targeting cancer cells. ICIs, such as nivolumab (PD-1 inhibitor), pembrolizumab (PD-1 inhibitor), and ipilimumab (CTLA-4 inhibitor), block these interactions and allow T-cells to remain activated and kill tumors. 6 These therapies have exhibited impressive clinical activity against melanoma, non-small-cell lung cancer (NSCLC), and bladder cancer. However, despite these promising results, the response rate remains suboptimal, with most patients not responding or relapsing after the initial response. These problems have led to investigations into combinatorial therapies and markers for selecting patients who would be more responsive. 7
CAR-T cell therapy has also been a historic success in and of itself, most notably in the case of the hematologic malignancies of B-cell lymphoma and acute lymphoblastic leukemia (ALL). CAR-T therapy involves genetically engineering a patient’s T-cells to produce chimeric antigen receptors (CARs) to recognize particular tumor antigens, such as CD19 on B-cells. 8 The engineered T-cells can bypass the immune suppression of the tumor and target and destroy cancer cells directly. CAR-T cell therapy has been shown to result in long-term remission in relapsed/refractory hematologic malignancies. The Food and Drug Administration (FDA) has also approved CAR-T therapies like Kymriah (tisagenlecleucel) and Yescarta (axicabtagene ciloleucel) for specific applications in some blood cancers. However, the extension of CAR-T cell therapy to solid tumors is daunting. 9 Solid tumors pose challenges like the tumor microenvironment (TME), which is immunosuppressive, and the compact architecture of the tumor that prevents CAR-T cell penetration. Current research strives to increase CAR-T cell persistence, enhance penetration through the tumor, and design combination strategies with ICIs to achieve their full potential in solid tumors. 10
Cancer vaccines, both preventive and therapeutic, also hold great promise. Preventive vaccines, like the human papillomavirus (HPV) vaccine, have been demonstrated to reduce the incidence of HPV-related cancer, that is, cervical cancer. Preventive vaccines accomplish this by vaccinating the immune system to recognize and destroy the virus so it never leads to cancer. 11 On the other hand, therapeutic cancer vaccines work to treat cancers by provoking an immune response to tumor-associated antigens. Therapeutic vaccines can be developed against antigens like HER2 in breast cancer or prostate-specific antigen (PSA) in prostate cancer. Therapeutic cancer vaccines, although with great promise, have not been as effective clinically as ICIs or CAR-T therapies, particularly in advanced-stage solid tumors. 12 Tumors are likely to evade immune detection, especially in advanced stages, which diminishes the efficacy of vaccines. To overcome this, scientists are in the process of developing personalized cancer vaccines, that is, vaccines that are customized to a patient’s tumor profile. Such vaccines can potentially increase immune responses by targeting specific mutations or antigens in the patient’s cancer. While much has been done in cancer immunotherapy, several challenges must be addressed to improve efficiency. 13
One of the most urgent issues is the complexity of the TME. The TME consists of numerous immunosuppressive cells, such as tumor-associated macrophages (TAMs), myeloid-derived suppressor cells (MDSCs), and regulatory T-cells (Tregs). These suppress immune responses to avert the effective operation of immunotherapies. 14 Tumor heterogeneity, where cancer cells from one tumor or between tumors from a single patient have different antigens, is also a challenge. This makes it impossible to formulate universal therapies, since some cancer cells are unlikely to respond to a single antigen-targeted therapy. Furthermore, resistance to immunotherapy is also rising as tumors evolve through mechanisms such as loss of tumor antigens or upregulation of alternative immune checkpoints. 15
Conquering these issues will require ongoing research into the crosstalk between the immune system and the tumor. Furthermore, treatments based on biomarkers will be needed to identify which patients will benefit from immunotherapy. Ongoing work in optimizing immunotherapy design, such as combination therapy and personalized therapy, will be required to conquer the issues. 16 Combination therapy, for example, ICIs with cancer vaccines or CAR-T therapy, is very promising for enhancing immune response and clinical outcomes. Even more promising is the future of cancer immunotherapy with personalized medicine, where the treatment is tailored to the personalized genetic and molecular profile of each patient’s tumor. This will allow for more targeted, effective, and less toxic therapy. 17
This narrative review presents an integrative and comprehensive overview of cancer immunotherapy’s three most advanced pharmacologic modalities: ICIs, CAR-T therapies, and cancer vaccines. Unlike previous reviews that usually report on a single modality or cancer type, this narrative synthesizes existing knowledge across modalities, focusing on clinical outcomes, mechanistic information, pharmacologic approach, and challenges such as the TME and resistance. Importantly, it emphasizes the comparative limitations and future promises of these modalities, especially in solid tumors, and the emerging trend of combination regimens and precision medicine. This integrative review will guide clinical practice and future research in an evolving field.
Review of Literature
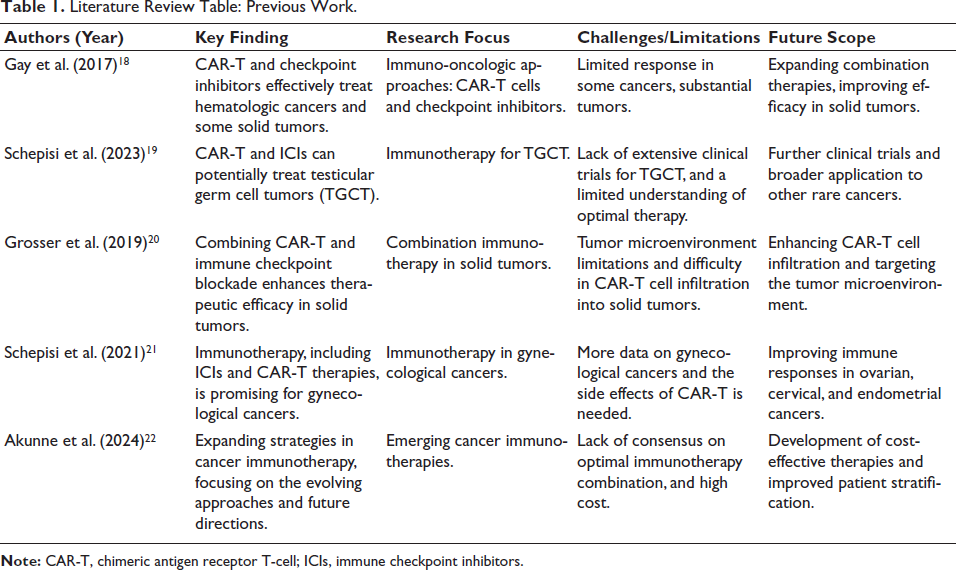
Recent research has pushed the boundaries of cancer immunotherapy, especially ICIs and CAR-T therapy. Gay et al. examined the performance of ICIs and CAR-T in tumor targeting, while Schepisi et al. revealed their promise in testicular germ cell tumors. Grosser et al. spoke of a synergistic combination of CAR-T with ICIs for solid tumors. Akunne et al. reviewed upcoming immunotherapeutic approaches, emphasizing how the cancer treatment landscape is changing.18–22
Table 1 is a comparative overview of major studies on CAR-T cell therapy and ICIs, including the key findings, therapeutic targets, current limitations, and proposed future developments in the evolving field of cancer immunotherapy.
Literature Review Table: Previous Work.
Methodology
Locating Data
Using the phrases “ICIs,” “CAR-T cell therapy,” and “cancer vaccines,” a thorough literature search was carried out across many databases, including PubMed, Scopus, and Google Scholar. Ongoing clinical studies and the reference lists of essential articles provided additional sources.
Data Collection
Relevant literature was considered, including observational studies, systematic reviews, and randomized controlled trials (RCTs). Included were peer-reviewed journal publications published between 2017 and 2024. Priority was given to inclusion in English-language publications with full-text accessibility.
Inclusion Criteria
The following were utilized: exclusively English-language, peer-reviewed articles from 2017 to 2024. Articles that included ICIs, CAR-T cell therapy, or cancer vaccines with clinical significance and full-text availability were selected.
Exclusion Criteria
Non-peer-reviewed articles, articles not written in English, case reports, editorials, and preclinical studies that were not relevant to clinical practice were excluded.
Limitations
As it was a narrative review, this study did not utilize a systematic protocol and thus possibly had selection bias. No formal quality measures of the study were utilized to judge validity, and the synthesis of findings was qualitative, not quantitative. Studying the heterogeneity of design, outcome, and publication bias makes generalizability unachievable. Therefore, conclusions drawn should be treated with the realization that cancer immunotherapy research is an evolutionary process.
Data Extraction
Information was taken from the included studies by two impartial reviewers. We collected data on primary outcomes, therapy strategies, sample size, reported difficulties, and research design. The reviewers’ disagreements were resolved by consensus and dialogue.
Integrating Data
A narrative synthesis approach was used to synthesize the findings of many studies. The advantages, disadvantages, and future promise of ICIs, CAR-T cell therapies, and cancer vaccines were contrasted and tabulated to identify the themes shared by all and the points of consensus.
Results
Efficacy and Clinical Outcomes of ICIs and CAR-T Cell Therapies
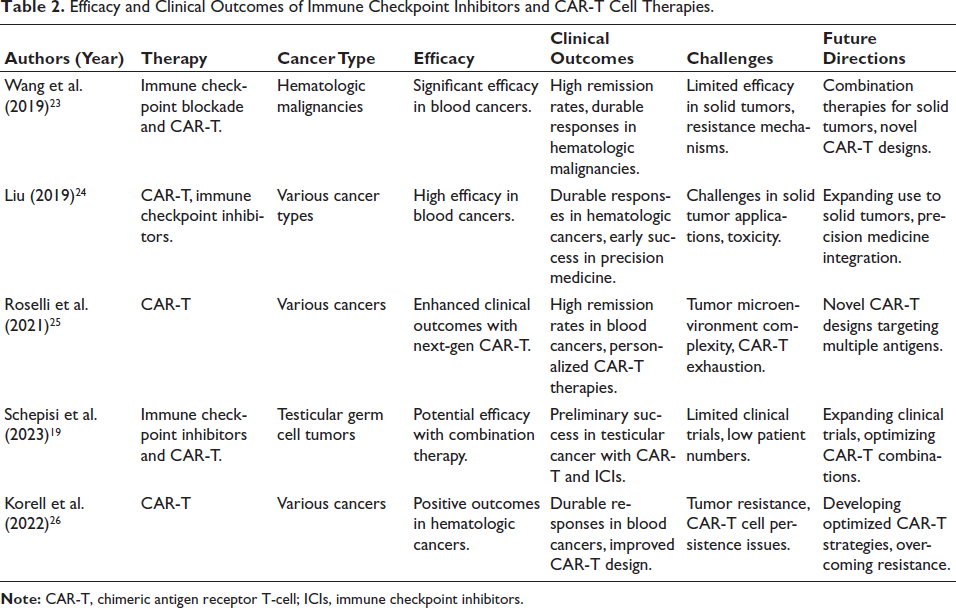
ICIs have effectively treated various cancers by blocking immune checkpoints such as PD-1/PD-L1 and CTLA-4 and restoring T-cell-mediated anti-tumor immune responses. 23 In melanoma, the advent of PD-1 inhibitors such as pembrolizumab and nivolumab has improved overall survival (OS) and progression-free survival (PFS). This has led to a relatively high percentage of patients with long-term responses. ICIs have also transformed the treatment of NSCLC by providing long-term survival benefits over traditional chemotherapy. ICIs have been proven to be effective in bladder cancer, with nivolumab and pembrolizumab approved for advanced disease, with impressive response rates and survival benefits. 24
CAR-T therapy has been remarkably effective in hematologic malignancies, particularly ALL and B-cell lymphoma. 25 CAR-T treatments, such as Kymriah (tisagenlecleucel) and Yescarta (axicabtagene ciloleucel), have been shown to have high remission rates and durable responses in relapsed or refractory patients. These therapies consist of gene-modifying a patient’s T-cells to target specific tumor antigens, such as CD19, and lead to the killing of cancer cells. 19 Although CAR-T cell therapies have been remarkably successful in blood cancers, their application in solid tumors is complex because of barriers like the TME and the difficulty in T-cell infiltration. However, clinical trials on the ongoing application of CAR-T cells in solid tumors show encouraging preliminary outcomes, particularly in cancers like glioblastoma and pancreatic cancer. 26 The findings are derived from Phase I to III RCTs data, real-world observational studies, and regulatory trial data.
Table 2 summarizes significant clinical outcomes of ICIs and CAR-T cell trials, such as their efficacy in various cancers, their respective clinical outcomes, therapy challenges, and directions in research to improve therapy, particularly in solid tumors.
Efficacy and Clinical Outcomes of Immune Checkpoint Inhibitors and CAR-T Cell Therapies.
Limitations and Challenges to the Use of CAR-T Cell Therapy
While CAR-T cell therapy has been highly effective in hematologic malignancies, its application in solid tumors presents several critical challenges. One of the significant challenges is immune evasion by solid tumors. 27 The tumor cells may employ several mechanisms to avoid immune recognition, such as downregulating antigen presentation or creating an immunosuppressive TME. These mechanisms disrupt the process of CAR-T cells recognizing and targeting tumor cells. 28 Another important constraint is the TME, which is generally immunosuppressive to immune cells. Solid tumors always have a corresponding TME with physical constraints like a dense extracellular matrix (ECM), the secretion of immunosuppressive cytokines, and regulatory immune cells like MDSCs and Tregs. CAR-T cell activity is inhibited, and their ability to infiltrate and survive in the tumor is impaired. 29
CAR-T cell persistence is also an issue in solid tumors. Unlike hematologic malignancies, where CAR-T cells have unrestricted circulation and can target tumor cells, the TME of solid tumors results in CAR-T cells being quickly exhausted or destroyed. This becomes a limitation to the therapeutic window and may result in tumor relapse. 30
Besides these biological concerns, side effects and toxicities are also of utmost concern. CAR-T cell therapy can lead to cytokine release syndrome (CRS), a frequently fatal syndrome that is indicative of systemic inflammation. Neurotoxicity is also an established complication, and the targeting of solid tumors compounds these toxicities. To overcome these complications, improved CAR-T cell infiltration, persistence, and specificity with fewer side effects are required. 31
In order to counter the difficulties of the TME of solid tumors, several novel strategies are under exploration to increase CAR-T cell infiltration, persistence, and efficacy. The TME, being immunosuppressive, contains regulatory cells like MDSCs, Tregs, and TAMs that inhibit CAR-T activity, whereas the dense ECM and hypoxia hinder cell penetration and survival. 32 To counter such limitations, scientists are engineering armored CAR-T cells that secrete cytokines, checkpoint-resistant variants, enzyme-secreting constructs, and bispecific CARs. Combination regimens and metabolic reprogramming are also being explored. Such approaches aim to augment CAR-T function and extend their success to solid tumors from hematologic malignancies. 33
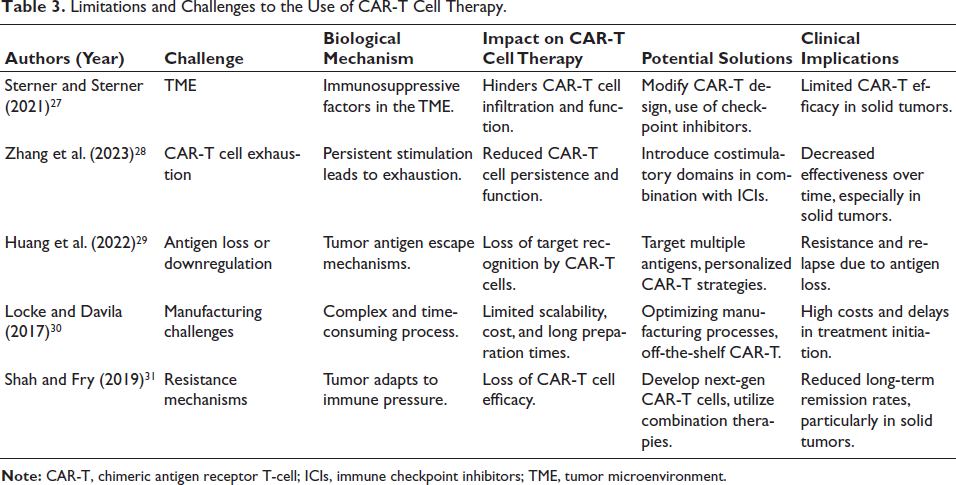
Table 3 outlines key CAR-T cell therapy limitations in solid tumors. It outlines the underlying biological rationale of each limitation, its impact on therapy, the proposed solutions to avoid such limitations, and the resulting clinical implications for patient treatment and treatment scalability.
Limitations and Challenges to the Use of CAR-T Cell Therapy.
Safety and Toxicity Profiles of Immunotherapies
CAR-T cell and ICI therapies have yielded unprecedented clinical responses, but at the expense of many adverse effects and toxicities. In ICIs, immunotherapy-related adverse events (irAEs) are the most common side effects to arise due to the triggering of immune responses against self-tissues. 34 These may be present in various organs, including the skin (rash), gastrointestinal tract (colitis), liver (hepatitis), and endocrine glands (adrenalitis or hypothyroidism). IrAEs may range from mild to life-threatening and thus need to be closely monitored and, at times, treated with corticosteroids or immunosuppressive agents for symptom control. 35
The two essential toxicities of CAR-T therapy are CRS and neurotoxicity. CRS occurs due to the release of enormous amounts of cytokines by CAR-T cells into the circulation following systemic inflammation, fever, and organ dysfunction. Severe CRS can cause multi-organ failure. 36 Neurotoxicity (e.g., encephalopathy, seizures, and delirium) has been reported, particularly in patients treated with CAR-T therapy for hematologic malignancies. Management of CRS is typically in the form of tocilizumab (IL-6 receptor antagonist), whereas neurotoxicity can be managed with supportive therapy and CAR-T therapy discontinuation. Management of these toxicities includes cautious monitoring, early recognition, and immediate treatment to minimize the risks and optimize patient results. The published toxicity profiles are mostly from clinical trials (Phase I–III), post-marketing surveillance, and real-world treatment cohorts, where adverse event monitoring is uniform. 37
Biomarkers and Personalized Approaches to Cancer Immunotherapy
Biomarkers are at the forefront of predicting the outcome of cancer immunotherapies, including ICIs and CAR-T cell therapy. One of the most widely used biomarkers is PD-L1 expression, which is used to choose between patients likely to benefit from PD-1/PD-L1 inhibitors because increased PD-L1 expression on tumor cells is predictive of increased response to ICIs. 38 Tumor mutational burden (TMB) is another critical biomarker. Increased TMB is associated with an increased response to ICIs due to the increased possibility of the presentation of neoantigens and, thus, increased immune recognition of cancer cells. Microsatellite instability (MSI), in the case of tumors like colorectal cancer, is another response predictor because high MSI tumors have enhanced sensitivity to ICIs. 39
The field of personalized immunotherapy is evolving rapidly, with therapies tailored to the patient’s unique molecular and genetic signature of the tumor. Personalized cancer vaccines are engineered to induce an immune response against tumor-specific antigens. CAR-T cell therapies can be designed to target unique tumor antigens expressed in an individual patient’s tumor profile. 40 This approach promises more efficient and more precise therapies. The application of genomic profiling in the clinic allows for the identification of actionable mutations and, thus, the development of individualized treatment regimens that maximize therapeutic benefit with minimal adverse effects. This biomarker and personalized therapy function is supported by evidence derived from genomic profiling reports, biomarker-directed clinical trials, and retrospective treatment efficacy and optimization studies. 41
Long-term Effectiveness, Relapse Rates, and Future Implications
The long-term effectiveness of ICIs and CAR-T cell therapy has been highly promising, most prominently in cancers like melanoma, NSCLC, and certain hematologic malignancies. 42 For ICIs, the long-term duration of response is a significant strength, with certain patients maintaining long-term remission even after treatment has been stopped. Relapse remains a problem, most prominently in lower immunogenicity cancers or patients with poorer biomarker profiles. For instance, although PD-1 inhibitors have revolutionized survival in melanoma, about 40% of patients recur, most typically through mechanisms of immune evasion or secondary resistance. 43
CAR-T cell therapies have also succeeded, particularly in hematologic malignancies such as B-cell lymphoma and ALL. Clinical trials have reported high remission rates, with some remission for decades. Relapse in patients treated with CAR-T, particularly in solid tumors, is still high. 44 Tumor heterogeneity, T-cell exhaustion, and the immunosuppressive TME are some of the challenges responsible for the failure of long-term responses in such patients. These findings are corroborated by extended follow-up of Phase II/III trials, post-marketing surveillance, and a real-world registry study of relapse occurrence and survival in chronic lymphocytic leukemia (CLL) patients. 45
The future of immunotherapy is combination regimens, which will maximize efficacy and avoid resistance mechanisms. Combining ICIs with CAR-T therapy, targeted therapies, or oncolytic viruses has been promising in initial trials to boost immune responses and minimize relapse rates. Emerging technologies like personalized cancer vaccines, gene editing technologies (e.g., clustered regularly interspaced short palindromic repeats (CRISPR)), and bispecific antibodies are also being investigated to increase the specificity and persistence of immunotherapies. Overcoming present limitations, mainly resistance and toxicity, will be crucial to maximizing the long-term efficacy of these therapies. 46
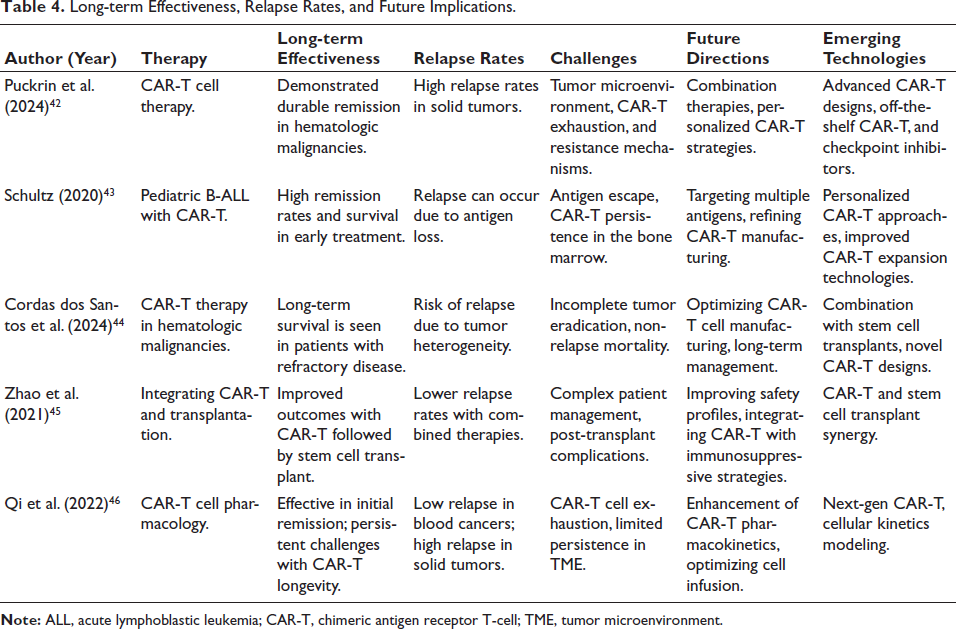
Table 4 presents key findings on the long-term effectiveness of CAR-T cell therapy, highlighting remission durability, relapse patterns, and associated challenges. It also outlines future directions and emerging technologies to enhance CAR-T performance and clinical outcomes.
Long-term Effectiveness, Relapse Rates, and Future Implications.
Discussion
Cancer immunotherapy has transformed cancer treatment by leveraging the body’s immune system to destroy cancer cells. ICIs, CAR-T therapies, and cancer vaccines represent some of the most significant advances. These therapies have delivered meaningful clinical responses across many cancers, yet are tumor type, immunocompetence, and patient-specific. 47
ICIs: Achievements and Limitations
ICIs have transformed the management of several solid tumors. By blocking inhibitory receptors such as PD-1, PD-L1, and CTLA-4, ICIs restore T-cell functions, leading to tumor regression. Their effectiveness is proven in melanoma, NSCLC, and bladder cancer, improving OS and durable remissions in patients. However, the success of ICIs is greatly influenced by tumor immunogenicity. 48 Favorable response rates occur in high mutational burden or neoantigen load tumors. Tumors like glioblastoma, pancreatic cancer, and some sarcomas are more likely to have a poor response with immune exclusion, low antigen presentation, or by an immunosuppressive TME. In addition, durable benefit occurs in a minority of patients with solid tumors, whereas the majority develop resistance or relapse in the long term. 49
Immunotherapy-related adverse events (irAEs) remain a significant limitation. These toxicities, ranging from mild cutaneous eruptions to severe autoimmune assaults in endocrine glands, lungs, or liver, tend to necessitate immunosuppressive treatment. Even though these treatments manage toxicity, they can also compromise the therapeutic activity of ICIs, and thus make it even more indispensable to have improved risk stratification and biomarker-driven selection. 50
CAR-T Cell Therapy: Beyond Hematologic Cancers
CAR-T cell therapy has historically been successful in hematologic malignancies, most notably B-cell lymphomas and ALL. The treatment allows for direct killing of tumor cells through the process of a patient’s T-cells being engineered to carry tumor-targeting receptors like anti-CD19 CARs. FDA-approved therapies, like Kymriah and Yescarta, have achieved durable remissions in refractory disease, making CAR-T a curative therapy for select blood cancers. 51
However, extrapolating this success to solid tumors is daunting. The immunoinhibitory and fibrotic TME restrict CAR-T cell trafficking and function. T-cells, MDSCs, and immunosuppressive cytokines such as TGF-β all contribute to resistance, and physical barriers in the form of a dense ECM hinder cell trafficking. Antigen heterogeneity and loss, T-cell exhaustion, and limited persistence all further compromise therapeutic efficacy in solid tumors. 52
Toxicities such as CRS and immune effector cell-associated neurotoxicity syndrome (ICANS) are also still significant issues. CRS is a systemic inflammatory response secondary to diffuse cytokine release, whereas ICANS is central nervous system involvement and can manifest as confusion, seizures, or encephalopathy. It is managed with careful monitoring and directed treatments such as tocilizumab or corticosteroids, which must be carefully titrated to maintain the efficacy of the treatment. 53
To address such challenges, several new strategies are on the horizon. Armed CAR-T cells, that secrete pro-inflammatory cytokines, can be employed to reprogram the TME. Bispecific CARs and checkpoint resistance-inducing constructs (e.g., PD-1 knockout) are being explored. 54 Enzyme-expressing CAR-T cells can be engineered to degrade ECM barriers to penetrate deeper, and combination regimens with ICIs or oncolytic viruses attempt to synergize with immune activation. Such modalities are promising in early-phase trials and represent a method to improve CAR-T outcomes in solid tumors. 55
Cancer Vaccines: Future Scope and Personalization
Cancer vaccines are an alternative form of immunotherapy to prevent or cure malignancies. Preventive vaccines, such as those against HPV, have been successful in cervical cancer prevention. Therapeutic cancer vaccines aim to generate T-cell responses against tumor-associated antigens in established malignancies. The clinical benefit is at best modest, particularly in advanced-stage solid cancers. 56
One of the significant obstacles to the success of therapeutic vaccines is immune evasion by tumors. Individualized cancer vaccines, built from genomic profiling of patient-specific tumor mutations, are a new strategy for overcoming this. The vaccines are designed to trigger a precise immune response and are now being assessed in early clinical trials. 57
The Biomarker and Precision Medicine Role
Biomarkers are equally critical in identifying patients with a high likelihood of response to immunotherapy. PD-L1 expression, TMB, and MSI are already utilized to identify ICI therapy. High PD-L1 expression and TMB correlate with high response rates to ICIs, and MSI-high status predicts response in colorectal and endometrial cancer. 58
The advent of personalized immunotherapy, informed by genomic and transcriptomic analysis, is transforming cancer therapy. This approach enables the personalization of therapy to immune and tumor-mutation profiles. CAR-T cell engineering and vaccine manufacturing are also informed by it, optimizing specificity and reducing off-target toxicity. The translation of these technologies into the clinic can lead to individualized and enhanced treatment regimens. 59
Future Horizons and Emerging Technologies
Combination strategies are an early focus. A combination of ICIs and CAR-T therapies, cancer vaccines, or targeted drugs is being tested in ongoing phase trials. Combinations aim to overcome resistance, enhance the immune response, and expand the number of cancers that can be treated. Off-the-shelf CAR-T products, CRISPR-engineered immune cells, and new delivery systems represent other emerging technologies that have the potential to improve scalability and reduce costs. 60 Despite the present setbacks, cancer immunotherapy is still among the most exciting advances in oncology. With the unabated stream of innovations in cellular engineering, biomarker incorporation, and combination regimens, the specialty is inching closer to overcoming its present limitations. 61 Further research and fine-tuning are essential to bring immunotherapy’s full potential to bear in durable, low-toxicity forms for a broader range of cancers. New technologies, including CRISPR-edited CAR-T cells, bispecific T-cell engagers (BiTEs), and patient-specific neoantigen vaccines, are also being investigated in early-phase clinical trials, with initial indications of enhanced persistence, diminished relapse, and enhanced targeting of the tumor. 62
Conclusion
Cancer immunotherapy, such as ICIs, CAR-T therapy, and cancer vaccines, has transformed the face of cancer treatment. These are targeted and potent alternatives to conventional treatments such as chemotherapy and radiotherapy, some of which induce long-lasting responses, especially in cancers such as melanoma, non-small-cell lung carcinoma, and B-cell lymphoma. However, for all their success, issues remain. ICIs exhibit poor response rates in specific cancers. CAR-T cell therapy is also faced with solid tumor resistance through TME challenges, immune evasion, and the persistence of CAR-T cells. In addition, the threat of side effects such as immune-related toxicities and CRS has to be treated cautiously. The future of cancer immunotherapy is to overcome these limitations with combination therapies and personalized medicine. Continued research in amplifying the effects of these therapies, augmenting patient selection through biomarkers, and optimizing immunotherapeutic approaches will be essential in overcoming current limitations. As the science develops, more targeted, less toxic therapies will improve patient outcomes, placing immunotherapy at the center of cancer treatment. Through ongoing innovation, cancer immunotherapy can lead to durable, life-prolonging therapies for more patients and cancers.
Key Takeaways
Cancer immunotherapy, including ICIs, CAR-T cell therapy, and cancer vaccines, has transformed cancer therapy by harnessing the immune system against tumor cells. While ICIs have been spectacularly effective in most cancers, poor response rates, toxicity, and resistance mechanisms have been encountered. CAR-T cell therapy has been spectacularly effective in hematologic malignancies. However, it faces challenges in solid tumors, including the intricacies of the TME and the persistence of CAR-T cells. Personalized approaches and combination therapies will be key to achieving maximum therapeutic efficacy and addressing these challenges. Future advancements in advanced biomarkers, patient selection, and new therapies will determine the future of cancer immunotherapies, with the hope of effective, sustained, and less toxic therapy.
Footnotes
Abbreviations
ALL: Acute lymphoblastic leukemia; BiTEs: Bispecific T-cell engagers; CAR: Chimeric antigen receptor; CAR-T: Chimeric antigen receptor T-cell; CRISPR: Clustered regularly interspaced short palindromic repeats; CRS: Cytokine release syndrome; CTLA-4: Cytotoxic T-lymphocyte associated protein 4; ECM: Extracellular matrix; FDA: Food and Drug Administration; HPV: Human papillomavirus; ICANS: Immune effector cell-associated neurotoxicity syndrome; ICIs: Immune checkpoint inhibitors; irAEs: Immune-related adverse events; MDSCs: Myeloid-derived suppressor cells; MSI: Microsatellite instability; NSCLC: Non-small-cell lung cancer; OS: Overall survival; PD-1: Programmed cell death protein 1; PD-L1: Programmed death-ligand 1; PFS: Progression-free survival; PSA: Prostate-specific antigen; RCTs: Randomized controlled trials; TAMs: Tumor-associated macrophages; TGCT: Testicular germ cell tumors; TGF-β: Transforming growth factor beta; TMB: Tumor mutational burden; TME: Tumor microenvironment; Tregs: Regulatory T-cells; WHO: World Health Organization.
Acknowledgments
The authors want to thank clinicians and scientists working on the research discussed in this manuscript for their efforts. Their continued work in cancer immunotherapy is crucial to determining how cancer therapy progresses.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
All the quoted studies and clinical trials were conducted in line with ethical standards by Institutional Review Boards and ethics committees. All the participants in the quoted studies gave informed consent in compliance with the Declaration of Helsinki.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.