
Abstract
Background
Chronic respiratory diseases (CRDs) significantly impact patients’ quality-of-life (QoL), necessitating effective interventions for symptom management and functional improvement. Pulmonary rehabilitation (PR) has emerged as a potential therapeutic approach; yet, comprehensive analyses comparing multiple QoL metrics remain limited. This study evaluated the effectiveness of PR by analyzing three validated assessment tools: the 36-Item Short Form Health Survey (SF-36), St. George’s Respiratory Questionnaire (SGRQ), and the University of California, San Diego Shortness of Breath Questionnaire (USCD-SOBQ).
Materials and Methods
A prospective study was conducted with 115 patients diagnosed with chronic respiratory conditions, including chronic obstructive pulmonary disease (COPD) (40%), interstitial lung disease (ILD) (34.78%), and asthma (25.22%). The study population predominantly comprised females (77.39%) with a mean age of 53.83 ± 10.2 years. QoL was assessed using SF-36, SGRQ, and Shortness of Breath Questionnaire (SOBQ) measures before and after PR. Statistical analysis included Wilcoxon signed-rank tests for pre-post comparisons and correlation analyses between different measurement tools.
Results
Significant improvements were observed across multiple QoL metrics post-rehabilitation. SGRQ scores showed substantial improvements across all domains (p < .001), with total scores decreasing from a median of 92 (IQR ± 14) to 63 (IQR ± 57). SF-36 demonstrated significant enhancements (p < .002), particularly in physical functioning (from 13 ± 9 to 20 ± 12) and role physical domains. SOBQ scores improved significantly from 79 ± 25 to 67 ± 36 (p < .001). Strong correlations were observed between all three assessment tools (ρ = 0.62–0.66, p < .001), validating their concurrent utility in measuring rehabilitation outcomes.
Conclusion
This study demonstrates that PR significantly improves the QoL in patients with CRDs across multiple validated assessment measures. The strong correlations between the SF-36, SGRQ, and SOBQ suggest these tools provide complementary insights into rehabilitation outcomes. These findings support the effectiveness of PR programs and validate the use of multiple assessment tools in monitoring patient progress.
Keywords
Introduction
Chronic respiratory diseases (CRDs) create a major worldwide healthcare problem because they produce extensive illness and death statistics. 1 The three conditions of chronic obstructive pulmonary disease (COPD), along with asthma and interstitial lung diseases (ILDs), produce progressive airflow blockage and dyspnea symptoms, which decrease patient quality-of-life (QoL). 2 Pulmonary rehabilitation (PR) functions as the leading therapeutic approach for CRDs because it addresses symptoms and builds exercise abilities, together with improving patients’ QoL. 3 The documented advantages of PR exist, but researchers need to examine different QoL assessment tools more thoroughly. 4 Millions of people worldwide experience CRDs, and COPD stands as the third most fatal condition worldwide. 5 According to the Global Burden of Disease Study, the prevalence of COPD keeps increasing because populations are aging, and exposure to smoking and air pollution is increasing. 6 Asthma affects more than 300 million global patients who need hospital care and generates high healthcare expenses. 7 When it comes to ILDs, the healthcare challenge increases due to diagnostic difficulties and treatment complexities, which reinforces the requirement for extensive rehabilitation approaches. 8 Combining educational and therapeutic components from multiple fields of expertise makes up the PR program for CRD patients. 9 The program combines exercise training with patient education and behavior intervention programs that match specific patient requirements. 10 Research shows that PR treatments successfully minimize shortness of breath symptoms and boost exercise capabilities while cutting down hospitalization rates. 11 The physiological changes in the body enable better respiratory function, oxygen delivery, and more efficient muscle operation. 12
The assessment of PR effectiveness demands measurement instruments that properly measure both patient-perceived and measurable outcomes. Three widely used instruments for QoL assessment are the 36-Item Short Form Health Survey (SF-36), the St. George’s Respiratory Questionnaire (SGRQ), and the Shortness of Breath Questionnaire (SOBQ). General health status is measured through the SF-36, but the SGRQ targets respiratory diseases exclusively, and the SOBQ specifically examines dyspnea intensity. The relationship between these evaluation tools needs to be completely comprehended to achieve optimal patient results and develop personalized rehabilitation strategies. Research has shown that rehabilitation through PR generates meaningful QoL improvements through all assessment methods, but each tool demonstrates different levels of responsiveness. The SF-36 instrument provides general health status information, SGRQ delivers disease-specific evaluation, and SOBQ specifically measures breathlessness. Multiple studies have shown that these QoL measurement tools are compatible, but their different sensitivity levels call for a comparative evaluation process. The established role of PR in CRD management exists, but researchers still need to understand how different QoL measurement tools are connected and affect patient-reported results. The evaluation of validity and reliability, along with clinical utility for SF-36, SGRQ, and SOBQ becomes possible through their comparative assessment. The research seeks to improve PR outcome assessment through relationship identification, which will guide evidence-based rehabilitation decisions. PR improves QoL and symptoms in CRDs, primarily studied in COPD. However, data comparing outcomes across diverse conditions (COPD, ILD, asthma) using validated tools like the SGRQ, SF 36, and SOBQ are limited. Disease-specific pathophysiology may influence responsiveness, necessitating tailored approaches. This study addresses these gaps by evaluating rehabilitation outcomes in a multi-diagnostic cohort to inform personalized treatment.
Objectives
PR has been used to determine its effect on the QoL as measured by validated (SF-36, SGRQ, and SOBQ) assessment tools in patients with CRD, but there are no absolute data on the degree of improvement achieved post-rehabilitation. The purpose of this study is to compare the effectiveness and interrelationship of SF-36, SGRQ, and SOBQ in QoL changes in patients undergoing PR.
Materials and Methods
Study Design
A prospective interventional study was conducted at Sparsh Chest Diseases Center, Ahmedabad, to evaluate the impact of PR on QoL metrics among 115 patients with CRDs. The study employed three validated assessment tools (SF-36, SGRQ, and SOBQ) pre- and post-rehabilitation, with correlation analyses to determine the relative effectiveness and relationships between these measurement instruments.
Participants and Sampling Method
A consecutive sampling method was employed at Sparsh Chest Diseases Center, where 320 patients with CRDs were initially screened. Following the application of inclusion and exclusion criteria, 205 patients were excluded, resulting in a final sample of 115 stable patients who had consented to participate. All enrolled patients underwent a 3-month PR program with pre- and post-intervention assessments.
Intervention
The PR program included exercise training, respiratory therapy, and patient education. The program was 8 weeks in duration, with supervised training sessions every 2 weeks, that included endurance, strength, and breathing techniques.
Data Collection Tools
Before and after rehabilitation, three validated questionnaires (SF-36, SGRQ, and SOBQ) were administered. General health-related QoL was measured by the SF-36, respiratory-specific impairment by the SGRQ, and breathlessness severity by the SOBQ. The SF-36, together with the SGRQ and the SOBQ, evaluated the QoL in patients with CRDs. SF-36 assessed general health status through its measurements, while SGRQ evaluated disease-specific impairment, and SOBQ quantified breathlessness severity. The SF-36 scores operated between 0 and 100 points, with superior health levels corresponding to increased scores. The SGRQ assessment yielded scores between 0 and 100 points, and better respiratory health corresponded to lower scores. The range of SOBQ scores extended from 0 to 100, while lower scores on this scale indicated reduced breathlessness. Multiple assessment instruments gave an in-depth evaluation of PR success.
Pulmonary Rehabilitation (PR)
The PR program was conducted over an 8-week period and consisted of three supervised sessions per week, totaling 24 sessions. Each session included aerobic training lasting 30 min at an intensity of 60%–70% of the participant’s peak heart rate. In addition, resistance exercises targeting both upper and lower limbs were performed, comprising two sets of 10 repetitions each. Furthermore, the program included weekly 45 min educational sessions focusing on topics such as energy conservation techniques and proper medication use. To ensure consistency and standardization across all participants, every session was conducted by certified respiratory therapists following pre-loaded exercise protocols on hospital equipment.
Statistical Analysis Methods
Statistical analysis was performed using Statistical Package for the Social Sciences (SPSS) software. The Wilcoxon signed-rank test was used to compare pre- and post-rehabilitation outcomes across SF-36, SGRQ, and SOBQ measures. Spearman’s correlation coefficient (ρ) was calculated to assess relationships between the three QoL measurement tools. Multivariate analysis was also carried out. Missing data were minimal (<2%) and were handled using complete-case analysis, including only participants with complete pre- and post-intervention assessments for SF-36, SGRQ, and SOBQ. No imputation methods were applied due to the low rate of missingness. Statistical significance was set at p < .05 for all analyses.
Results
Of the 320 patients screened, 205 (64.06%) were excluded due to non-attendance for therapy sessions during the screening phase. The remaining 115 patients were enrolled, all of whom completed the 8-week PR program and provided pre- and post-intervention assessments. No dropouts occurred post-enrollment, and analyses were based on the full sample of 115 participants.
Demographic and Clinical Profile of Participants
A total of 115 participants took part in the study, where 89 (77.39%) identified as female and 26 (22.61%) identified as male. The research participants averaged 53.83 years of age, with a standard deviation of 10.2 years. The study participants ranged between 30 years old and above 71 years old with the following distribution: 14 (12.17%) were between 31 and 40 years old, 23 (20.00%) were aged between 41 and 50 years old, and 52 (45.22%) were within the 51–60 age group. The study participants included 24 individuals (20.87%) who were between 61 and 70 years old, together with two participants (1.74%) who were above 71 years old. The research participants showed an average body mass index (BMI) value of 26.59 ± 4.51, as shown in Table 1. The results showed one participant with an underweight status (<18.5) and 39 participants with a healthy BMI (18.5–24.9) among the total participants. A baseline analysis of patient characteristics was conducted to understand the patients’ situation before PR started.
Baseline Demographics and Clinical Characteristics.
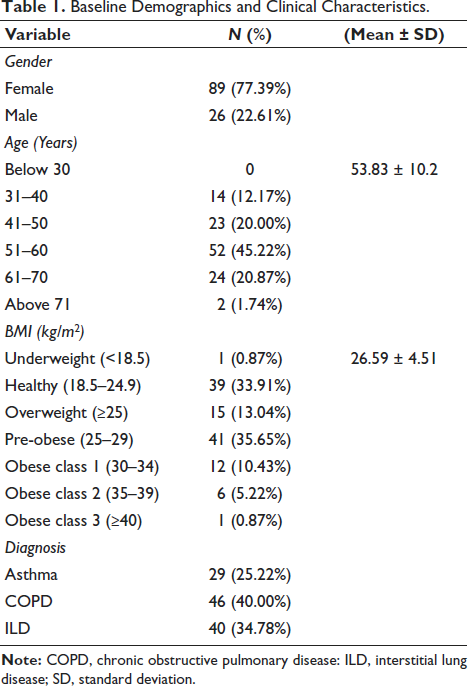
Table 2 illustrates the impact of PR on patient outcomes by comparing pre- and post-intervention measures using the SGRQ, SF-36, and the University of California, San Diego Shortness of Breath Questionnaire (USCD-SOBQ) scores. Significant improvements (p values < .05) are observed across various domains, highlighting the effectiveness of rehabilitation. For the SGRQ, substantial reductions are recorded in symptom burden (84 to 52), activity limitation (100 to 77), impacts (91 to 57), and the total score (92 to 63), reflecting an enhanced overall respiratory-related QoL. Similarly, in the SF-36 domains, physical functioning (13–20) and role physical (4–6) demonstrate meaningful gains, though some areas, such as general health, vitality, and mental health, remain unchanged. Notably, the USCD-SOBQ score improves from 79 to 67, indicating reduced dyspnea. The Wilcoxon signed-rank test confirms the statistical significance of these changes (p < .05), affirming the positive effect of rehabilitation.
Pre- and Post-rehabilitation Outcomes (Median ± IQR)
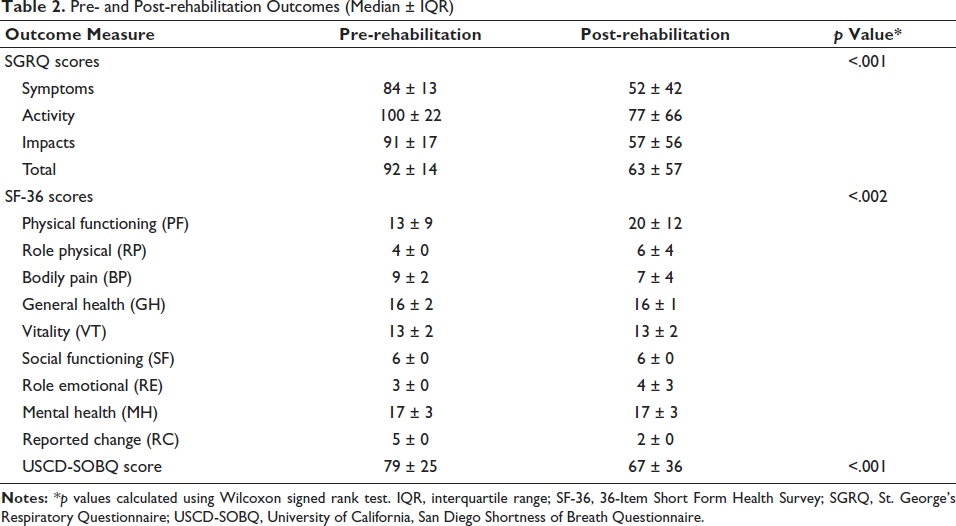
Table 3 presents the correlation between three key QoL assessment tools: SF-36, SGRQ, and SOBQ. Each pairwise comparison reveals a strong positive correlation, with coefficients (ρ) ranging from 0.62 to 0.66 and p values below .001, signifying statistically significant relationships. The SF-36 and SOBQ show a correlation of 0.65, suggesting that improvements in physical and mental health align with reductions in dyspnea. Similarly, the SGRQ and SOBQ exhibit a correlation of 0.66, reinforcing the link between respiratory symptom relief and reduced breathlessness. The SF-36 and SGRQ correlation (0.62) indicates that enhanced general health and well-being correspond with a lower respiratory disease impact. These findings highlight the interconnected nature of QoL domains and suggest that improvements in one area (e.g., symptom relief) are closely tied to better physical functioning and reduced breathlessness, supporting the comprehensive benefits of PR.
Correlation Matrix Between Quality-of-life Measures.
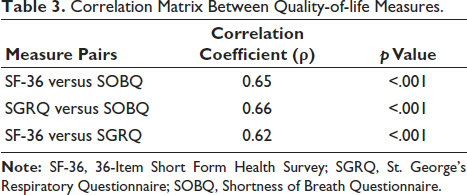
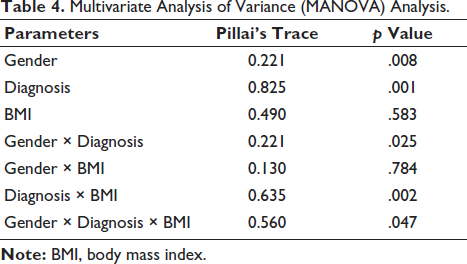
Table 4 presents that gender has a statistically significant multivariate effect on the dependent variables. Diagnosis also has a highly significant multivariate effect, indicating that the type of diagnosis (asthma, COPD, and ILD) strongly influences the outcomes across all dependent variables. BMI does not have a significant multivariate effect on the dependent variables. The interaction between gender and diagnosis is statistically significant, suggesting that the combined effect of these factors impacts the dependent variables. No significant interaction effect between gender and BMI was observed. The interaction between diagnosis and BMI is significant, indicating that BMI modifies the effects of diagnosis on the dependent variables. The three-way interaction among gender, diagnosis, and BMI is statistically significant at the multivariate level.
Multivariate Analysis of Variance (MANOVA) Analysis.
To assess the clinical relevance of the observed changes, improvements in SGRQ, SF-36, and SOBQ scores were compared to established minimal clinically important difference (MCID) thresholds. The SGRQ total score decreased by a median of 29 points (from 92 ± 14 to 63 ± 57), exceeding the MCID of 4 points. 13 For SF-36, the physical functioning domain improved by a median of seven points (from 13 ± 9 to 20 ± 12), surpassing the MCID of five points for this domain. 14 The SOBQ score improved by a median of 12 points (from 79 ± 25 to 67 ± 36), which meets the proposed MCID of 5–10 points. 15 These findings indicate that the improvements are not only statistically significant but also clinically meaningful.
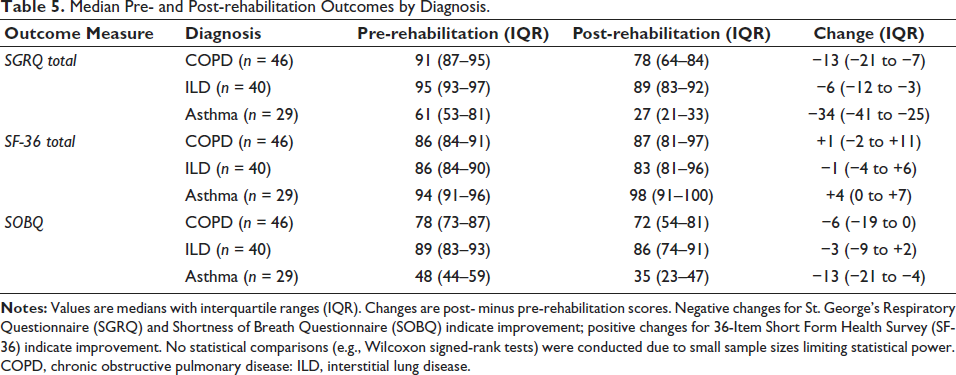
The analysis of potential differences in PR outcomes by diagnosis, an exploratory descriptive analysis was conducted for COPD (n = 46), ILD (n = 40), and asthma (n = 29). Formal subgroup analysis with statistical testing was not performed due to insufficient sample sizes, particularly for asthma (n = 29), which limited statistical power. Table 5 presents median score changes for SGRQ, SF-36, and SOBQ. Asthma patients showed the largest SGRQ total score reduction (−34 points), followed by COPD (−13) and ILD (−6). SF-36 improvements were modest, with asthma showing a four-point gain, COPD a one-point gain, and ILD a one-point decline. SOBQ reductions were greatest for asthma (−13), followed by COPD (6) and ILD (−3). These trends align with the significant multivariate effect of diagnosis (Table 4, p = .001), suggesting variable responses by condition, though formal statistical comparisons were not feasible.
Median Pre- and Post-rehabilitation Outcomes by Diagnosis.
Discussion
The findings of this study demonstrate significant improvements in QoL measures following PR among patients with CRDs. The comprehensive analysis using three validated assessment tools provides robust evidence of the effectiveness of PR programs. The demographic profile of our study population revealed a predominance of female participants (77.39%), with a mean age of 53.83 ± 10.2 years. This aligns with previous research, 16 which reported higher participation rates among middle-aged female patients in PR programs. The distribution of diagnoses, with COPD (40%) being the most prevalent, followed by ILD (34.78%) and asthma (25.22%), reflects the typical pattern of CRDs in rehabilitation settings. 17
The SGRQ results showed substantial improvements across all domains post-rehabilitation (p < .001). The reduction in total SGRQ scores from 92 ± 14 to 63 ± 57 exceeds the MCID of four units established by Jones et al., 13 indicating meaningful clinical improvement. These findings corroborate with Mitchell and Kumar’s systematic review, 18 which demonstrated similar magnitudes of improvement in SGRQ scores following structured rehabilitation programs.
SF-36 outcomes revealed significant enhancements in physical functioning and role physical domains (p < .002). The improvement in physical functioning scores from 13 ± 9 to 20 ± 12 aligns with Wong’s findings, 19 suggesting that PR effectively enhances patients’ physical capabilities and daily activity participation. However, the minimal changes observed in the mental health and social functioning domains indicate a need for greater emphasis on psychosocial support during rehabilitation, as highlighted by Garcia-Martinez et al. 20
The UCSD-SOBQ scores showed significant improvement (p < .001), decreasing from 79 ± 25 to 67 ± 36, suggesting reduced dyspnea perception during daily activities. This improvement corresponds with findings from Anderson’s 21 multicenter study, which reported similar reductions in breathlessness following comprehensive PR. A notable finding was the strong correlation between all three assessment tools (ρ = 0.62–0.66, p < .001). This robust correlation validates the concurrent utility of these instruments in measuring rehabilitation outcomes, supporting previous findings by Lee and Park on the complementary nature of multiple assessment approaches. 22
The clinical relevance of the observed improvements is underscored by their alignment with established MCID thresholds. The SGRQ total score reduction of 29 points far exceeds the MCID of four points, indicating substantial improvements in respiratory-specific QoL. 13 Similarly, the seven-point improvement in SF-36 physical functioning surpasses the MCID of five points, suggesting meaningful enhancements in patients’ daily physical activities. 14 The 12-point reduction in SOBQ scores meets or exceeds the proposed MCID of 5–10 points, reflecting a clinically significant reduction in dyspnea. 15 These findings highlight the practical benefits of PR, supporting its role in improving patient well-being beyond statistical significance. However, variations in MCID responsiveness across specific respiratory conditions warrant further investigation.
These diagnosis-specific outcomes (Table 5) inform clinical practice and rehabilitation program design. Asthma’s large SGRQ (−34) and SOBQ (−13) improvements suggest the intensification of symptom-focused components, such as enhanced breathing retraining and education on trigger avoidance, within the 8-week program. COPD’s moderate gains (−13, −6) support standard aerobic and resistance training, with added psychosocial counseling to address QoL deficits. ILD’s minimal changes (−6, −3) indicate a need for palliative-focused sessions, prioritizing symptom management over intensive exercise. The heterogeneity of respiratory conditions (COPD, 40%; ILD, 34.78%; asthma, 25.22%) likely influences rehabilitation outcomes due to distinct pathophysiology. 14 Exploratory analysis (Table 5) showed larger SGRQ and SOBQ improvements for asthma (−34 and −13 points, respectively) compared to COPD (−13 and −6) and ILD (−6 and −3), possibly reflecting asthma’s reversible airway obstruction versus ILD’s progressive fibrosis. SF-36 trends also favored asthma (+4 points), while ILD showed a slight decline (−1), consistent with its limitations. 17 The significant multivariate effect of diagnosis (Table 4, p = .001) supports these differences, but small sample sizes (n = 29 for asthma) precluded formal statistical analysis. Larger, diagnosis-specific studies are needed to confirm differential effects.
The study’s findings have important clinical implications. First, they support the integration of comprehensive QoL assessments in PR programs, as suggested by Davidson et al. 23 Second, the strong correlations between assessment tools suggest that clinicians might selectively use these instruments based on specific patient needs while maintaining confidence in the outcome measurement validity. 24
The durability of rehabilitation benefits remains uncertain without long-term follow-up data. Prior studies indicate that short-term gains may diminish within 6–12 months without maintenance programs. 25 While our findings demonstrate significant short-term improvements, particularly for asthma, future research should incorporate a 6–12-month follow-up to assess sustainability and inform maintenance strategies.
Conclusion
This study demonstrates the comprehensive effectiveness of PR in improving the QoL across multiple measurement tools. The strong correlations observed between SF-36, SGRQ, and SOBQ scores (ρ = 0.62–0.66) validate their complementary nature in assessing rehabilitation outcomes. The significant improvements in all three measures post-rehabilitation suggest that the benefits of PR extend across various aspects of health-related QoL. The study’s findings support the use of multiple assessment tools to capture the full spectrum of rehabilitation benefits. These results provide valuable insights for healthcare providers in selecting appropriate outcome measures and highlight the robust nature of PR’s positive impact on patient well-being. Future research should focus on determining the MCIDs for these measures in various respiratory conditions.
Limitation
The study on PR’s effectiveness in improving QoL (SGRQ, SF-36, SOBQ) for 115 patients with CRDs (COPD, n = 46; ILD, n = 40; asthma, n = 29) has notable limitations. A significant exclusion of 205 patients (64.06%) during screening due to non-attendance may introduce selection bias, potentially overestimating benefits for less motivated or adherent individuals. Although no dropouts occurred post-enrollment and missing data were minimal (<2%), the complete-case analysis may limit generalizability to populations with higher non-compliance or incomplete assessments. The predominantly female cohort (77.39%) aligns with local participation trends, possibly due to healthcare-seeking behaviors, but restricts applicability to males. The small male sample (n = 26) precluded sex-stratified analyses, limiting insights into sex-specific outcomes. The single-center design ensured intervention consistency, but it may introduce selection bias and reduce applicability to diverse clinical settings. The 8-week intervention lacked a long-term follow-up, hindering the evaluation of sustained benefits. Additionally, the heterogeneity of diagnoses (COPD, ILD, asthma) and small subgroup sizes, particularly for asthma (n = 29), prevented formal statistical comparisons (e.g., Wilcoxon signed-rank tests), despite exploratory analysis (Table 5) suggesting greater improvements for asthma. This complicates condition-specific effects, which is compounded by potential variations in the sensitivity of SF-36, SGRQ, and SOBQ across conditions. These constraints limit differential outcome insights. Future studies should incorporate multicenter designs, balanced sex representation, and extended follow-up to enhance generalizability, explore sex- and condition-specific effects, and validate findings across broader populations.
Footnotes
Abbreviations
BMI: Body mass index; BP: Bodily pain; COPD: Chronic obstructive pulmonary disease; CRD: Chronic respiratory disease; GH: General health; ILD: Interstitial lung disease; IQR: Interquartile range; IRB: Institutional review board; MH: Mental health; PF: Physical functioning; PR: Pulmonary rehabilitation; QoL: Quality-of-life; RC: Reported change; RE: Role emotional; RP: Role physical; SD: Standard deviation; SF: Social functioning; SF-36: 36-Item Short Form Health Survey; SGRQ: St. George’s Respiratory Questionnaire; SOBQ: Shortness of Breath Questionnaire; ρ: Spearman’s correlation coefficient; SPSS: Statistical Package for the Social Sciences; USCD-SOBQ: University of California, San Diego Shortness of Breath Questionnaire; VT: Vitality.
Acknowledgments
The authors extend heartfelt gratitude to all study participants for their valuable time and consent, which made this research possible. The authors would also like to thank the management and staff members of Sparsh Chest Diseases Center, Navrangpura, Ahmedabad, for their assistance during the data collection period.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
The Institutional Ethics Committee approved (GCSMC/EC/ResearchProject/APPROVE/2022/352) all procedures. Written informed consent was obtained from all the participants before enrollment. All data of the participants were strictly maintained and kept confidential and anonymous.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.