
Abstract
Background
Subgingival plaque biofilm is a potential harboring site for bacteria and viruses, serving as a source of entry into the bloodstream. The presence of Severe Acute Respiratory Syndrome Coronavirus 2 RNA (SARS-CoV-2 RNA) in subgingival plaque could be a possible source for cross infection due to aerosol contamination during dental procedures.
Objectives
The objective of this study was to investigate the presence of SARS-CoV-2 RNA in the subgingival plaque biofilm of patients who recovered from COVID-19 infection.
Materials and Methods
Ten subjects visiting the Outpatient clinic with a previous history of COVID-19 infection were recruited for this cross-sectional study. Subgingival plaque sample was collected from all four quadrants using a sterile curette. Nasopharyngeal and oropharyngeal swabs were taken from all the subjects. Reverse transcriptase real-time qualitative polymerase chain reaction (RT-PCR) was used to determine the presence of SARS-CoV-2 RNA using BAG SARS-CoV-2 RT-PCR kit targeting E gene, RdRp gene, and internal control.
Results
Ten participants (seven females and three males) with a previous history of COVID-19 infection were included in the study. Six participants previously presented with mild COVID-19 infection (uncomplicated upper respiratory tract infection, mild fever, cough, sore throat, nasal congestion, malaise, headache, without evidence of breathlessness or hypoxia), and four participants previously presented with moderate COVID-19 infection (dyspnea and or hypoxia, fever, cough, SpO2 90%–94% on room air, respiratory rate more or equal to 24 per minute) according to clinical management protocol for COVID-19, Government of India. The nasopharyngeal, oropharyngeal, and subgingival plaque samples tested negative for SARS-CoV-2 RNA.
Conclusion
The absence of the SARS-CoV-2 virus in the subgingival plaque sample of patients recovered from COVID-19 infection suggests that dental plaque could not be a potential reservoir of the virus. However, clinicians should take at most precautions while treating the patients recovered from COVID-19 infection and should anticipate a change in subgingival environment leading to alteration in periodontal disease progression.
Introduction
In 2019, a pneumonia outbreak with an unknown etiology occurred in China. This disease condition was found to be caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) and hence was named Corona Virus Disease 2019 (COVID-19). In March 2020, COVID-19 was declared a pandemic by the World Health Organization (WHO), due to an increase in the number of COVID-19 cases worldwide. 1 Recent research is being done to understand the pathobiology of the COVID-19 infection and thus to ascertain the prevention of disease spread. The human body can harbor SARS-CoV-2 RNA at various sites and its presence has been detected in nasopharynges, oropharynges, lower respiratory tract secretions, bronchoalveolar lavage fluids, blood, rectal swabs, and feces. 2 An extensive meta-analysis by Cevik et al. 3 has suggested that the maximum duration of shedding of SARS-COV-2 RNA in the population recovering from COVID-19 infection was 60 days in serum samples, 126 days in stool samples, and 83 and 59 days in upper and lower respiratory tracts, respectively. 3 The presence of viral RNA in the salivary gland was discovered recently, and saliva was identified as the critical route of interindividual transmission.4, 5 Huang et al. 6 suggest that the virus can persist in saliva or nasopharynx for 2 months, and in asymptomatic individuals, the viral clearance was observed after 3.5 weeks. 6 Understanding the harboring sites of this virus, which can be the virus’s potential point of entry, is pivotal in managing its spread. The oral cavity has several intra-oral niches such as the cheek mucosa, tongue, hard and soft palates, tonsils, teeth, and gingival sulcus which are capable of harboring several types of microorganisms including viruses.7–10 The plaque biofilm on the non-shedding tooth surface harbors micro-organisms in a complex environment that can resist host immune response and other pharmaceutical agents unless it is mechanically disrupted.11, 12 The microorganism can detach from the plaque biofilm and gain systemic entry during the process of plaque maturation. 13 Hence, in this study, we will be assessing the presence of SARS-CoV-2 RNA in the subgingival plaque sample of the subjects who have been previously infected with COVID-19 infection within the last 6 months, to understand the possible role of dental plaque as a reservoir of SARS-CoV-2 virus.
Materials and Methods
A cross-sectional study was conducted in the Department of Periodontology, Sri Ramachandra Dental College and Hospital, during the period of January 2022 to June 2022. The study protocol was approved by the Institutional Ethics Committee (IEC), Sri Ramachandra Institute of Higher Education and Research (IEC-NI/21/OCT/80/139), and was conducted in accordance with the Helsinki criteria. Written informed consent was obtained from the study participants.
As this is the first study of its kind to assess the presence of the SARS-CoV-2 virus in subgingival plaque samples of patients recovered from COVID-19 infection, an exploratory study with a convenient sample size of 10 subjects was conducted. Patients visiting the outpatient clinic in the Department of Periodontology, Sri Ramachandra Dental College and Sri Ramachandra Medical Centre, Post-COVID care clinic, were screened, and 10 patients were recruited for the study. Patients in the age group of 18–30 years with a previous history of COVID-19 infection in the last 6 months and with fair/poor oral hygiene maintenance were included in the study. Pregnant and lactating women, patients who had been treated for periodontal disease in the last 6 months, and those with other infectious diseases such as tuberculosis, hepatitis, and HIV infection were excluded from the study. A detailed proforma comprising the patient’s demographic data, oral hygiene status, periodontal parameters, history, and severity of COVID-19 infection was recorded. According to the clinical severity and assessment parameters as per the clinical management protocol for COVID-19 by the Government of India, subjects were categorized into mild, moderate, and severe. 14
Sample Collection and Data Analysis
Patient recruitment, clinical examination, and elicitation of extensive history and severity of COVID-19 infection were performed using a structured proforma by a single investigator. The kappa value was >90% while assessing for the intra-investigator variability. Subgingival plaque samples were collected from all four quadrants following adequate isolation using sterile curettes. Nasopharyngeal and oropharyngeal swab samples were also obtained. All the samples were immediately transferred into a viral transport medium and stored at −80°C until further processing. Reverse transcriptase real-time qualitative polymerase chain reaction (RT-PCR) was done to detect the presence of SARS-CoV-2 RNA using a BAG SARS-CoV-2 RT- PCR kit targeting the E gene, RdRp gene, and internal control. Based on the Indian Council of Medical Research (ICMR) guidelines, the cycling threshold (CT value) of a targeted gene less than 35 was considered positive and more than 35 was considered negative. Descriptive analyses such as mean, standard deviation, and percentage were assessed for all continuous variables such as age, Oral Hygiene Index – Simplified score, 15 probing pocket depth, and disease severity, using the SPSS 18 (IBM) software.
Results
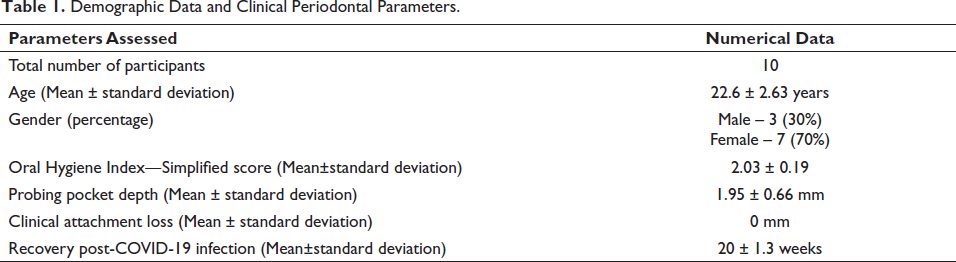
The demographic data (Table 1) shows that the total number of subjects recruited for the study was 10 of which 3 were male and 7 were female. The patient cohort recruited was in the mean age group of 22.6 ± 2.63 years. The clinical parameters recorded showed that the subjects had fair oral hygiene maintenance (OHI-S score: 2.03 ± 0.19) with a probing pocket depth of 1.95 ± 0.66 mm.
Demographic Data and Clinical Periodontal Parameters.
All the study participants tested RT-PCR positive for COVID-19 infection in the last 6-month duration. Based on the Clinical management protocol for COVID-19, the Government of India, 60% of the study participants were categorized as mild and 40% had moderate COVID-19 infections (Table 2).
History of Disease Severity in Subjects Previously Exposed to COVID-19 Infection From January 2022 to June 2022.
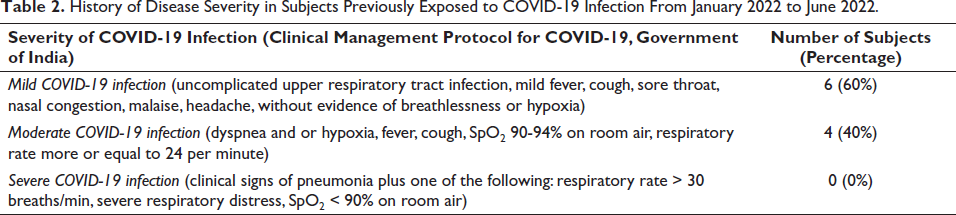
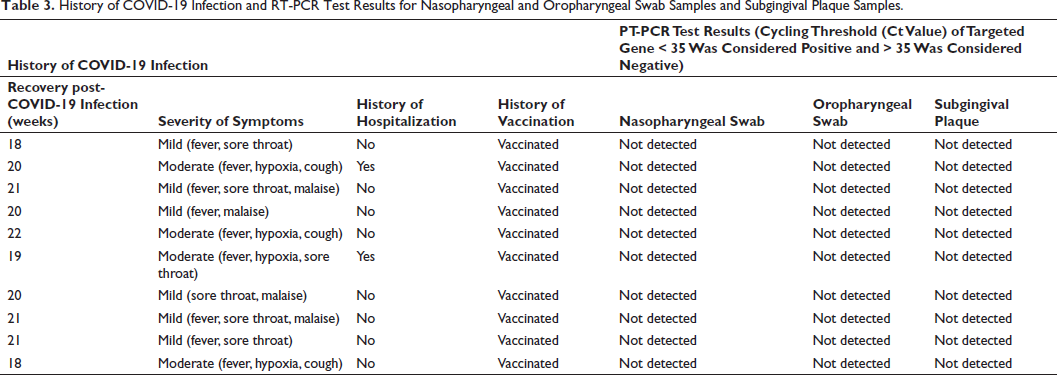
Table 3 describes the history of COVID-19 infection and the RT-PCR test results among the study participants. The COVID-19 history of the participants revealed that they had symptoms such as fever (80%), sore throat (60%), malaise (40%), hypoxia (30%), and cough (20%), and two participants gave a history of hospitalization. All the participants were vaccinated for COVID-19 infection at the time of the study. The nasopharyngeal and oropharyngeal swab samples and subgingival plaque samples from all the subjects were collected 20 ± 1.3 weeks post-recovery from COVID-19 infection. The samples were assessed for the presence of SARS-CoV-2 RNA using RT-PCR, and the results were negative/not detected for all the samples, based on cycling threshold values that were considered negative if more than 35 according to the Indian Council of Medical Research (ICMR) guidelines.
History of COVID-19 Infection and RT-PCR Test Results for Nasopharyngeal and Oropharyngeal Swab Samples and Subgingival Plaque Samples.
Discussion
In the early 1990s, various studies have proved the role of viruses in periodontal disease pathogenesis. As Epstein–Barr virus, human cytomegalovirus, and herpes simplex virus have been detected in periodontal pockets, they are described as pathogens related to periodontal disease.16–18 Literature also suggests the presence of viruses in the complex communities associated with subgingival plaque biofilm and infiltration of viruses from the biofilm into the bloodstream was also detected. 19 The source of viruses in periodontal tissues could be either direct infection exposure in the mouth or infiltration of infected immune cells from the bloodstream into the sites with periodontal disease. 20
The epithelial cells of oral mucosa exhibit high expression of angiotensin-converting enzyme II (ACE2) receptors, which is required for the attachment, multiplication, and entry of SARS-CoV-2, leading to infection. 21 A study by Gomes et al. 22 hypothesized that dental biofilm might be a potential reservoir for SARS-CoV-2 RNA in symptomatic COVID-19 subjects and could have an essential role in COVID-19 transmission. Notably, 18.6% of the sample population tested positive for SARS-CoV-2 in the dental biofilm of which 46.2% presented with flu-like symptoms. 22
Various studies have been conducted to establish an association between oral health and COVID-19 infection. A recent study elicited the presence of SARS-CoV-2 in gingival crevicular fluid (GCF) and saliva in subjects who were COVID-19 positive upon nasopharyngeal sampling which was considered a gold standard. The viral RNA was detected in 63.64% of the GCF samples and 64.52% of the saliva sample. Considering the sensitivity of GCF when compared with saliva, GCF was suggested as a possible mode of viral transmission in COVID-19-infected patients. 23
Our study results show an absence of SARS-CoV-2 RNA in subgingival plaque samples of patients who recovered from COVID-19 infection in the last 6 months. A conceivable reason could be that the study population involved subjects with mild and moderate COVID-19 infections. Hence, the viral load could be potentially less as it correlates with disease severity. 24 Our sample population includes subjects who completely recovered from the infection, currently presenting with no related symptoms, and have been vaccinated against COVID-19 infection.
The potential limitations of the study include the subgingival plaque samples being collected approximately 20 weeks post-recovery from COVID-19 infection, thereby leading to a possible reduction in viral load. The sample size was inadequate, and the population did not include severe cases of COVID-19 infection. Though the result of this study does not indicate the presence of the SARS-CoV-2 virus in patients recovered from COVID-19 infection, dental healthcare professionals are still advised to follow guidelines given by the governing bodies to prevent cross-infection.
Conclusion
Dental plaque could not be a potential reservoir of the virus, due to the absence of SARS-CoV-2 virus in the subgingival plaque sample of patients recovered from COVID-19 infection. However, an assessment of a larger sample population needs to be conducted to prove the hypothesis. Hence, all necessary personal protective measures must be taken by the clinicians while treating the patients recovered from COVID-19 infection. A change in the subgingival environment must be anticipated, leading to alteration in periodontal disease progression. Hence, a modification in periodontal maintenance care is suggested.
Abbreviations
Footnotes
Acknowledgments
The authors wish to thank the laboratory staff from Central Lab, Sri Ramachandra Medical Centre, for their valuable technical support in this project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study protocol was approved by the Institutional Ethics Committee (IEC), Sri Ramachandra Institute of Higher Education and Research (IEC-NI/21/OCT/80/139).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.