
Abstract
Objective:
To evaluate the impact of ketamine following spinal anesthesia on the duration of postoperative analgesia and the need for analgesics.
Methods:
This was a prospective, randomized, double-blinded placebo-controlled study done over a period of two years. A total of 60 participants undergoing elective surgeries under spinal anesthesia were randomized into two groups. After 10 min of spinal anesthesia and achieving the required level of sensory and motor blockade, both groups were given Inj. Midazolam 1 mg intravenously, followed by Inj. Ketamine 0.25 mg/kg, volume made up to 10 mL with normal saline, given intravenously for Group K and Inj. Normal Saline 10 mL was given intravenously for Group N. Hemodynamic monitoring was done intraoperatively, and the postoperative visual analog score (VAS), sedation score, the mean time for the first rescue analgesia, and the total dose of postoperative analgesic required in 24 h were tabulated.
Results:
There was no statistical difference between the two groups in terms of age, weight, ASA grade, and duration of surgery. In Group K, the VAS scores were significantly lower and patients were comfortable when compared to Group N (P value <.01). The mean time to first rescue analgesia was longer in Group K (6.4 ± 1.69 h) when compared to Group N (2.9 ± 1.01 h), and the total dose of postoperative analgesia (Tramadol) required in 24 h was also significantly less in Group K (143.33 ± 56.83 mg) when compared to Group N (236 ± 49.01 mg). Changes in hemodynamic parameters (heart rate and mean arterial pressure (MAP)) were statistically and clinically not significant in both the intraoperative and postoperative periods between the groups.
Conclusion:
Patients in Group K were more comfortable, had a longer duration of postoperative analgesia, and required less dose of rescue analgesia in the postoperative period. Ketamine is a safe drug that is readily available, and it decreases the use of opioids and opioid-related side effects. Therefore, ketamine can serve effectively as an adjunctive analgesic drug.
Introduction
Pain can be defined as an “unpleasant feeling and an emotionally charged experience connected with actual or potential tissue damage or described in terms of such damage,” according to the International Association for the Study of Pain. 1
Ketamine was synthesized for the first time in 1962. It is a one-of-a-kind intravenous (IV) anesthetic that, among other things, promotes sleepiness, catalepsy, somatic analgesia, bronchodilation, and sympathetic nervous system activation. 2 Ketamine is lipid soluble and rapidly degrades, allowing it to be transferred to peripheral organs. It is metabolized extensively in the liver through the N-demethylation and ring hydroxylation pathways.3, 4 Ketamine causes dissociative anesthesia, in which the patient looks to be awake but is separated from his or her surroundings while keeping his or her eyes open. 5 The main mechanism of action is the noncompetitive antagonism of the N-methyl D-aspartic acid receptor. It also interacts with opioid receptors, monoamine, cholinergic, purinergic, and adrenoreceptor systems and has local anesthetic effects. 6 Ketamine is useful in the treatment of severe pain, including injuries, fractures, stomach and flank discomfort, low back pain, and extremity pain, according to a significant body of research. Low-dose ketamine, also known as subdissociative dosing of ketamine, is used for pain management alone or in combination with other drugs. 7 The results, on the other hand, are mixed. Some studies have shown that ketamine reduces pain scores and, as a result, the need for opioids after surgery.8, 9, 10 Various drug combinations have been used to investigate the effect of ketamine on postoperative pain after spinal anesthesia. 8
Therefore, we studied the effect of intravenous ketamine on hemodynamics and postoperative pain in patients undergoing surgery under spinal anesthesia.
Methods
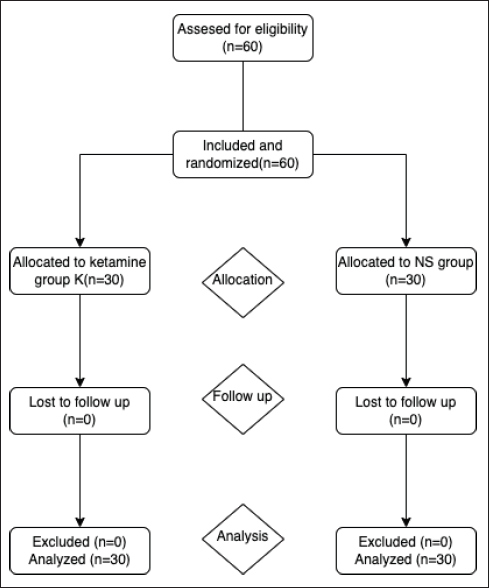
After approval from the Institutional Ethics committee and informed consent was taken, we did a prospective, randomized, double-blinded study done over a period of two years in 60 patients. Inclusion criteria were patients belonging to either sex, aged 18 to 60 years, ASA I and II status, and undergoing elective surgeries under spinal anesthesia. Exclusion criteria were the patients with the major neurological, cardiac, respiratory, metabolic, renal, and hepatic disease with coagulation abnormalities, patients belonging to ASA grade >2, and patients allergic to study drugs. Written informed consent was taken from all patients. In the study carried out by Behdad et al., 11 total analgesic consumption in ketamine and midazolam groups was 54.17 ± 12.80 mg and 74.44 ± 33.82 mg, respectively. We used the difference between the above-mentioned two means and the OpenEpi software, (Massachusetts, USA) to calculate the sample size. We set the confidence interval to 95% and the power of the study to 80%. With this calculation, we got a total sample size of 52, with 26 in each group (Groups N and K). Considering all the exclusion and dropouts, we took a total sample size of 60, with 30 in each group. Both the groups were given Inj. Midazolam 1 mg intravenously, followed by the study drug Inj. Ketamine 0.25 mg/kg, volume made up to 10 mL with normal saline, given intravenously in 30 cases, and Inj. Normal Saline 10 mL intravenously given in 30 cases.
CONSORT Diagram Showing Enrolment, Allocation and Analysis at Every Stage of Randomized Control Trial. n = Number of Patients.
The preoperative visit was conducted on the previous day of surgery, and a detailed history and complaints were noted. Informed consent was taken. Patients were kept nil by mouth from midnight prior to surgery.
On the day of surgery, after shifting the patient to the operation theatre, the pulse oximeter, ECG, and noninvasive blood pressure monitoring devices were fitted. The baseline vitals were taken. A 20-G cannula was used to secure IV access. All of the patients were given 10 mL/kg of Ringer’s lactate fluid before spinal anesthesia.
The patients were placed in a sitting position. One minute later, the back was cleaned with a 10% betadine solution and allowed to dry. After 1 min, betadine was cleaned with the methylated spirit, and the region was covered with a sterile drape. A 26-G needle was used to infiltrate the intervertebral area between the third and fourth lumbar spines with 1 cc of 2% lignocaine. At the L3–L4 intervertebral space, a lumbar puncture was performed in the midline using a 26-G Quincke spinal needle; free flow of clear cerebrospinal fluid (CSF) was confirmed, and 3 mL of 0.5% hyperbaric Bupivacaine hydrochloride was given intrathecally.
The patient was placed supine immediately, and all the vital parameters were noted. The cephalad spread of sensory blockade was checked using the pinprick method at regular intervals. The motor blockade was checked using the Bromage scale. After 10 min of spinal anesthesia and achieving the required level of sensory and motor blockade, both the groups were given Inj. Midazolam 1 mg intravenously, followed by the study drug Inj. Ketamine 0.25 mg/kg, volume made up to 10 mL with normal saline, given intravenously in Group K (30 cases), and Inj. Normal Saline 10 mL intravenously given in Group N (30 cases).
All patients received 4 L of oxygen supplementation with a Hudson mask. The vital parameters (heart rate, blood pressure, SPO2, and ECG) were noted at 1 min, 5 min, and every 10 min after drug administration till the completion of surgery. Any discomfort, nausea, vomiting, shivering, pain, bradycardia, or other side effects were monitored. After completion of the surgery, patients were shifted to the postoperative recovery room and observed for 6 h. Postoperative VAS score and sedation score were noted at the intervals of 30 min, 60 min, 90 min, and 6 h. Sedation was assessed using the Richmond Agitation Sedation Score (RASS). After 6 h, patients were shifted to the ward.
Patients were given Inj. Ondansetron 4 mg followed by Inj. Tramadol 100 mg IV in 100 mL NS on demand for rescue analgesia during the postoperative period if their pain score was greater than 5 on the Visual Analogue Scale (VAS). If a patient’s pain score was 5 or higher, rescue analgesics were administered. The time of the rescue analgesic administration was recorded, and a chart was maintained. Patients were monitored 24 h postoperatively, and the total number of tramadol doses required in 24 h was noted. The duration of postoperative analgesia was taken from the administration of spinal anesthesia to the first rescue analgesic administration. Any postoperative complaints, like nausea, vomiting, and disturbing dreams, were also observed.
All of the cases were completed in the allotted time. Data were entered onto an excel sheet and evaluated with a Social Science Statistical Software 20 (SPSS Inc. Chicago). The information was gathered, organized, and tabulated. The parametric test was used to conduct the statistical analysis, and the “Z” test (standard normal variant) was used to interpret the results with a 95% level of significance. The Student “t” test was used to analyze quantitative data, whereas the Chi-square test was used to analyze qualitative data.
Results
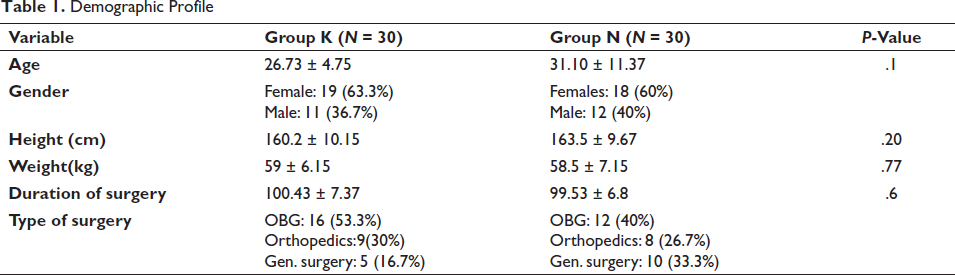
The demographic profile was comparable in both groups. The mean age in the ketamine group was (26.73 ± 4.75) years, whereas in the control group, the mean age was (31.10 ± 11.37) years. The variations in terms of the age of study subjects were statistically nonrelevant (P > .05). The gender-wise distribution of cases showed that out of 60 study subjects, 37 (61.7%) were females and 23 (38.3%) were males, and gender distribution was comparable in both groups.
The types of surgeries in both the groups were compared, and it was found that obstetrics and gynecological procedures (46.7%) were more than other surgical procedures (53.3%) in both the groups.
The duration of surgery was compared, but it was not statistically significant.
Demographic Profile
The hemodynamic parameters (heart rate and MAP) were statistically and clinically not significant in both the intraoperative and postoperative periods.
Postoperative Scores and Analgesic Requirement
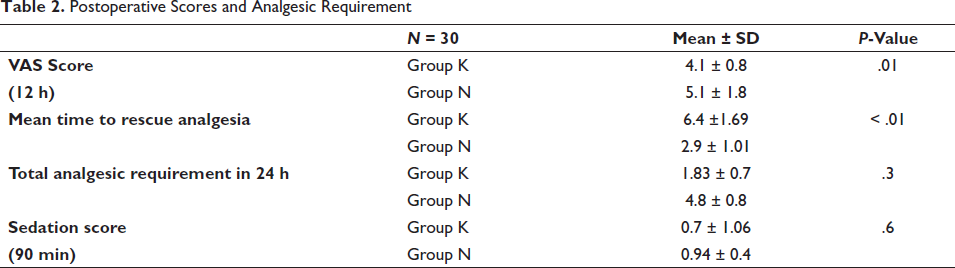
Figure 2 shows the comparison of VAS scores between two study groups (n = 30 in each group). Mean and standard deviation were calculated for each group, and a comparison was made. The comparison was found to be significantly low throughout the postoperative period in Group K. The mean VAS scores ranged from 0.1 ± 0.54 to 4.1 ± 0.8 in Group K and from 1.7 ± 1.11 to 5.1 ± 1.8 in Group N throughout the postoperative period. Patients were more comfortable and calmer in Group K compared to Group N.
VAS Score.
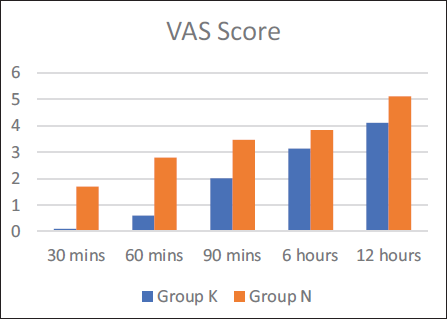
Figure 3 shows the comparison of time to rescue analgesia between the two study groups (n = 30 in each group). Mean and standard deviation were calculated for each group, and a comparison was made. It was found that the time for the first rescue analgesia administration was longer in Group K compared to Group N. It was found that the mean time for the first rescue analgesia in Group K was 6.4 ± 1.69 h, and it was given after 2.9 ± 1.01 h in Group N.
Mean Time to Rescue Analgesia.
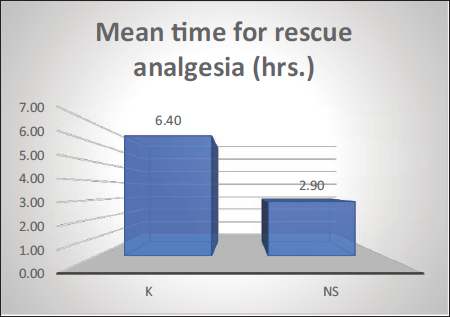
Figure 4 shows the statistical results of the total dose of analgesic in 24 h in both groups (n = 30 in each group). The mean dose of Inj. Tramadol received was 143 ± 56.83 mg by Group K and 239 ± 49.01 mg by Group N. The total dose of analgesic received by Group K was less than that by Group N. This shows that the duration of analgesia was longer in Group K compared to Group N.
Total Dose of Analgesic in Milligrams in 24 h.
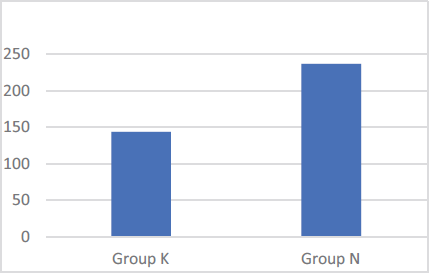
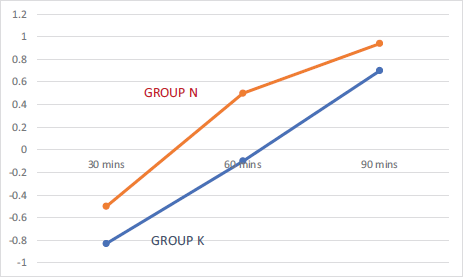
Figure 5 shows the comparison of sedation scores between both groups (n = 30 in each group). The sedation scores ranged from –0.83 ± 0.79 to 0.94 ± 0.4 for Group K and –0.5 ± 0.5 to 0.94 ± 0.4 for Group N. It was found that the comparison was statistically not significant throughout the postoperative period.
Sedation Score.
No other significant postoperative side effects were observed in either group.
Discussion
Surgical operations almost always result in tissue damage and pain. Inadequate pain management has long been recognized as having negative consequences, including delayed mobilization and accompanying complications, as well as psychological discomfort and worry. 12
Ketamine is a commonly used general anesthetic and intraoperative analgesic that has been in use for nearly forty years. High dosages of ketamine act as an intravenous anesthetic, whereas modest doses of ketamine act as an analgesic agent, as is widely documented. 12 There are a variety of alternative options for managing postoperative pain. Opioids, like morphine and pethidine, are the most widely prescribed drugs; yet, they are often associated with a slew of negative side effects, such as postoperative respiratory depression, itching, nausea, vomiting, and addiction. Different amounts of ketamine can be delivered in a variety of ways as an alternate technique for treating postoperative pain. 13
In our study, the mean VAS scores ranged from 0.1 to 4.1 in Group K and 1.7 to 5.1 in Group N throughout the postoperative period. Patients were more comfortable and calmer in the ketamine group compared to the control group. This finding was similar to Behzad’s 11 study, where the pain scores in the ketamine group (0.78 ± 1.09) were significantly lower than that in the control group (1.72 ± 1.22) during the first hours after cesarean section.
In our study, the mean time to the first rescue analgesia was 6.5 h in Group K and 2.9 h in Group N, which was similar to a study done by Anil Kumar Bhiwal, 14 in which ketamine received by the Ka group was 0.15 mg/kg and the Kb group was 0.3 mg/kg given intravenously 5 min after delivery; Group C received 2 mL of 0.9 percent NS, and the time to the first analgesic requirement was significantly prolonged in the Ka group (5.44 ± 1.45 h) and the Kb group (6.18 ± 1.61 h) as compared to the control group (4.97 ± 1.48 h).
In our study, the total dose of rescue analgesia (tramadol) given in 24 h in Group K was (143 ± 56.8 mg), which was significantly less when compared to Group N (236.6 ± 49.01mg), which was similar to the study done by Richard Mwase’s 15 double-blinded study in 2014, in which he evaluated the analgesic effects of preincision ketamine on postspinal cesarean in Uganda’s Tertiary Hospital in a total of 88 parturient, with 44 each assigned to experimental and control groups. The ketamine group was given 0.25 mg/kg of ketamine, and the placebo group was given normal saline 10 mL. The total dose of rescue analgesia dose of Tab. Diclofenac 75 mg IV was lower in the ketamine group when compared to the placebo group, which is the same as our finding.
In our study, it was found that sedation scores were statistically and clinically not significant. Sedation scores were compared in the study done by Sen et al. 16 They studied the analgesic effects of low-dose intravenous ketamine after spinal anesthesia for cesarean section in three randomized groups of 90 patients undergoing elective cesarean section. Ketamine (0.15 mg kg) or an equal volume of normal saline was given intravenously immediately after initiating spinal anesthesia in the ketamine and control groups. In the fentanyl group, 10 µg of fentanyl was added to the intrathecal bupivacaine. They observed mild sedation in only two patients (6.6%).
No other significant postoperative side effects were observed in either of our study groups.
Conclusion
Based on our study, we conclude that Inj. Ketamine 0.25 mg/kg intravenously after spinal anesthesia maintains good intraoperative hemodynamic stability, lowers postoperative pain scores, and minimizes the need for comprehensive rescue analgesia in the first 24 h after surgery. Because of the reduction in discomfort, this aids in achieving early postoperative ambulation. Ketamine is a safe and generally available medication that reduces the use of opioids and their associated negative effects. As a result, ketamine can be used as a complementary analgesic.
Limitations
Because of the small sample size, it is impossible to extrapolate the results to all patient populations. Midazolam injection was given prior to ketamine injection which might have effect on sedation and VAS scores.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
Not applicable
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable