
Abstract
This article presents an overview on nonsuicidal self-injury in Southeast Asia. Following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, a systematic review was conducted regarding self-injury in Southeast Asia. Seventeen studies eligible for inclusion were identified. Findings revealed that self-injury is most common among youth between the ages of 14 and 35 years old. The prevalence rates reported were from 7.1% to 11.4% in community samples and 20.7% to 75.9% in clinical samples. The most common function for self-injury is that it serves as an emotion regulation strategy, and the main causes appear to stem from individual (emotional dysregulation, low self-esteem, gender and psychiatric disorders) and environmental factors (childhood maltreatment, childhood neglect, parental invalidation and academic stress). Comorbidity with depressive disorders, adjustment disorders and anxiety disorders are most often reported. The paucity of studies with high heterogeneity calls for further research exploring self-injury which may inform better mental health practice and policymaking in Southeast Asia.
Introduction
Nonsuicidal self-injury (NSSI), often referred to as self-harm, is a rising clinical and public health problem around the world (Cipriano et al., 2017). NSSI refers to ‘the deliberate, self-inflicted damage of the body tissue without suicidal intent and for purposes not socially and culturally sanctioned’ (International Society for the Study of Self-Injury, 2018). The most common examples of NSSI are cutting, burning, scratching, hitting and punching. Other forms of NSSI include extreme skin picking, biting and intentionally preventing wounds from healing. Despite the fact that self-injury has always been present among us, NSSI was only incorporated as a disorder by itself in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). The most important difference between suicidal behaviour and self-injury is the intent. Individuals who are suicidal are experiencing severe life stressors and/or mental disorders that cause unbearable pain, and suicide is seen as the only option to end their pain. Suicidal ideations and attempts generally stem from a place of worthlessness, hopelessness and despair. Individuals who engage in NSSI, on the other hand, do so as a way to cope with their stressors and adverse emotions. NSSI is mainly used as a coping strategy against ending one’s life.
In addition, the psychological effect of NSSI is distinct from suicide attempts. NSSI is linked to reduced negative affect and heightened positive affect (Cipriano et al., 2017). While suicide attempts may lead to more depressive symptoms and distress that the prior attempt was unsuccessful (Park et al., 2018). In most cases, suicidal thoughts and attempts come after prolonged engagement in NSSI. Past studies have shown that NSSI is a significant risk factor of subsequent suicidal behaviour (Castellví et al., 2017; Kiekens et al., 2018). NSSI can progress into suicidal behaviour when self-injury is no longer an effective coping method to regulate one’s emotions. This is because over time individuals become desensitized or habituated to the physical pain and develop a concurrent desire to escape their stressors and emotional sufferings altogether through suicide.
There is a plethora of research in the West examining the function, prevalence and aetiology of NSSI. The most common function of NSSI is emotion regulation (intrapersonal function) and expressing distress (interpersonal function) (Taylor et al., 2018). Nevertheless, findings generated from global studies on the aetiology and prevalence of NSSI have been for the most part heterogenous. Till date, there is no consensus on the exact prevalence and underlying causes of NSSI. A review by Gillies et al. (2018) reported that 16.9% of all people self-injure during their lifetime. However, this review included past studies on self-injury with suicidal intent. Another review revealed the prevalence rates range between 7.5% and 46.5% for adolescents, 38.9% for college students and 4% and 23% for adults (Cipriano et al., 2017). Then again, this review was limited to mostly Western nations, for example, the USA, Belgium, Germany, Spain, Canada, England and Italy. Only two studies were from China (representing Asia) (Tang et al., 2016; Wan et al., 2015).
There are certain factors that may heighten the risk of NSSI. The most common factor is childhood sexual, physical or emotional abuse (Cipriano et al., 2017; Liu et al., 2018). Apart from that, NSSI seems to co-occur with a myriad of mental disorders. Comorbidity rates are particularly high for borderline personality disorder, depressive disorders, anxiety disorders, post-traumatic stress disorder and eating disorders (Cipriano et al., 2017). Having friends who self-injure can also lead individuals to begin self-injuring (Schwartz-Mette & Lawrence, 2019; Victor & Klonsky, 2018). Nonetheless, little is known about the cultural differences in NSSI. Past studies on NSSI are rooted in a set of centuries old Western philosophical assumptions conducted in an individualist-oriented society. The researchers and samples over the past century have been monopolized by Western regions such as Europe, the USA, Canada and Australia. These studies may have mistaken specific cultural twists that may differ from culture to culture. There are clear cultural differences (e.g., cultural, familial and social values) between Western and Asian countries, which may impact the prevalence, function and aetiology of NSSI. An awareness of these differences is imperative to develop specific treatment methods and preventive measures for NSSI.
Asia is the largest continent on Earth and is divided into five regions which are Central Asia, West Asia, South Asia, East Asia and Southeast Asia. Central Asia includes Tajikistan, Uzbekistan, Kazakhstan, Turkmenistan and Kyrgyzstan. These five countries became independent after the dissolution of the former USSR in 1991 (Savani et al., 2020). Consequently, these countries are undergoing severe growing pains as they continue to adjust to the rapid shift in economy, social-political philosophy and COVID-19 as independent countries. Currently, they are focusing on fulfilling the basic needs of their citizens such as healthcare, education and sufficient jobs. As a result, NSSI research in Central Asia is virtually non-existent.
West Asia encompasses middle eastern countries such as Syria, Lebanon, Palestine, Iran, Jordan, Iraq, Oman, Yemen, Kuwait, Bahrain, Qatar and Saudi Arabia. Research on NSSI in West Asia is still in its infancy. A study by Hanania et al. (2015) revealed that the lifetime prevalence of NSSI is 22.6% among Jordanian youth. Whereas Gholamrezaei et al. (2017) revealed the lifetime prevalence of NSSI is 12.3% among Iranian youth. Contrary to the findings from the West, the former study reported more males having engaged in NSSI, but the latter study found no gender differences. While countries such as Iraq, Syria, Yemen, Lebanon and Palestine are either experiencing civil war or enduring substantial costs of the past civil war and other post conflict impacts. Hence, research on self-injury is often associated with post-traumatic stress disorder in asylum seekers or refugees (Gargiulo et al., 2020; Sami & Hallaq, 2018). Hence, more research is warranted to improve our understanding on the cultural nuances in this region before a systematic review can be conducted.
South Asia is divided into India, Pakistan, Nepal, Bangladesh, Sri Lanka, Bhutan and the Maldives. NSSI is not well recognized as an independent concept in South Asia and has received limited research attention. For instance, a systematic review by Gandhi et al. (2016) of 38 articles in India showed discrepancies in the definitions of self-injury and spotted only one research which clearly used a definition of NSSI according to the international nomen- clature (Kharsati & Bhola, 2015). Similarly, research in Pakistan, Sri Lanka and Bangladesh recorded inconsistent definitions of self-injury associating it with suicidal behaviour, with self-poisoning being the most common method (Akter et al., 2018; Husain et al., 2019; Pushpakumara et al., 2019). Hence, more culturally relevant studies are needed in these countries according to the DSM-5 definition of NSSI in order to have a consensus understanding on the prevalence, function and risk factors of NSSI.
East Asia is divided into China, Macau, Hong Kong, Taiwan, North Korea, South Korea, Japan and Mongolia. Research on NSSI in East Asia has been predominantly reported in China. A meta-analysis of a total of 26 Chinese studies revealed the prevalence rate was 22.37% among youth (Lang & Yao, 2018). The most salient theme to emerge from research in East Asia is that NSSI functions as an emotion regulation or coping strategy (Lee, 2016; Ren et al., 2018; Tian et al., 2021; Tresno & Mearns, 2016; Wong & Chung, 2021). Similarly, most studies report that the risk factors of NSSI are childhood maltreatment or poor relationship with others (Kang et al., 2018; Lee et al., 2020; Ren et al., 2018; Tian et al., 2021; Tresno & Mearns, 2016). These results are logical given the cultural similarities of these countries. Some of the defining cultural characteristics are that they share language roots or traditional writing systems (e.g., Hanzi) as well as common religious and ethical notions related to Buddhism, Confucianism and Taoism.
Southeast Asia is divided into 11 countries that are Brunei, Cambodia, Indonesia, Laos, Malaysia, Myanmar, the Philippines, Singapore, Thailand, East Timor and Vietnam. Southeast Asians are primarily a collectivist society who value selflessness, working as a group in which families and communities have a key role as opposed to individualistic societies (e.g., Europe and North America) who value autonomy and focus on the individual needs over the needs of the group (Cherry, 2020). These characteristics catalyse in the upbringing of children and individuals having different perspectives on life. For instance, family members in a collectivist society are expected to maintain familial values, for example, maintaining harmonious relationships, obedience, cooperation and helpfulness (Sumari et al., 2020). Therefore, from young, Southeast Asians tend to use indirect communication and be less expressive. As they are forced to constantly suppress their frustrations, they may use NSSI as a method to release pent-up frustrations.
Despite Southeast Asia’s rich cultural and ethnic diversity, they share similar values. Much of these shared values inform mental health and family life. Ethnically homogeneous nations such as China, Japan, Korea, India and Saudi Arabia contrast with the linguistic and religious heterogeneity of Southeast Asian societies. Besides that, findings from western studies and research from other Asian regions may not be consistent with the cultural norms of Southeast Asians. Hence, it is pertinent to systematically review studies in Southeast Asia, identify patterns and develop potential themes for NSSI. The authors aimed to address this knowledge gap by conducting a systematic literature review to uncover the prevalence, function and aetiology of NSSI in Southeast Asia. The evidence synthesized in this article will render an overview of NSSI in this region, which may inform better decision-making and future research on NSSI in Southeast Asia.
This article is organized into five sections. Section I, Introduction, provides the background of the study with its research objectives. Section II, Methodology, describes the methods used to identify and appraise past studies performed in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Section III, Results, presents the findings of this study. Section IV, Discussion, closely interprets the results in the context of the review and presents the limitations of this study. Lastly, Section V concludes the article with recommendations for future research on NSSI.
Methodology
This systematic review was performed in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Shamseer et al., 2015). Prior to the formal commencement of this study, a protocol was published on the PROSPERO database (registration number: CRD42022302114).
Inclusion and Exclusion Criteria
Studies were chosen in line with the following inclusion criteria: (a) English language (as the authors understand this language); (b) published in a peer-reviewed journal; (c) contain either qualitative, quantitative or mixed methods approach (empirical data); (d) studies conducted in Southeast Asia; (e) published in the last 8 years (2013–2021) and (f) pertaining to NSSI. Articles published from 2013 onwards were included given that NSSI was only recognized as a distinct disorder in DSM-5.
Furthermore, studies were excluded in line with the following exclusion criteria: (a) theoretical papers (reviews, meta-analysis and discussion papers); (b) published in languages other than English; (c) non-peer reviewed articles (e.g., books, book chapters, conference abstracts, editorials and dissertations); (d) published before 2013; (e) assessing other mental disorders which do not involve NSSI (e.g., self-injuries related to neurological or developmental abnormalities) or (f) self-poisoning. The authors conducted a comprehensive inspection of the articles’ titles and abstracts. Self-injury related to neurological or developmental abnormalities (e.g., autism spectrum disorder, Lesch-Nyhan syndrome, Tourette’s syndrome and intellectual disability) are not considered as NSSI as they involve a pattern of repetitive stereotypies or caused by another mental condition as explained in DSM-5. As NSSI in DSM-5 is restricted to immediate and evident injuries on one’s skin, self-poisoning is not deemed as NSSI even if it is done with the absence of suicidal intent.
Search Strategy
A thorough literature review was performed using Scopus, Web of Science, PubMed and CINAHL in January 2022. The search terms used to identify relevant articles are displayed in Table 1.
Search Terms Used.
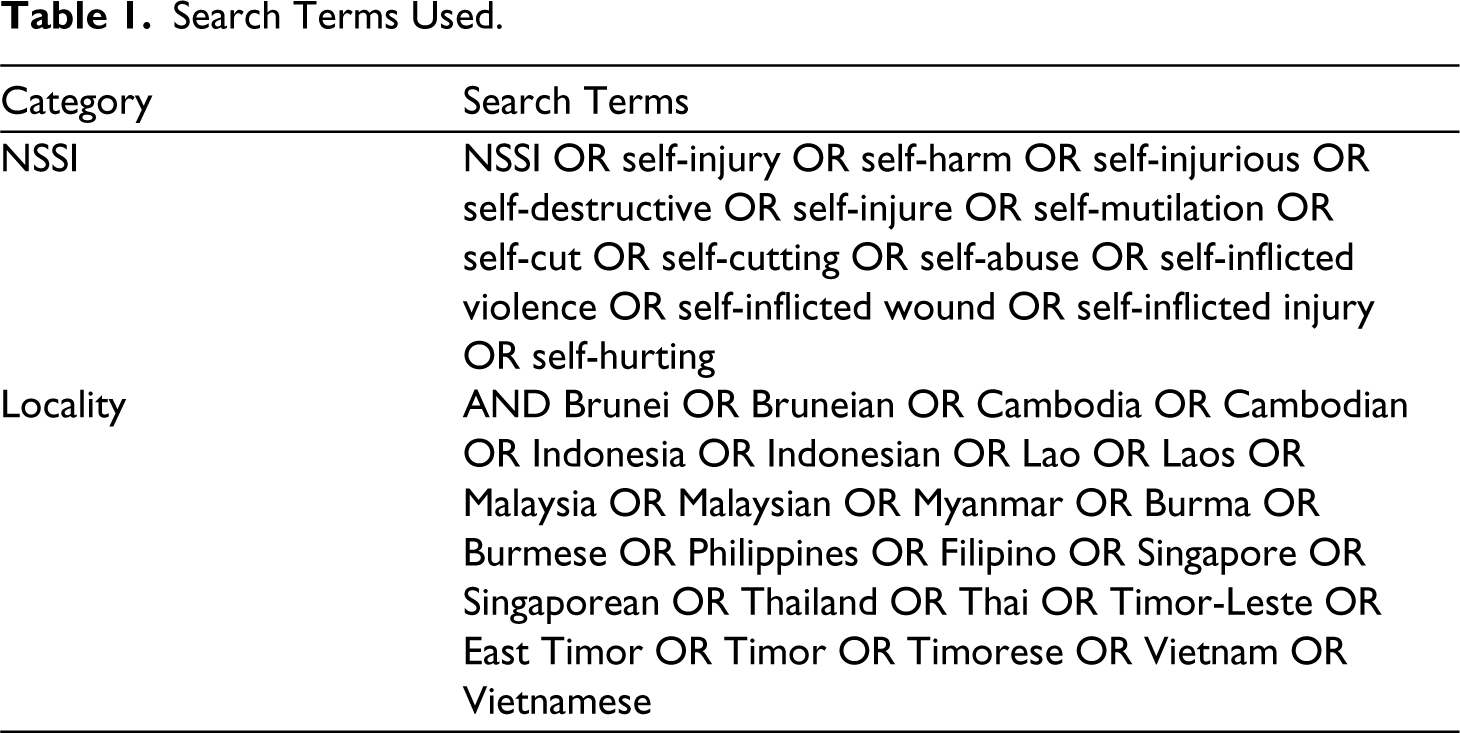
Search Terms Used.
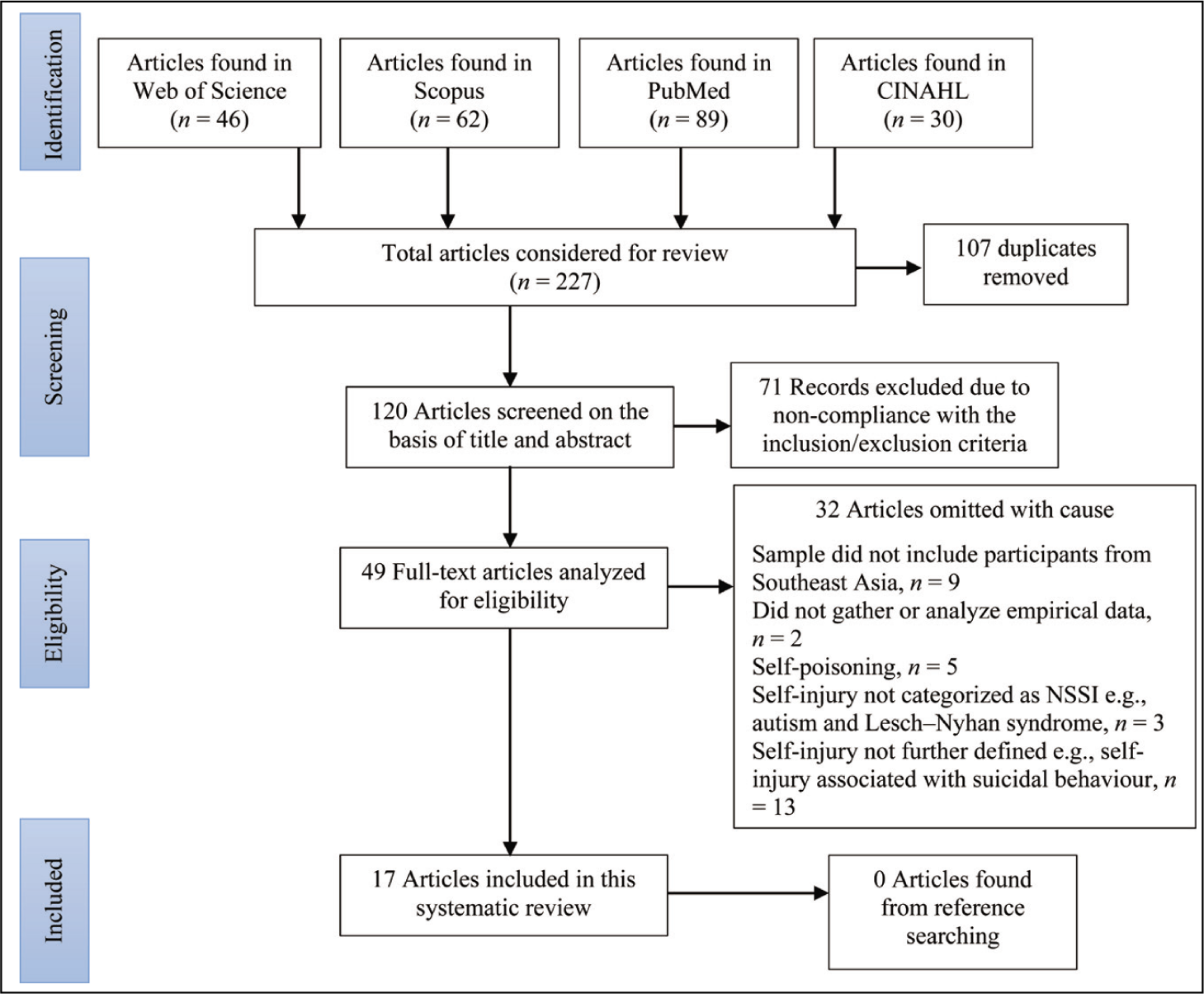
Figure 1 displays the selection procedure in accordance with PRISMA guidelines (Shamseer et al., 2015). After filtering through the duplicates and studies meeting the aforementioned inclusion and exclusion criteria, the search produced 17 studies which are included in this review.
PRISMA Flowchart of the Literature Review Procedure.
Synthesis
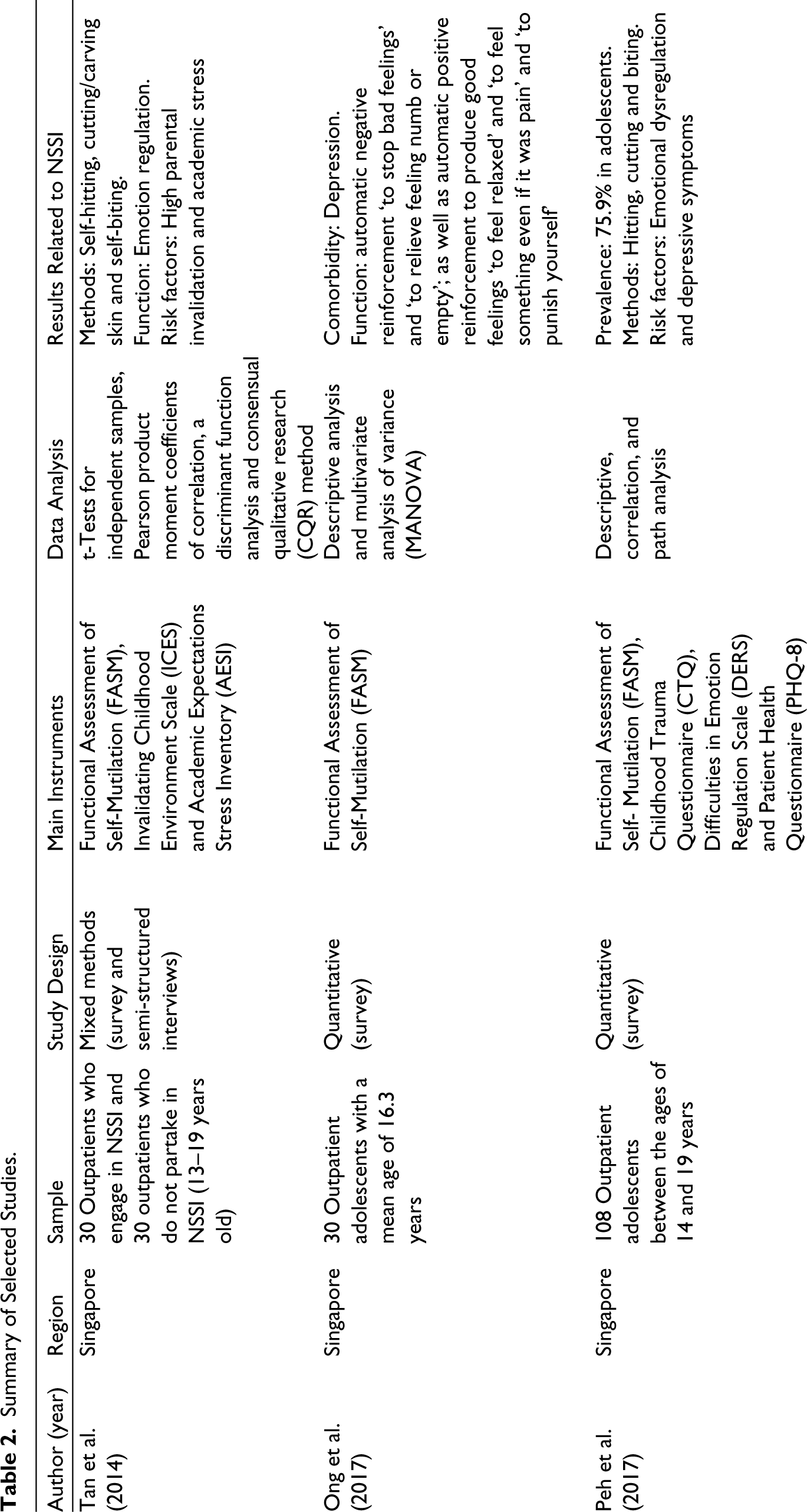
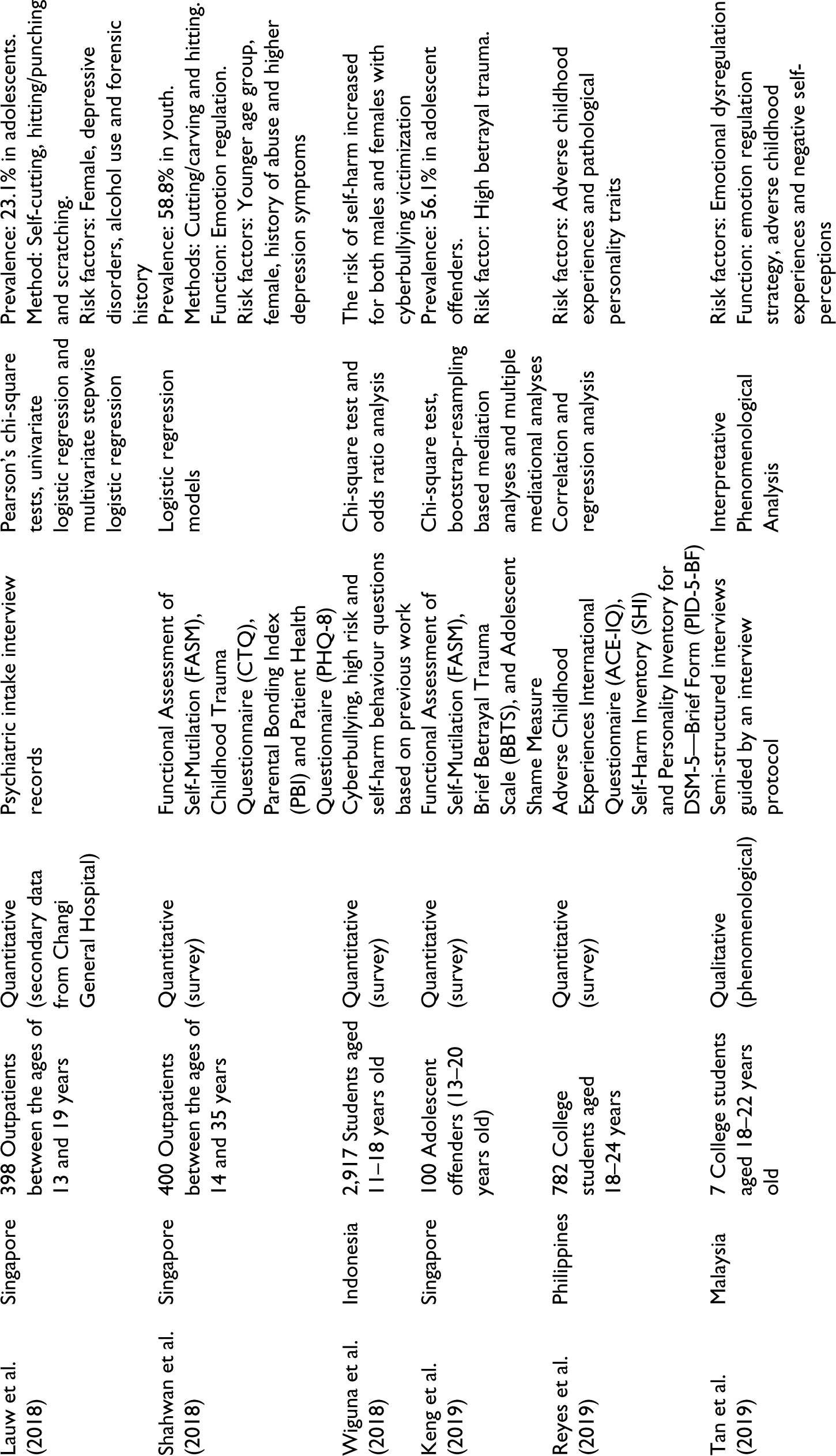
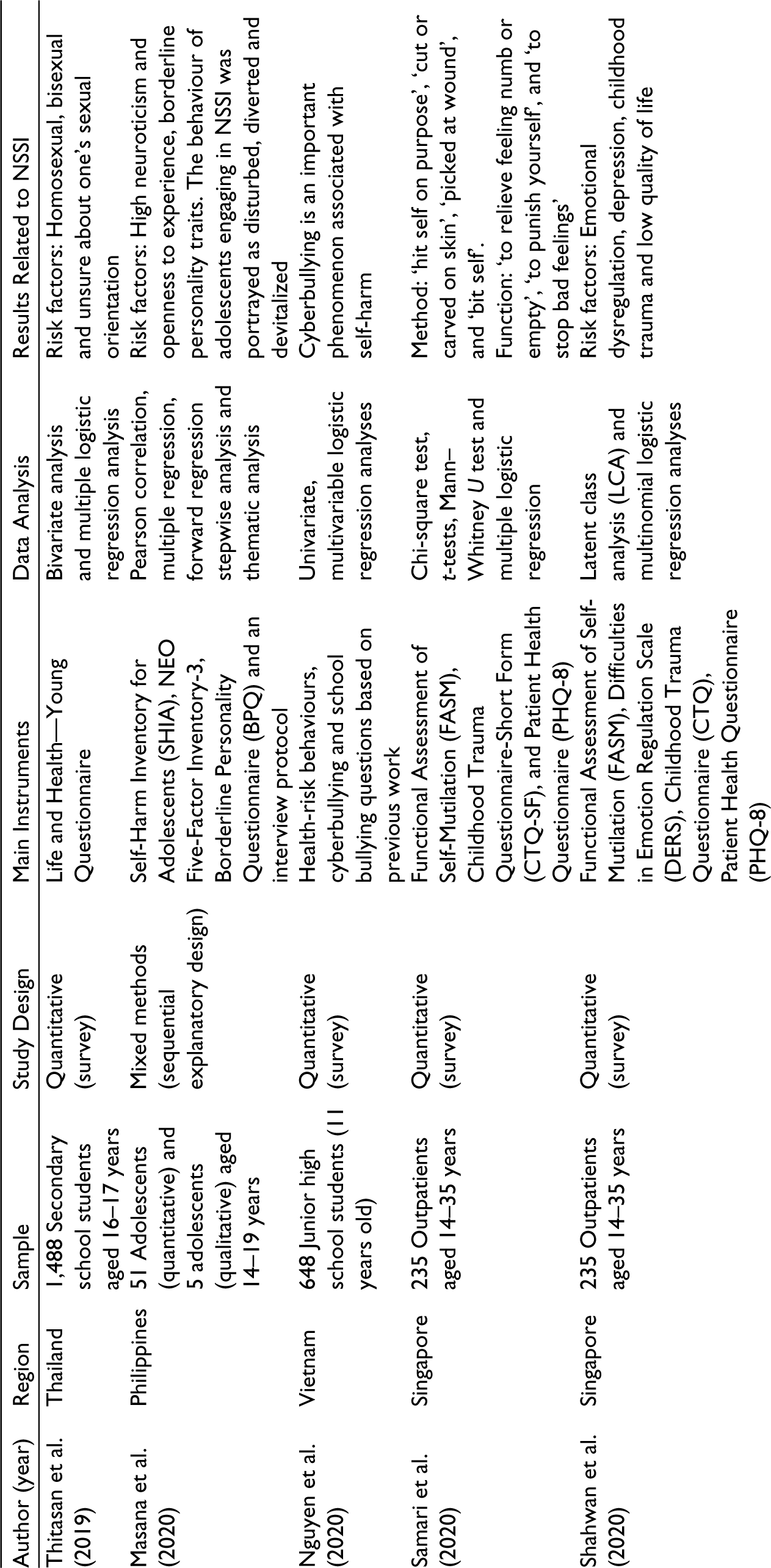
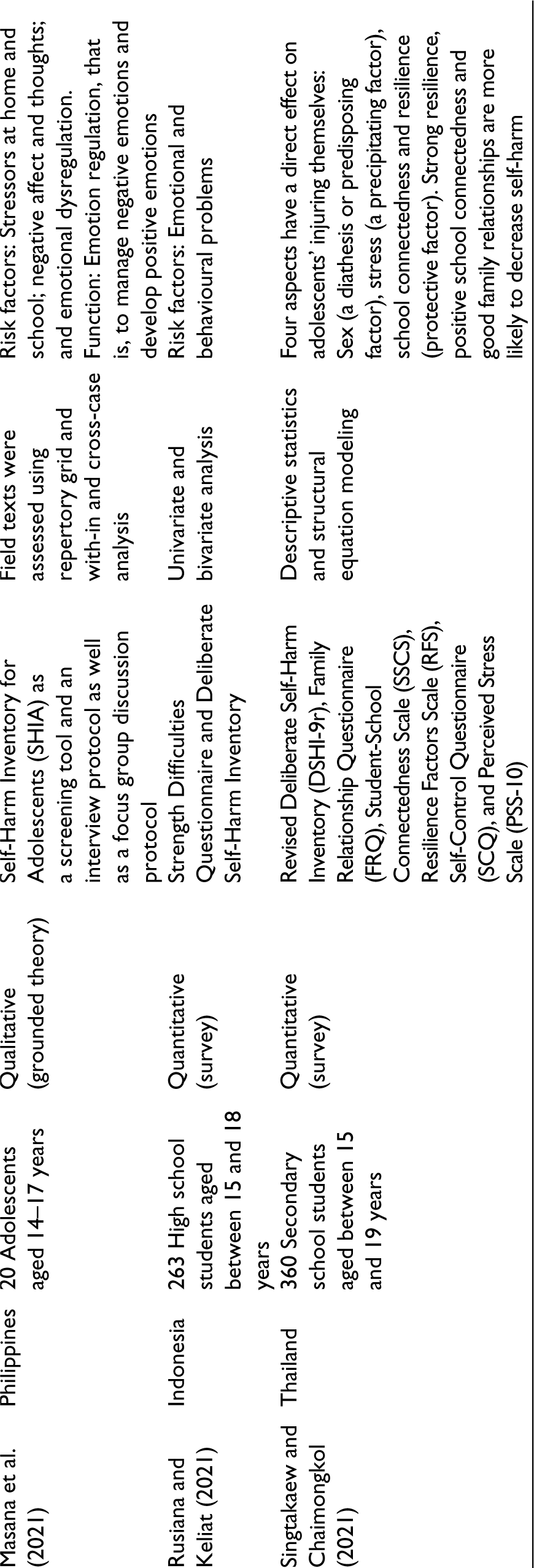
The key characteristics from the 17 studies are tabulated in Table 2. Findings were synthesized to provide a summary of the available data regarding the sample description, study design, data analysis and findings.
Summary of Selected Studies.
Quality Assessment
The quality assessment phase was conducted to ensure that the methodologies and data analyses of the identified studies were satisfactory. The authors used the mixed-method appraisal tool (MMAT) by Hong et al. (2018) to critically assess the selected studies. The MMAT outlines a set of criteria to provide an overall quality score for each selected study and requires at least two independent reviewers to conduct the quality appraisal (Hong et al., 2018). All reviewers must mutually agree on the quality of each study in order for the selected studies to be incorporated in this article.
For qualitative studies, the criteria include suitability of qualitative approach to answer research questions; suitability of data collection methods; findings being adequately derived from the data; interpretation of results and cohesion between data sources, collection, analysis and interpretation. While the criteria for quantitative (descriptive) approach include sampling strategy suitability; representativeness of sample; suitability of measurements; risk of nonresponse bias and suitability of statistical analysis. Whereas the criteria for mixed methods approach include rationale for using mixed methods design; effectiveness of the different components of the study being integrated to answer the research question; interpretation of data collected; divergences and inconsistencies adequately addressed and adherence to quality of each of the involved methods.
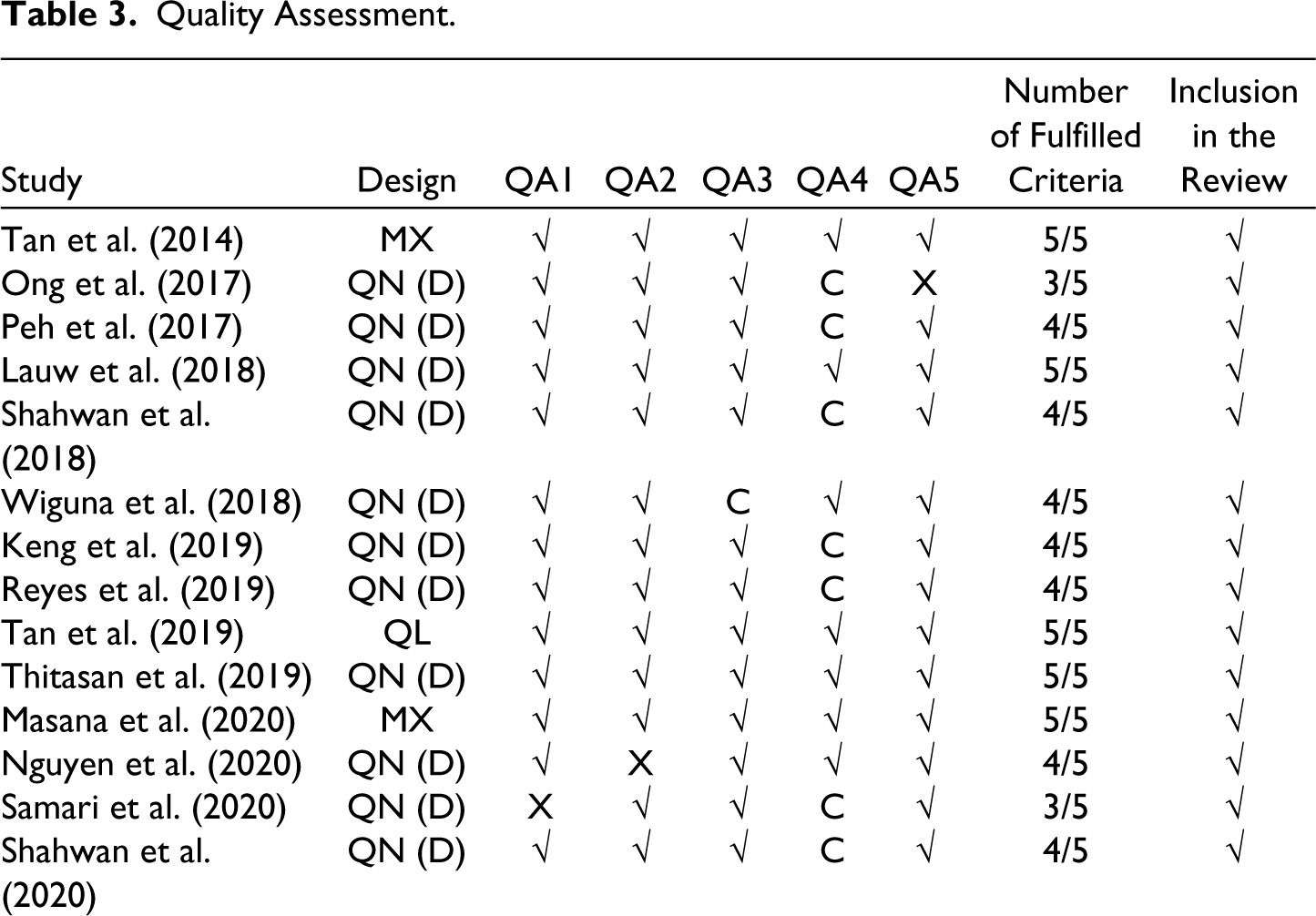
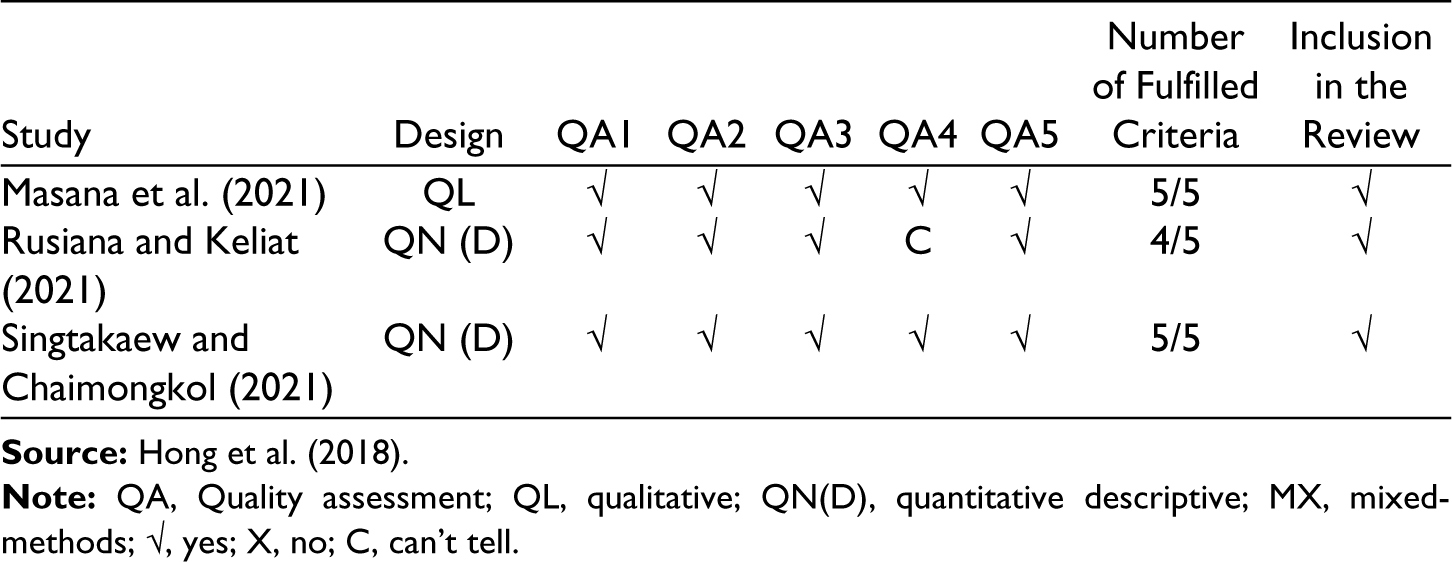
Of the 17 identified studies, the full texts were collected and scrutinized by three independent reviewers to ensure that the studies had suitable research questions, sound research designs and underwent rigorous analysis. Guided by MMAT, the three reviewers assessed the studies in accordance with the five criteria with three options when reporting their responses, that is, ‘yes’, ‘no’, or ‘can’t tell’. Only studies that met at least three criteria were included in this review. All the reviewers mutually agreed on the appraisal of each criterion. In total, seven studies fulfilled all the criteria, eight studies fulfilled four out of five criteria and two studies fulfilled at least three criteria (please see Table 3). Hence, all of the 17 remaining articles were suitable to be reviewed.
Quality Assessment.
The selected studies were conducted in Singapore (n = 8), the Philippines (n = 3), Indonesia (n = 2), Thailand (n = 2), Malaysia (n = 1) and Vietnam (n = 1). There were no studies selected from Brunei, Cambodia, Myanmar, Laos and East Timor.
Prevalence of Nonsuicidal Self-injury
The overall prevalence rates of NSSI among community samples fall between 7.1% and 11.4% (Nguyen et al., 2020; Rusiana and Keliat, 2021). Among clinical samples, prevalence rates of NSSI ranged between 20.7 and 75.9% (Lauw et al., 2018; Peh et al., 2017; Reyes et al., 2019; Shahwan et al., 2018). The onset age of NSSI most frequently occurs in early adolescence, between 13 and 16.5 years old (Shahwan et al., 2018; Tan et al., 2014). The most common methods of NSSI were self-hitting and self-cutting (Lauw et al., 2018; Peh et al., 2017; Samari et al., 2020; Shahwan et al., 2018; Tan et al., 2014). Some of the less common methods of NSSI include scratching, biting, head banging and burning (Lauw et al., 2018; Peh et al., 2017; Samari et al., 2020; Shahwan et al., 2018; Tan et al., 2014). There were a handful of studies that reported the average frequency of NSSI was between 2 and 25 times over a 12-month period (Keng et al., 2019; Peh et al., 2017; Samari et al., 2020; Shahwan et al., 2018, 2020; Tan et al., 2014).
Nonsuicidal Self-injury Function
NSSI is regularly performed as an emotion regulation strategy (Ong et al., 2017; Shahwan et al., 2018; Singtakaew & Chaimongkol, 2021; Tan et al., 2014, 2019). Individuals often resort to NSSI because they are unable to control their intense emotions or calm themselves down. After the NSSI episode, they often reported a sense of relief and calmness (Masana et al., 2020; Tan et al., 2019). It is a form of escape from their painful emotions and frustrations. Negative emotions (e.g., sadness, anxiety, anger, frustration or loneliness) tend to occur before the act of self-injury, followed by a surge in positive emotions (e.g., relief) and decline in negative emotions after the act.
In summary, there are four main functions of NSSI which are (a) automatic negative reinforcement; (b) automatic positive reinforcement; (c) social positive reinforcement and (d) social negative reinforcement. Majority of the studies endorsed the automatic negative reinforcement (to reduce or stop negative feelings, relieve feeling numb and empty) (Masana et al., 2021; Ong et al., 2017; Samari et al., 2020; Shahwan et al., 2018; Tan et al., 2014) and automatic positive reinforcement (to produce positive feelings, to feel relaxed and to feel something even if it is pain) (Masana et al., 2020; Ong et al., 2017; Shahwan et al., 2018; Tan et al., 2014).
For some, NSSI is a form of self-punishment (Ong et al., 2017; Samari et al., 2020; Shahwan et al., 2018). Those who engage in NSSI often equate setbacks and problems with personal failure and weakness (Tan et al., 2019). Stressful events in their lives triggered self-blame and self-hatred, and NSSI is viewed as a form of self-retribution. Self-critical individuals believe that they are complete failures and thus should be punished. These individuals view NSSI as an expression of anger and derogation towards themselves and feel purified after engaging in NSSI. After NSSI, their negative emotions were reduced, while positive emotions increased which would support both automatic positive and negative reinforcement. In short, individuals engage in NSSI because they seek to punish themselves as a way of redeeming themselves, at least in their own eyes.
NSSI was also linked with regaining control indicating social positive reinforcement (Ong et al., 2017; Tan et al., 2014, 2019). By self-injuring, they had control of the method, severity and setting of the act. When focusing on the physical pain or act of NSSI, they were able to temporarily forget their current problems and distressing memories. NSSI serves as a means of converting emotional pain to physical pain (Tan et al., 2014). Apart from that, there is a very small group of individuals who endorsed social negative reinforcement, specifically to remove negative consequences as a function of NSSI, for example, to avoid schoolwork, other activities, certain people or punishments (Ong et al., 2017; Tan et al., 2014).
Many reported self-injury as a reliable coping method that helps them to deal with intense emotions (Tan et al., 2019). While some participants expressed their self-injury episodes as pain free (Masana et al., 2020), others describe their experience as physically painful, but it is performed to cope with emotional pain (Tan et al., 2019). Over time, they became habituated with NSSI (Masana et al., 2021). Consequently, they increased the frequency and intensity of NSSI. In some cases, they switched to more destructive forms of NSSI (Tan et al., 2014).
It is important to note that individuals who engage in high-frequency NSSI in the past year were more likely to partake in more than three methods of self-injury and endorse all of the functions of self-injury (Shahwan et al., 2020). This suggests that these individuals may have emotion regulation and interpersonal skill deficits, thus turning to self-injury often. On the contrary, individuals who engage in low-frequency NSSI in the past year had fewer methods of self-injury and a low endorsement of using self-injury to fulfil interpersonal and intrapersonal functions (Shahwan et al., 2020). This implies that these individuals do not use self-injury as their usual coping repertoire. Nevertheless, individuals from both groups (high- and low-frequency NSSI) will benefit from learning diverse coping strategies such as mindfulness practice, distress tolerance skills, self-compassion work and conflict management.
Aetiology of Nonsuicidal Self-injury
Young people engaging in NSSI reported struggling with intense emotions and stress (Masana et al., 2020, 2021; Tan et al., 2019). Due to the overwhelming distress, they often feel helpless and lack means for coping. The aetiology of NSSI can be split into two main groups, that is, individual (emotional dysregulation, low self-esteem, gender and psychiatric disorders) and environmental (childhood maltreatment, childhood neglect, parental invalidation and academic stress). The combination of multiple stressors is also a risk factor for NSSI (Tan et al., 2019).
Experience with NSSI is most commonly linked to childhood maltreatment such as being bullied at school (Masana et al., 2021; Reyes et al., 2019; Rusiana & Keliat, 2021; Tan et al., 2019), emotional abuse (Keng et al., 2019; Peh et al., 2017; Reyes et al., 2019; Shahwan et al., 2018, 2020; Tan et al., 2014), physical abuse (Keng et al., 2019; Peh et al., 2017; Reyes et al., 2019; Rusiana & Keliat, 2021; Shahwan et al., 2018, 2020; Tan et al., 2019) and sexual abuse (Reyes et al., 2019; Shahwan et al., 2018, 2020). While a handful of studies found parental emotional neglect (Reyes et al., 2019; Shahwan et al., 2020) and physical neglect (Shahwan et al., 2020) as significant predictors of NSSI. It is worth noting that cyberbullying is also associated with self-injury (Nguyen et al., 2020; Wiguna et al., 2018). In fact, cyberbullying can have more devastating and longer-lasting effects. As the harassment occurs electronically, it can be communicated to a larger audience in a shorter span of time. Cyberbullying victims are exposed to bullying at school as well as at home. As a result, the home is no longer seen as a safe zone and victims constantly feel helpless. This is also true for victims of physical and emotional abuse perpetrated by parents.
Several studies reported academic stress as a trigger for NSSI (Masana et al., 2020, 2021; Tan et al., 2014, 2019). Academic stress can be divided into parental expectations and self-expectations. Young people reported feeling pressured by their parents to constantly excel in studies (Tan et al., 2014). Some parents obsess over their child’s academic achievement so much that the need for obtaining the highest score overtakes everything else including the child’s mental health. This leads to stress, anxiety and fear of failing among students. NSSI can be the outcome of excess pressure. Besides that, it is becoming more common for people to set extremely high expectations of themselves. The pressure to be perfect can be overwhelming. Most of the individuals who engage in NSSI have a negative self-perception and often blame themselves when they fail to meet their expectations (Tan et al., 2019). High self-expectations in academia may have stemmed from initial parental pressures. Parents tend to show subtle expectations like facial expressions of disappointment when their children do not meet their expectations (Tan et al., 2014).
Furthermore, individuals who partake in NSSI constantly reported low self-esteem (Masana et al., 2020; Tan et al., 2014). Concepts aligned with low self-esteem are also endorsed as motives for self-injury. Some examples include self-punishment (Ong et al., 2017; Samari et al., 2020; Shahwan et al., 2018), disappointment with oneself (Tan et al., 2019), negative self-perceptions (Tan et al., 2019) and feelings of shame (Keng et al., 2019; Tan et al., 2014, 2019). This indicates negative thought patterns towards oneself are linked to both the development and maintenance of NSSI. For instance, young people engaging in NSSI often report adverse thoughts and effects immediately preceding the NSSI act (Masana et al., 2020).
Moreover, NSSI may serve as an emotion regulation function, stemming from poor emotion skills (i.e., emotional dysregulation) (Peh et al., 2017; Shahwan et al., 2020; Tan et al., 2019). Most young people disclosed poor emotional awareness and difficulty identifying their emotions (Tan et al., 2019). Furthermore, many reported difficulties expressing their emotions to their family members and often kept their feelings to themselves (Tan et al., 2019). Some reported that they needed to display a certain face irrespective of their actual feelings and that expressing adverse feelings openly was a sign of weakness (Tan et al., 2019).
Besides that, Tan et al. (2014) found parental invalidation to be a predictor of NSSI. Parental invalidation refers to the communication between a parent and his/her child wherein the child’s feelings are not acknowledged. For instance, a parent not listening or trying to comprehend his/her child’s feelings. Interestingly, young people who partake in NSSI were highly likely to have parents with lower educational attainment when compared to those who do not partake in NSSI (Tan et al., 2014). Perhaps, parents with higher educational attainment practice more egalitarian parenting styles; thus, they tend to be aware of, acknowledge and address their children’s feelings.
In addition, young people who identify as LGBTQI+ (lesbian, gay, bisexual, trans, queer, questioning and intersex) are at a greater risk of partaking in NSSI. Thitasan et al. (2019) reported that self-injury was highest among homosexuals and lowest among heterosexuals. Furthermore, the latter study revealed that self-injury was more often reported by homosexual, bisexual and unsure young people. This trend may be due to the stigma and discrimination experienced by these youth, placing them at an elevated risk for poor mental health outcomes. The findings obtained from studies focusing on only two sexes (males and females) have been for the most part heterogenous. A study by Singtakaew and Chaimongkol (2021) demonstrated that males are more predisposed to self-injury, but females were more inclined to engage in self-injury when they feel stressed. Another study by Tan et al. (2014) reported no gender differences among young people who partake in NSSI. Nonetheless, Lauw et al. (2018) and Shahwan et al. (2018) posited that females have a greater tendency to self-injure than males.
Apart from that, NSSI is known to co-occur with other psychiatric disorders. The most common disorder being depressive disorders (Lauw et al., 2018; Masana et al., 2020; Ong et al., 2017; Peh et al., 2017; Samari et al., 2020; Shahwan et al., 2018, 2020), followed by adjustment disorders (Lauw et al., 2018; Peh et al., 2017; Samari et al., 2020; Shahwan et al., 2018) and anxiety disorders (Lauw et al., 2018; Ong et al., 2017; Peh et al., 2017; Samari et al., 2020; Shahwan et al., 2018). Other psychiatric disorders include borderline personality disorder (Masana et al., 2020), acute stress disorder (Ong et al., 2017), conduct disorder (Ong et al., 2017) and eating disorders (Lauw et al., 2018).
Consequences of Nonsuicidal Self-injury
Many individuals felt guilty and shameful for engaging in NSSI (Tan et al., 2019). They feel incompetent for not being control of their emotions. Interestingly, this potent mixture of cocktails (guilt, shame and needing to release tension) leads them to the act of NSSI again. Self-injury turns into a vicious cycle that becomes difficult to stop. This compulsive behaviour also prevents them from learning more effective coping strategies.
Although NSSI helps those who self-injure feel better, they view NSSI as a negative and shameful behaviour. Many of them reported performing NSSI in secret and carefully hiding their injuries and scars in fear of how others would react (Tan et al., 2019). They do not want their loved ones to worry or feel hurt. Ultimately, having to carry this secret constantly may lead these young people feeling lonelier and more isolated. NSSI itself is an isolating act, often done alone. It has a way of both causing feelings of loneliness and of reinforcing them. As a result, NSSI can go as long as it does, sometimes lasting decades.
Moreover, prolonged self-injury may lead to suicidal behaviour (Samari et al., 2020; Shahwan et al., 2018). Young people who partake in prolonged NSSI may develop a heightened threshold for pain and a reduced fear of death. NSSI can escalate into suicidal behaviour when those who self-injure feel that self-injury is no longer an effective coping method, when it ceases to offset the negative feelings triggered by trauma or intense stress.
Discussion
The objective of this article was to examine existing studies and provide an overview of NSSI in Southeast Asia. There is general belief that self-injury begins in adolescence, with a main onset age of 13–16.5 years old (Shahwan et al., 2018; Tan et al., 2014). Prevalence rates are high in community samples, between 7.1 and 11.4% (Nguyen et al., 2020; Rusiana & Keliat, 2021) and even higher in clinical samples, between 20.7% and 75.9% (Lauw et al., 2018; Peh et al., 2017; Reyes et al., 2019; Shahwan et al., 2018). All the studies in this article centred around youth between the age of 14 and 35 years old. Regrettably, research on NSSI in children, older adults and the elderly in Southeast Asia are virtually non-existent. As NSSI is often perceived as something youngsters do, older adults engaging in NSSI may feel ashamed to seek professional help. Therefore, clinicians and mental health researchers should conduct more studies on NSSI among other age groups to shed light and bring about awareness about NSSI.
In Southeast Asia, there were several different terms used to define NSSI such as deliberate self-harm (Lauw et al., 2018; Masana et al., 2020; Samari et al., 2020; Shahwan et al., 2018; Singtakaew & Chaimongkol, 2021), self-harm (Nguyen et al., 2020; Peh et al., 2017; Thitasan et al., 2019; Wiguna et al., 2018), self-injury (Rusiana & Keliat, 2021) and self-hurting behaviour (Wiguna et al., 2018). It is essential to use one clear terminology (i.e., NSSI) to describe NSSI to avoid confusion and enhance understanding. Additionally, the DSM-5 officially recognized NSSI as a psychiatric nomenclature. Some of these terms may be pejorative or unacceptable to certain individuals. For example, the term deliberate self-harm, self-harm and self-injury may refer to self-inflicted injuries irrespective of suicidal intent. While, ‘self-mutilation’ may seem derogatory, stigmatizing and even sensationalistic when referring to the behaviour (Walsh, 2012). Also, self-mutilation may be restricted to cutting, albeit NSSI includes other methods, for example, burning, banging, scratching, hitting, etc.
Moreover, the most common function for NSSI is that it serves as an emotion regulation strategy (Ong et al., 2017; Shahwan et al., 2018; Singtakaew & Chaimongkol, 2021; Tan et al., 2014, 2019). Western societies emphasize open expression of emotions in the interest of individual rights (Lim, 2016). In contrast, Asians emphasize greater restraint or control of emotions in the interest of maintaining group harmony, making it difficult for them to process emotional distress (Lim, 2016). Constant suppression of emotional expression may exacerbate psychological distress, and for some, NSSI may become a method for communicating emotional distress. Unfortunately, the value placed on emotional restraint or control may also contribute to the stigma linked to mental disorders in many Southeast Asian cultures and the subsequent avoidance of mental health treatment.
In terms of the aetiology of NSSI, emotional abuse (Keng et al., 2019; Peh et al., 2017; Reyes et al., 2019; Shahwan et al., 2018, 2020; Tan et al., 2014), physical abuse (Keng et al., 2019; Peh et al., 2017; Reyes et al., 2019; Rusiana & Keliat, 2021; Shahwan et al., 2018, 2020; Tan et al., 2019) and academic stress (Masana et al., 2020, 2021; Tan et al., 2014, 2019) were significantly associated with NSSI. NSSI is common among children of parents who frequently use criticisms and verbal put downs (Tan et al., 2014). Many Asian parents express love as disapproval. These parents believe that they are doing their children a favour by pointing out their children’s flaws. Parents often believe that if their children were more aware of their shortcomings, they would be more motivated to fix them.
Apart from that, Asian culture values respect for authority and elders; thus, parents are inclined to use more orders and try to control their children’s behaviour more openly than Western parents (Russell et al., 2010). Southeast Asian parents tend to use authoritarian parenting style and corporal punishment at home (Chan, 2018; Cheung & Lim, 2021). Though parental physical abuse is different from corporal punishment, past research revealed that individuals who experienced corporal punishment are at an increased risk of also having experienced parental physical abuse (Fréchette et al., 2015). Likewise, recent research showed that authoritarian parenting style is linked to lower child emotion regulation skills (Haslam et al., 2020). This explains why individuals engaging in NSSI have difficulties regulating emotions. Authoritarian parenting is also related to lower self-esteem (Jadon & Tripathi, 2017), more negative self-talk (Chong & Chan, 2015) and greater depressive symptoms (King et al., 2016) among adolescents, which are all risk factors of NSSI.
Furthermore, Asian parents often show their love through instrumental support in meeting their children’s basic and educational needs (Russell et al., 2010). They typically put their children’s needs before their own. For instance, they make sacrifices by taking up multiple jobs for their child’s education expenses and diligently save to fund their children’s college education. This is because they place a lot of importance on education and academic success (Russell et al., 2010). This can be extremely stressful for children as they feel pressured to attain academic success up to their parents’ expectations. This is a unique cultural dimension in which academic stress may result in NSSI, where it is used as a method for coping or regaining control.
Majority of the studies in this review defined gender as male or female. Only Thitasan et al. (2019) permitted the participants to choose their sexual orientation as homosexual, bisexual or unsure. Though visibility and acceptance of LGBTQI+ in Southeast Asia have grown in recent years, some countries continue to criminalize same-sex relations or individuals with different gender expressions, for example, Brunei, Malaysia and Myanmar. LGBTQI+ rights in Southeast Asia are limited in comparison to Western countries. There is blatant discrimination and insufficient legislative protections for persons whose gender identities are non-conforming. As a result, LGBTQI+ people experience greater levels of social stress (e.g., stigma, victimization, prejudice and discrimination), resulting in detrimental mental health outcomes (e.g., depression and anxiety). These individuals often engage in NSSI to cope with tension caused by LGBTQI+ identity and/or homophobia. In Southeast Asia, both LGBTQI+ and NSSI are culturally tabooed and religiously proscribed, making it even more difficult to seek professional help. Hence, further research looking into the various gender identities and NSSI are needed to address this knowledge gap and encourage them to seek professional help in Southeast Asia.
Before the twenty-first century, the general belief was that NSSI is more common in females. This was stemmed from early research that suggested that females engage in NSSI more often than males (Favazza, 1992; Graff & Mallin, 1967). In fact, this behaviour is not gender-specific and affects everyone. Females tend to seek professional help more than males, with respect to mental health issues (Sagar-Ouriaghli et al., 2019). Furthermore, females are more inclined to disclose their struggles to others. With males, it happens to a lesser degree due to the misconception that self-harm is predominantly a female issue. There is also a deluded expectation (especially in Asia) of men needing to be strong and not expose their vulnerability. All these features in tandem make it more challenging for men to come forward. Consequently, mental health professionals and NSSI survivors should work towards destigmatizing NSSI through creating more awareness in order for more survivors (especially males) to seek help.
Besides that, the most common instrument used to measure self-injury was the Functional Assessment of Self-Mutilation (FASM) (Keng et al., 2019; Ong et al., 2017; Peh et al., 2017; Samari et al., 2020; Shahwan et al., 2018, 2020; Tan et al., 2014). Nevertheless, FASM includes self-tattooing as a type of self-injury which is excluded in the proposed criteria of NSSI in DSM-5. The FASM showed good structural validity, construct validity and internal consistency but the reliability, cross-cultural validity and criterion validity are relatively unknown (Faura-Garcia et al., 2020). Comparing NSSI across cultures and languages presents the dilemma of adapting the questionnaire to the specific culture without compromising the integrity of the questionnaire. Researchers should consider developing a tailormade NSSI questionnaire that is applicable for Southeast Asians that includes cultural nuances such as parental invalidation, academic stress and religiosity.
Strengths and Limitations
Overall, findings from the studies in this review support the view of a more culturally nuanced interpretation of NSSI in Southeast Asia. The current review includes both males and females partaking in NSSI and thus, addresses the misconception in previous literature that NSSI is a condition that primarily affects females. This is the first systematic review on NSSI in Southeast Asia. This article sought to understand the prevalence, main functions and causes of NSSI. The most noticeable limitation in NSSI research in Southeast Asia is the paucity of research regarding effective treatment and preventive programs. Even globally, there is no solid evidence on the effectiveness of any specific treatment for self-injury. As it is clearly apparent that many Southeast Asians struggle with NSSI, further research should be conducted on the treatment and intervention strategies for NSSI. Besides that, there were only two qualitative studies (Masana et al., 2021; Tan et al., 2019) and two mixed-methods studies (Masana et al., 2020; Tan et al., 2014) from Southeast Asia. Qualitative studies allow for a deeper dialogue on NSSI and uncover the NSSI experience in depth. Also, NSSI is a complex behaviour that is often done in secret; thus, it may be better for researchers to undertake more qualitative studies to elicit true responses that are sensitive in nature.
Recommendations for Practice
As prolonged NSSI may lead to suicidal behaviour, intervention strategies that can lower suicidal risk should be implemented for youth who self-injure as soon as possible. Schools and colleges should implement preventive interventions that focus on effectively dealing with negative emotions. Peer groups and mentor programs can also be developed for youth as supportive friends are known to be protective factors against NSSI. Last, culturally responsive parenting programs are needed to improve parent-child communication, grant autonomy to children and enhance parental empathy.
Conclusion
This article provides an overview on NSSI in Southeast Asia. Growing prevalent rates that are seen in youth is of increasing concern in both clinical and educational settings. Public and clinical mental health interventions must be emphasized along with improving the social determinants of NSSI. The paucity of studies on NSSI with high heterogeneity calls for further research in exploring NSSI which may inform better mental health practice and policymaking in Southeast Asia. More studies may be conducted to look into intergroup differences and how cultural factors relate to the NSSI experience.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.