
Abstract
Introduction:
Malignant pleural effusion (MPE) is the second most common cause of exudative pleural effusion with a reduced life expectancy. Hence, diagnosing MPE is important for early intervention and management to improve survival. Histopathological examination of pleural fluid (PF) has an accuracy of 40% to 87% for diagnosing MPE[8]. When the malignancy is not diagnosed, a closed or thoracoscopic pleural biopsy is performed to establish the diagnosis, but a closed pleural biopsy adds only 8% to the overall yield. Hence, pleural effusion remains undiagnosed in situations when the patient refuses the thoracoscopic biopsy or when the test is unavailable. Cancer ratio (CR), that is, the ratio of serum Lactate Dehydrogenase (LDH) to pleural fluid Adenosine Deaminase (ADA) and Cancer Ratio plus, that is, the ratio of Cancer Ratio to pleural fluid lymphocyte count are markers which may be a ‘forewarning’ to patients who are not diagnosed by cytology but later confirmed to have MPE. The aim in this study is to test the diagnostic potential of CR plus (CR/PF lymphocyte count) in identifying MPE from other effusions. (CR = serum LDH/PF ADA)
Results:
Among the total of 110 patients included in the study, the mean of CR plus is 50.63 ± 30.772 among MPE and 12.45 ± 18.08 among non-MPE. At a cut-off of 20.5, the sensitivity and specificity of CR plus are 95.1% and 92.7%, respectively.
Conclusion:
Triage of patients presenting with exudative lymphocytic but diagnostically inconclusive pleural effusion can be facilitated by using biochemical markers such as the CR and CR plus, which are simple, affordable and widely available.
Introduction
Pleural effusion is referred to as an abnormal buildup of pleural fluid (PF) in the pleural space. PF begins to accumulate whenever the absorption is reduced or the production is increased. All pleural effusions can be classified as either transudative or exudative. Transudative effusions occur when systemic mechanisms regulating the generation and absorption of PFs are changed, leading to PF accumulation. An exudative effusion occurs from increased capillary permeability, which is a characteristic of an inflammatory reaction. The evaluation of pleural effusion begins with confirmation of PF and classification into transudative or exudative effusions. Light’s criteria serve as a standard tool for this differentiation and assist in narrowing the diagnosis of pleural effusion.
Malignant pleural effusion (MPE) has been recognised as the second leading cause of exudative pleural effusion.[1] It is the accumulation of fluid with malignant cells in the pleural space between the lung and the chest wall.[2] Reduced life expectancy is linked to the presence of malignant cells in the PF and/or pleural tissue, which verifies the existence of disseminated or advanced malignancy. A recent study found that patients with MPE have a 5.5-month survival rate for lung cancer,[3] whereas overall survival for all cancer types varied from 3 to 12 months, depending on the patient’s comorbidities and the kind of tumour.[4]
Hence, diagnosing MPEs is necessary for early intervention and management to improve survival. PF cytology can offer helpful diagnostic, prognostic and therapeutic information. According to reports, the accuracy of cytological diagnosis for MPEs ranges from 40% to 87%.[5]
However, pleural biopsy is still the gold standard, but repeated biopsy or longer follow-up is typically needed if the first biopsies reveal inflammation, but its invasive nature adds to the limitation. Closed pleural biopsy contributes to only about 8% of the total diagnostic yield.[6] A number of more sophisticated tests have been created recently to identify cancer in patients who present with pleural effusion. Examples include protein microarray technology to distinguish between malignant and tuberculosis effusion and measuring the tumour markers CA15–3, cyfra 21–1, CA125 and CEA in PF. These tests have limitations of cost and availability.
Recently, in a study by Verma et al. the authors came up with new biochemical markers, cancer ratio (CR), that is, the ratio of serum LDH to PF ADA and CR plus, that is, the ratio of CR to PF lymphocyte count.[7,8] These markers may act as a ‘forewarning’ to individuals with negative cytology who are later confirmed to have MPE. It was concluded in their study that CR and CR plus have high sensitivity and specificity in identifying MPE.
The present study was conducted to evaluate the potential of CR plus in identifying malignant effusions from other effusions.
*CR plus = CR/PF lymphocyte count
*CR = Serum LDH/PF ADA
Aims and Objectives
Aim
To study the diagnostic potential of CR plus (CR/PF lymphocyte count) in identifying malignant effusion from other effusions (where CR = serum LDH/PF ADA).
Objectives
To assess the role of CR plus in recognising MPE from other types of pleural effusions.
To prospectively compare patients’ diagnosis with outcomes of CR and CR plus.
Methodology
A prospective observational study was done on patients with exudative pleural effusions presenting to a tertiary care centre in coastal Andhra between August 2022 and June 2024. All the patients attending the hospital with pleural effusions were examined and investigated and selected based on the criteria given below. The sample size taken for the study is 110 which is calculated based on the formula n = 4pq/d2 and where p is expected prevalence, q = 1-p, d is allowable error.
Inclusion Criteria
All in-patients diagnosed with exudative pleural effusions based on Light’s criteria.
Exclusion Criteria
Patients not willing for study
Patients aged <18 years age
Exudative effusions diagnosed after diuretic therapy
Patients who are hemodynamically unstable
Procedure related pleural effusion
Suspected pulmonary thromboembolism
Pregnant, psychiatric patients
Procedure
A detailed history was taken and physical examination was conducted for all patients.
All patients underwent comprehensive laboratory investigations, comprising complete blood picture, renal and liver function tests, blood glucose, serum LDH, serum protein, electrocardiogram, chest X-ray and sputum CBNAAT. Ultrasound-guided diagnostic thoracentesis was carried out and sent for PF analysis, which includes PF CBNAAT, PF total and differential count, PF AFB, PF gram stain and culture sensitivity, PF ADA, PF cytology, PF cell block, PF protein, sugar and LDH. Patients were evaluated further with CT chest, ICD insertion, bronchoscopy, ultrasound abdomen, closed pleural biopsy, medical thoracoscopy and pleural biopsy wherever needed.
Malignancy in pleural effusion is diagnosed by one of the following:
PF cytology for malignant cells Closed pleural biopsy Bronchoscopic biopsy, transbronchial needle aspiration Thoracoscopic pleural biopsy Known case of MPE presenting with recurrent pleural effusions.
After a definitive diagnosis, CR plus is calculated
(CR plus = CR/PF lymphocyte count) (CR = serum LDH/ PF ADA) and diagnostic yield of the CR and CR plus will be assessed.
Statistical Analysis
Data entered in a Microsoft Excel spreadsheet. SPSS23.0v was used to perform statistical analysis. Categorical variables were summarised into frequencies and percentages, while continuous variables were presented as mean ± standard deviation or median with interquartile range, depending on the normality of data. A receiver operating characteristic (ROC) curve was constructed to calculate the area under the curve (AUC). Predictive values, sensitivity and specificity were determined based on cut-offs that were derived from ROC analysis. A P value of less than .05 is considered statistically significant for testing the hypothesis.
Results
In this study of 110 patients, most of them were aged 45–59 years, with a mean of 49 years. Males were predominant, comprising 62.7% males and 37.3% females. The malignancy cases were on a slightly higher side among the female population, with 53.6%. Out of the 65 cases diagnosed as TB pleural effusion, MTB was diagnosed in PF CBNAAT in only 12 cases (10.9%).
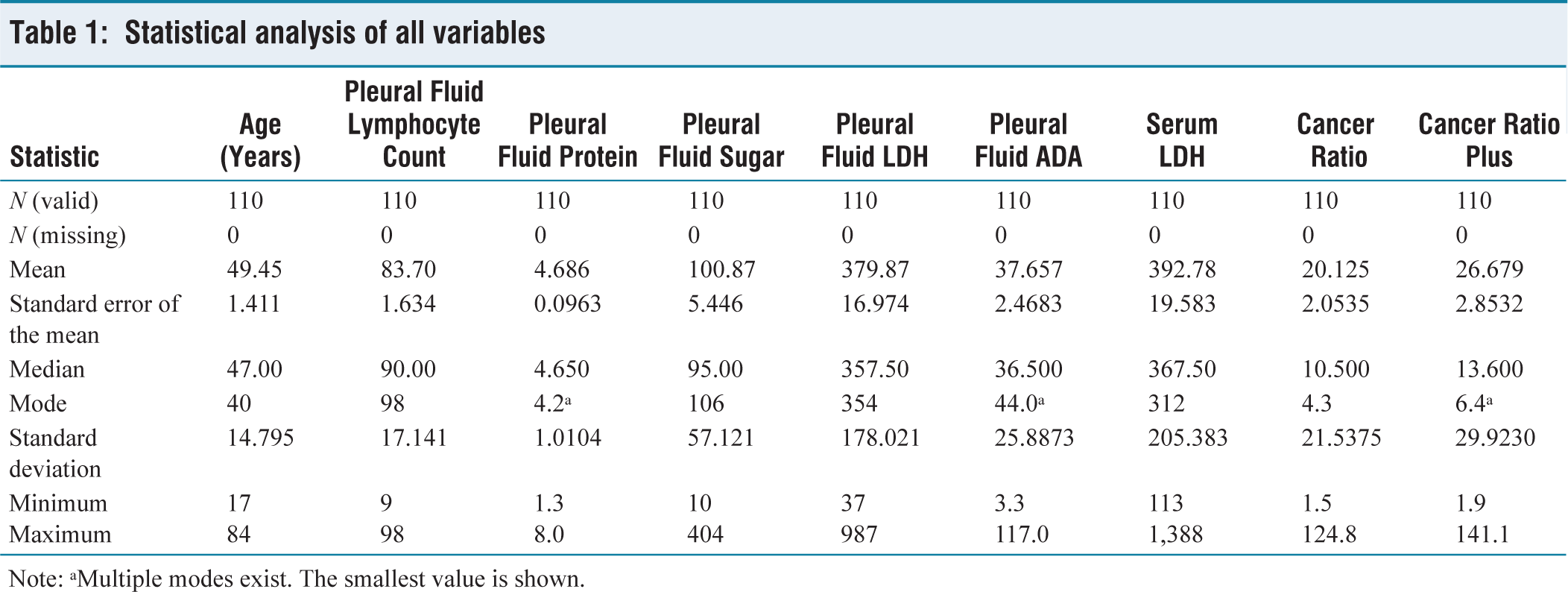
Mean of PF lymphocyte count in MPE is 78.51 ± 18.218 and among non-MPE is 86.78 ± 15.808. Among patients with pleural effusions, the mean of PF protein was 4.61 ± 0.96 g/dL in malignant cases and 4.73 ± 1.04 g/dL in non-malignant cases. The mean of PF LDH in the malignant group and non-malignant group is 407.46 ± 173.903 and 363.48 ± 179.661, respectively. The mean values of serum LDH in MPE are 453.56 ± 262.200 and in non-MPE are 356.67 ± 153.703, with P value of .016 and are found to be statistically significant. The mean PF ADA was 17.40 ± 17.17 U/L in MPE and 49.69 ± 22.50 U/L in tubercular effusion (TPE), with a statistically significant difference (P < .001). PF cytological examination established the diagnosis of malignancy in 14 cases (12.7%) and PF cell block established the diagnosis of malignancy in 18 cases (16.4%). With the invasive investigation of PF biopsy, the diagnosis of malignancy was established in 16 cases (14.5%) Statistical analysis of all variables is tabulated in Table 1.
Statistical analysis of all variables
Out of the 110 cases, 41 (37.3%) cases had MPEs: 65 cases (59.1%) had TPEs, one case had a pancreatic pleural fistula and the other 3(3.6%) cases had parapneumonic effusions. Final diagnosis is established after thorough evaluation and the aetiology of malignancy was confirmed by PF cytology alone (n = 11), PF cell block alone (n = 14) and pleural biopsy (n = 16). 7 cases were diagnosed as malignant from both PF cytology and cell block. A total of 41 cases (37.3%) were diagnosed as malignant among the 110 cases.
Cancer Ratio
Mean values of CR among MPE and non-MPE are 38.67 ± 24.440 and 9.11 ± 7.851, respectively, with a P value of < .001 which is statistically significant.
Using a cut-off value of 19.45, the test demonstrated a sensitivity of 90.2% and a specificity of 97.1%, with an area under the receiver operating curve (AUC) of 0.941.
Cancer Ratio Plus
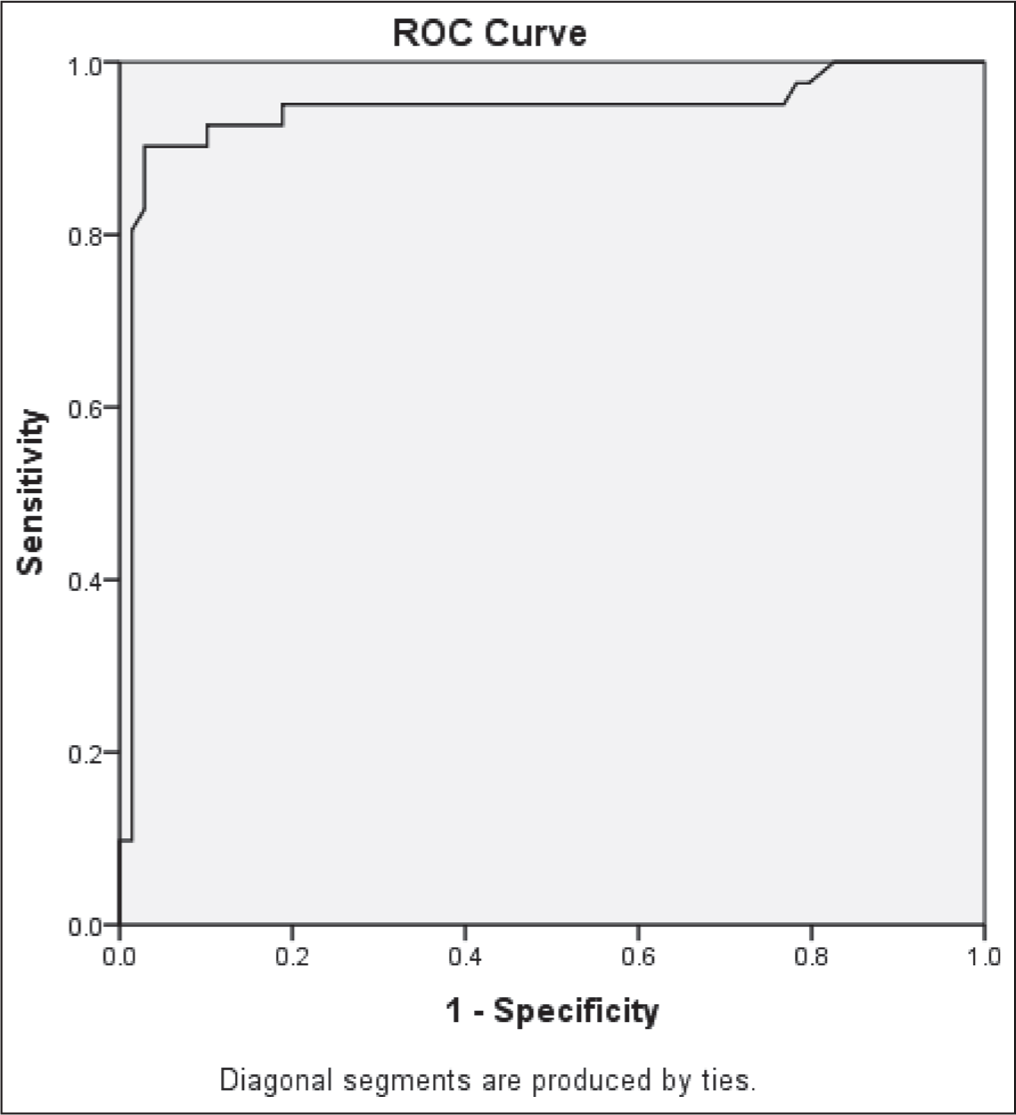
Among the patients, the mean CR plus was 50.63 ± 30.77 in malignant cases and 12.45 ± 18.08 in non-malignant cases. Among 41 malignant cases, two cases had a CR plus value of <20, 17 cases had between 20 and 40 and 22 cases >40. At the cut-off level of 20.05, the sensitivity and specificity are 95.1% and 92.7%, respectively, with an AUC of 0.946 as seen in Figure 1.
ROC curve of CR plus. At a cut-off of 20.5, the sensitivity and specificity of CR plus are 95.1% and 92.7%, respectively, with an AUC of 0.946
Discussion
The present study was conducted among 110 patients with exudative pleural effusions in a tertiary care centre in coastal Andhra.
Among the various etiologies of pleural effusions, exudative effusions are common. Infectious causes are most common, followed by malignant effusions. But, to diagnose malignant effusions is a tedious process and needs varied resources.
Hence, newer diagnostic tests using simpler parameters have been tried, which include CR and CR plus.
CR was calculated by dividing serum LDH by PF ADA. The mean value of CR among the MPEs is 38.67 ± 24.440 and among non-MPEs is 9.1 ± 7.851.
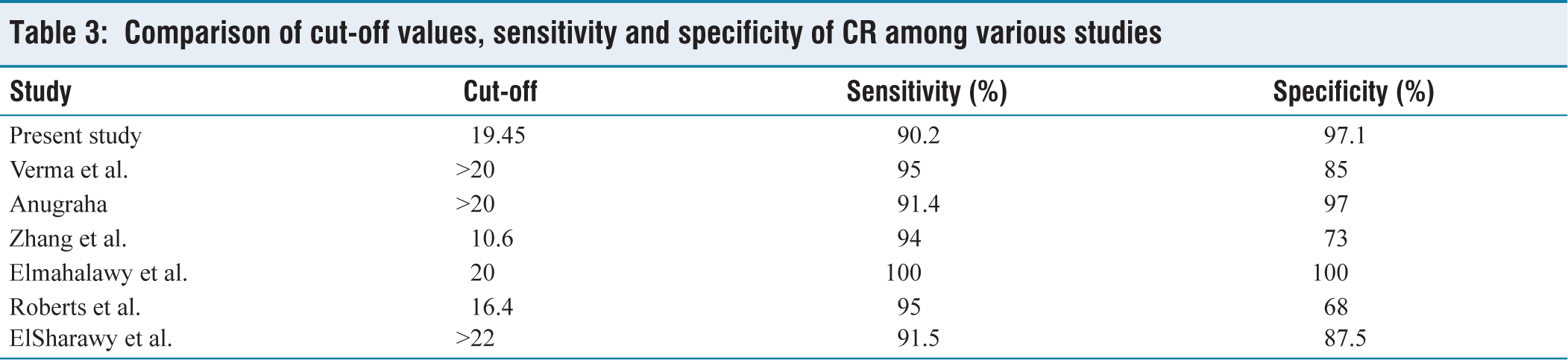
At a cut-off of 19.45, sensitivity and specificity are 90.2% and 97.1%, respectively, with an AUC of 0.941. In Verma et al.[7] the mean values of CR among MPE and non-malignant are 65 and 11.5, respectively; and at a cut-off level of >20, the sensitivity and specificity of ‘CR’ were 0.95 (95% CI 0.87–0.98) and 0.85 (95% CI 0.68–0.94), respectively. AUC was 0.81. In the study done by Anugraha[9] the mean value of CR is 45.2 for MPE and 8.1 for non-malignant. At the cut-off of >20, the sensitivity is 91.4 and the specificity is 97%. In a study by Zhang et al.[10] at a cut-off of 10.6, the AUC is 0.84 and the sensitivity is 94% and the specificity is 73%. In Elmahalawy et al.[11] study, at a cut-off of 20, the sensitivity and specificity are both 100%. In Roberts et al.[4] study, with a cut-off of 16.4, sensitivity and specificity were 95% and 68%, respectively and the AUC was 0.83. A study by ElSharawy et al.[12] reported that a CR with a cut-off value ≥ 22 can effectively differentiate MPE from other causes, showing sensitivity of 91.5% and specificity of 87.5%.
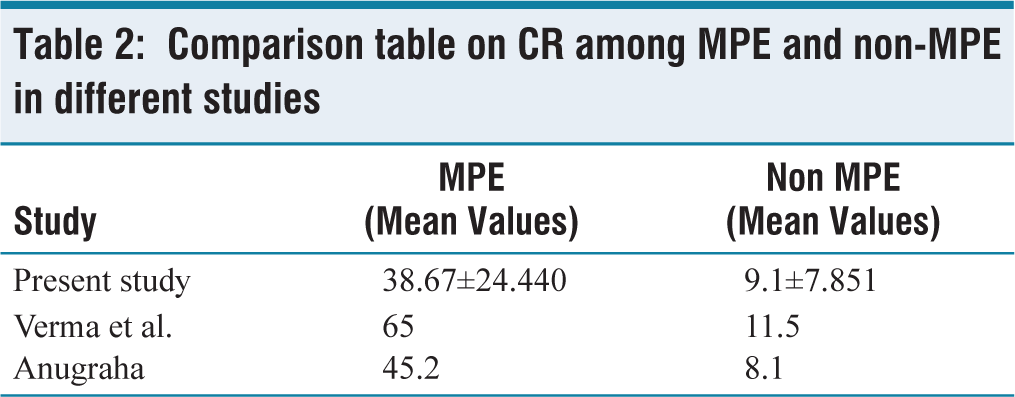
Table 2 illustrates the comparison of CR among MPE and non-MPE in different studies and Table 3 summarises the cut-off values along with the sensitivity and specificity of CR reported in multiple studies.
Comparison table on CR among MPE and non-MPE in different studies
Comparison of cut-off values, sensitivity and specificity of CR among various studies
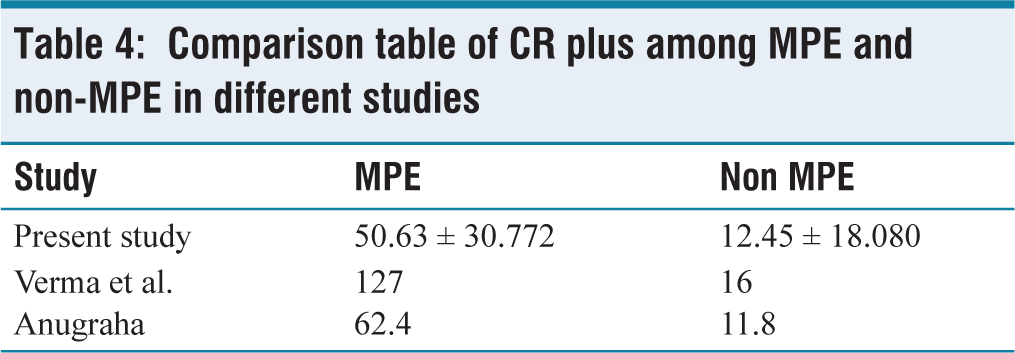
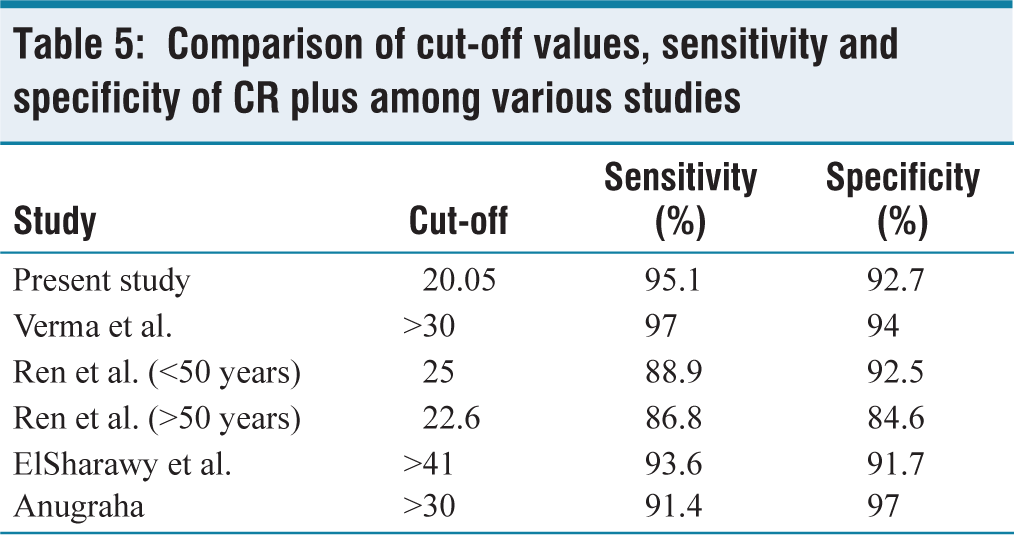
CR plus is obtained by dividing the CR by the PF lymphocyte count. In the present study, the mean CR plus among malignant effusions was 50.63 ± 30.772, whereas in non-MPEs it was 12.45 ± 18.080, which is comparable to findings reported in the study of Anugraha.[9] At the cut-off level of 20.05, the sensitivity and specificity are 95.1% and 92.7%, respectively, with an AUC of 0.946. In Verma et al.[8] study, means of CR plus among MPE and non-malignant are 127 and 16, respectively. At a cut-off level of >30, the sensitivity and specificity of CR plus were 0.97 (95% CI 0.90–0.99) and 0.94 (95% CI 0.78–0.98), respectively. AUC was 0.86.
In Ren et al.[13] study, among age <50 years, at a cut-off of 25, the AUC, sensitivity and specificity are 0.93, 88.9% and 92.5%, respectively.
Among age >50 years, at a cut-off of 22.6, AUC, the sensitivity and the specificity are 0.836, 86.8%, 84.6%, respectively. In a study by ElSharawy et al.[12] CR plus at a cut-off value of ≥ 41 can discriminate MPE from any other cause with a sensitivity 93.6%, and specificity 91.7%. In a study by Anugraha[9], the mean of CR plus in MPE is 62.4 and tuberculosis is 11.8. It is observed that, at the cut-off of more than 30, the sensitivity is 91.4 and the specificity is 97%.
Refer to Table 4 for comparison of CR plus among MPE and non-MPE in different studies and Table 5 for comparison of cut-off values, sensitivity and specificity of CR plus among various studies.
Comparison table of CR plus among MPE and non-MPE in different studies
Comparison of cut-off values, sensitivity and specificity of CR plus among various studies
However, this study has several limitations. The single-centre observational design of the study may restrict the broader applicability of the results. Although all malignant cases were confirmed by histology, the prognosis for these patients remained poor and follow-up was difficult to maintain. In addition, individuals in the non-cancerous group did not consistently attend follow-up appointments, which may have affected longitudinal assessment. Delays in sample processing could also influence cell counts and the calculated CR. Furthermore, accurate enumeration of lymphocytes in PF remains challenging because these cells can degenerate rapidly, creating diagnostic difficulties. Long-standing haemorrhagic effusions may result in falsely elevated pleural LDH levels, potentially affecting the interpretation of results.
Conclusion
The prime goal of this research on CR and CR plus is to establish the most accurate and quick diagnostic tool for MPEs.
Triage of patients with exudative lymphocytic but inconclusive pleural effusion using biochemical markers such as the CR and CR plus may be beneficial, as these markers are simple, inexpensive and easily accessible and can aid in identifying potential malignant cases.
Footnotes
Acknowledgements
We are extremely thankful to the entire Department of Pulmonary Medicine, Andhra Medical College, Visakhapatnam for their support and guidance throughout the study and for their valuable feedback.
Abbreviations
ADA: Adenosine deaminase; CBNAAT: Cartridge based Nucleic Acid Amplification Test; CEA: Carcinoembryogenic Antigen; CR: Cancer Ratio; CR Plus: Cancer Ratio Plus; CT: Computed tomography; LDH: Lactate Dehydrogenas; MPE: Malignant Pleural Effusion; MTB: Mycobacterium Tuberculosis; PF: Pleural Fluid; TB: Tuberculosis.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
This study was approved by the Institutional Ethics Committee, AMC, Visakhapatnam (28/IEC AMC/JAN 2023).
Informed consent
Written and informed consent has been obtained from all the participants.
Credit author statement
Tarakaturi Sharon Swarna Sheela: Conceptualization, methodology, investigation, analysis.
Raghumanda Sunil Kumar: Supervision, project administration.
Shanti Annapurna Maddala: Data curation, writing, visualization, editing.
Praveena Sreerama: Validation, supervision.
Nithin Kurian: Review and editing.
Data availability statement
Non digital data curated at AMC.
Use of artificial intelligence
Nil.