
Abstract
Background:
Heart failure (HF) remains a major global health burden with high morbidity and mortality. Identification of low-cost and widely available markers of disease severity is essential, particularly in resource-limited settings. Red cell distribution width (RDW), a routine haematological parameter, reflects erythrocyte size variability and has been linked to inflammation, oxidative stress and iron dysregulation in HF. This study evaluated the association of RDW with left ventricular ejection fraction (LVEF) and clinical severity in patients with HF.
Methods:
A cross-sectional study was conducted at a tertiary care hospital, including 90 adult patients with clinically and echocardiographically confirmed HF classified as the New York Heart Association (NYHA) class II-IV. RDW values were obtained from complete blood counts and LVEF was assessed using 2D echocardiography (Simpson’s biplane method). Patients with anaemia, hypothyroidism, chronic liver or renal disease, chronic obstructive pulmonary disease (COPD), alcoholism or autoimmune or inflammatory disorders were excluded. Statistical analysis included Pearson correlation, one-way analysis of variance (ANOVA) and receiver operating characteristic (ROC) curve assessment.
Results:
The mean RDW-coefficient of variation (CV) was 17.04% ± 2.98% and the mean LVEF was 40.6% ± 12.1%. RDW demonstrated a strong negative correlation with LVEF (r = –0.85, P < .001) and increased significantly with higher NYHA class (II: 13.17% ± 0.37%, III: 16.48% ± 2.19%, IV: 20.62% ± 1.69%; P < .001). Patients with reduced ejection fraction (<40%) had significantly higher RDW compared to those with preserved ejection fraction (EF) (18.92% ± 2.47% vs. 14.82% ± 1.71%; P < .001). RDW showed excellent discriminative ability for identifying reduced EF, with an area under the curve (AUC = 0.97).
Conclusion:
RDW, an inexpensive and universally available biomarker, strongly correlates with both echocardiographic (LVEF) and clinical (NYHA class) measures of HF severity. Although not a substitute for established biomarkers, RDW may serve as a practical adjunctive indicator for disease assessment, particularly in primary care and low-resource environments. Future prospective studies are warranted to define standardised cut-offs and validate its prognostic utility.
Keywords
Introduction
Heart failure (HF) is a complex clinical syndrome characterised by structural and/or functional impairment of ventricular filling or ejection of blood, leading to inadequate cardiac output and systemic congestion. Globally, HF affects more than 64 million people and remains a major contributor to morbidity, frequent hospitalisations and premature mortality despite advances in treatment.[1,2] Standard prognostic assessment in HF relies on echocardiographic measurement of left ventricular ejection fraction (LVEF) and biomarkers such as N-terminal pro-brain natriuretic peptide (NT-proBNP).[3,4] However, these tools may be limited by high cost, accessibility issues and lack of availability in resource-constrained settings.
Red cell distribution width (RDW), a routinely reported component of the complete blood count, reflects variability in red blood cell size (anisocytosis). Traditionally used in the evaluation of anaemia, RDW has emerged as a potential prognostic marker in cardiovascular diseases, including coronary artery disease, stroke and HF.[5-7] Elevated RDW is thought to reflect pathophysiological processes relevant to HF, such as systemic inflammation, oxidative stress, iron metabolism dysregulation and neurohormonal activation.[8,9]
Large cohort studies and meta-analyses have consistently shown that elevated RDW is independently associated with adverse HF outcomes, including higher mortality, increased readmission rates and advanced functional class.[10-13] Felker et al. first identified RDW as a novel predictor of all-cause mortality and HF hospitalisation,[14] and subsequent multicenter analyses confirmed that RDW adds prognostic value beyond NT-proBNP and echocardiographic parameters.[11,15] Recent studies from Gu et al. and Kim et al. further demonstrated its predictive utility for readmissions and survival in HF.[12,16] A meta-analysis by Xanthopoulos et al. concluded that each 1% rise in RDW corresponds to nearly a 10% increase in mortality risk.[17]
Despite these findings, data exploring the correlation of RDW with echocardiographic indices such as LVEF and with clinical severity scales such as the New York Heart Association (NYHA) class remain limited in Indian populations. Considering RDW is universally available, inexpensive and pathophysiologically relevant, it may serve as a practical biomarker for HF risk stratification in routine practice. This study, therefore, aimed to evaluate the prognostic significance of RDW in HF by analysing its association with LVEF and NYHA functional class in an Indian cohort.
Aims and Objectives
Aim: To evaluate the association between RDW, LVEF and clinical severity (NYHA classification) in patients with HF.
Objectives:
To assess the correlation between RDW and LVEF in patients with HF, as measured by 2D echocardiography. To determine the association between RDW and the clinical severity of HF, categorised according to the NYHA functional classes. To analyse the relationship of RDW with key clinical features and risk factors associated with HF (e.g., hypertension, diabetes, ischaemic heart disease, previous myocardial infarction).
Material and Methods
Study Design and Setting
This cross-sectional observational study was conducted in the Department of Internal Medicine at a tertiary care centre in North India between August 2022 and January 2024.
Study Population
A total of 90 patients with clinically diagnosed HF were enrolled after obtaining informed consent. Patients included both newly diagnosed cases and those with a prior diagnosis of HF who presented with symptoms and signs consistent with the syndrome and underwent routine echocardiography. No upper age limit was applied, as the study aimed to capture the full adult spectrum of HF severity. Older adults represent a major portion of the HF population and excluding them could have limited external validity. The influence of age on RDW was not used as an exclusion factor but was considered during correlation analysis.
Sample Size Calculation
For the confidence level of study at 95% (α = 0.05) and power of 80% (β = 0.2), a minimum of 85 patients (Previous studies reported, correlation coefficient between RDW and LVEF is 0.3) are required to study the correlation between RDW and LVEF in patients.
Sample Size Justification:
Study used: RDW and its relationship with global longitudinal strain in patients with HF with reduced ejection fraction: A study using two-dimensional speckle tracking echocardiography.
Formula for calculating the sample size

where,
N is the sample size, Z is the z score
The standard normal deviate for α = Zα = 1.9600 The standard normal deviate for β = Zβ = 0.8416
C = 0.5 * ln[(1 + r)/(1 – r)] = 0.3095, where r is the observed correlation coefficient. N = [(1.9600 + 0.8416)/0.3095]2 + 3 = 85
The minimum required sample size was 85. To account for exclusions, 90 patients were ultimately included.
Inclusion Criteria
Adult patients aged ≥18 years.
Clinical and/or echocardiographic confirmation of HF.
Symptomatic patients belonging to NYHA functional class II-IV (class I patients were excluded, as they are typically asymptomatic and often evaluated for non-HF indications).
Patients with either preserved or reduced LVEF, as determined by 2D echocardiography.
Exclusion Criteria
Anaemia (haemoglobin <12 g/dL) or history of blood transfusion within the past three months.
Known haematological malignancies.
Chronic liver or renal disease.
Hypothyroidism.
Chronic obstructive pulmonary disease (COPD) or cor pulmonale unrelated to left-sided HF.
Chronic alcohol use disorder.
Chronic inflammatory or autoimmune diseases (e.g., rheumatoid arthritis, systemic lupus erythematosus).
Patients who declined to provide informed consent.
Clinical Assessment
All patients underwent a detailed history and physical examination, including symptom assessment (dyspnoea, orthopnoea, paroxysmal nocturnal dyspnoea (PND), chest pain, palpitations, fatigue) and clinical signs (jugular venous pressure, pedal oedema, rales, S3 gallop). Functional status was classified using the NYHA classification (class II-IV).
Investigations
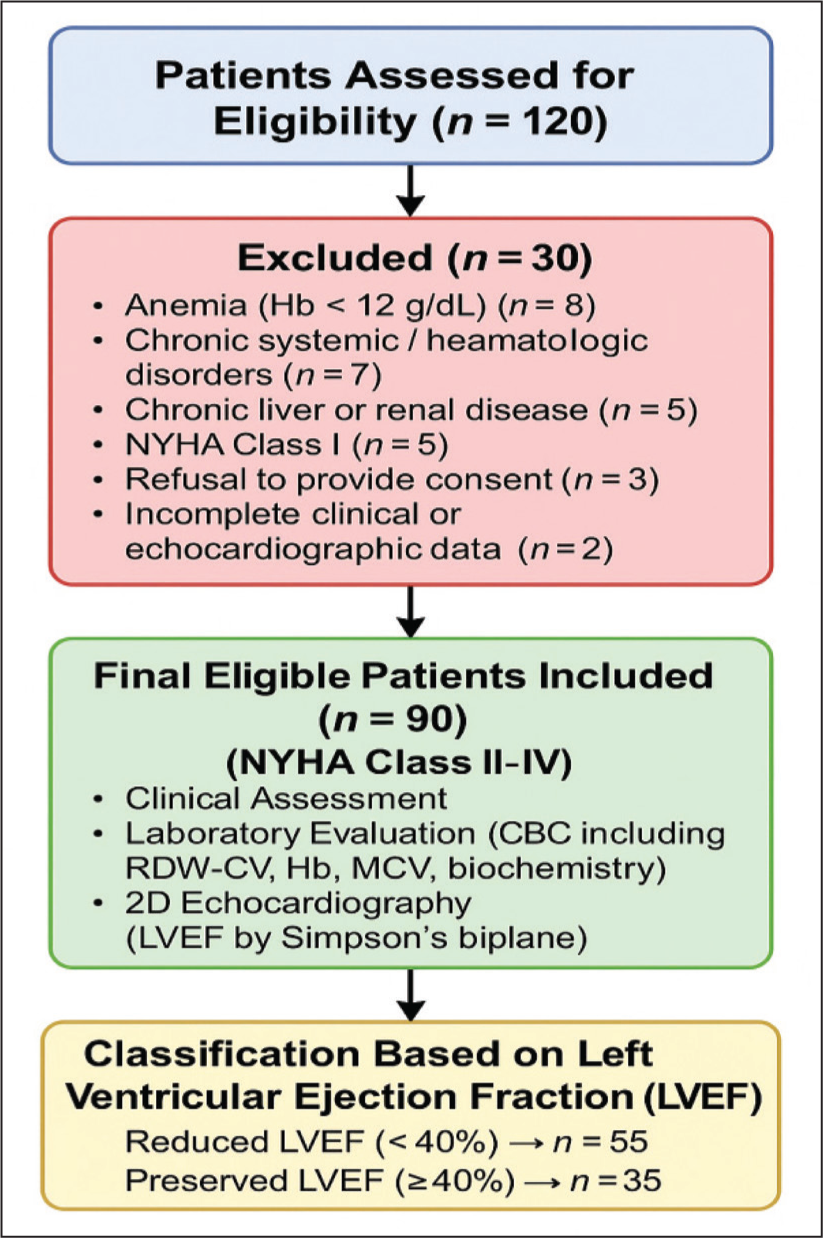
Laboratory tests: Complete blood count including RDW-coefficient of variation (CV) (%) and mean corpuscular volume (MCV), blood glucose, lipid profile, liver and renal function tests and electrolytes. The patient recruitment and enrolment process is shown in Figure 1.
Echocardiography: LVEF was assessed by the Simpson’s biplane method using 2D transthoracic echocardiography.
Other tests: Electrocardiogram and chest X-ray were performed for structural and rhythm evaluation.
Statistical Analysis
Data were analysed using SPSS version 16.0 (Chicago, IL, USA). Continuous variables were expressed as mean ± standard deviation (SD) and categorical variables as percentages.
Pearson correlation coefficient was used to evaluate the association between RDW and LVEF.
One-way analysis of variance (ANOVA) and independent t-tests were applied to compare RDW across NYHA classes and categorical variables such as diabetes, hypertension and prior myocardial infarction.
Receiver operating characteristic (ROC) analysis was performed to assess the discriminative ability of RDW for reduced LVEF (<40%).A P value < .05 was considered statistically significant.
Results
Baseline Characteristics
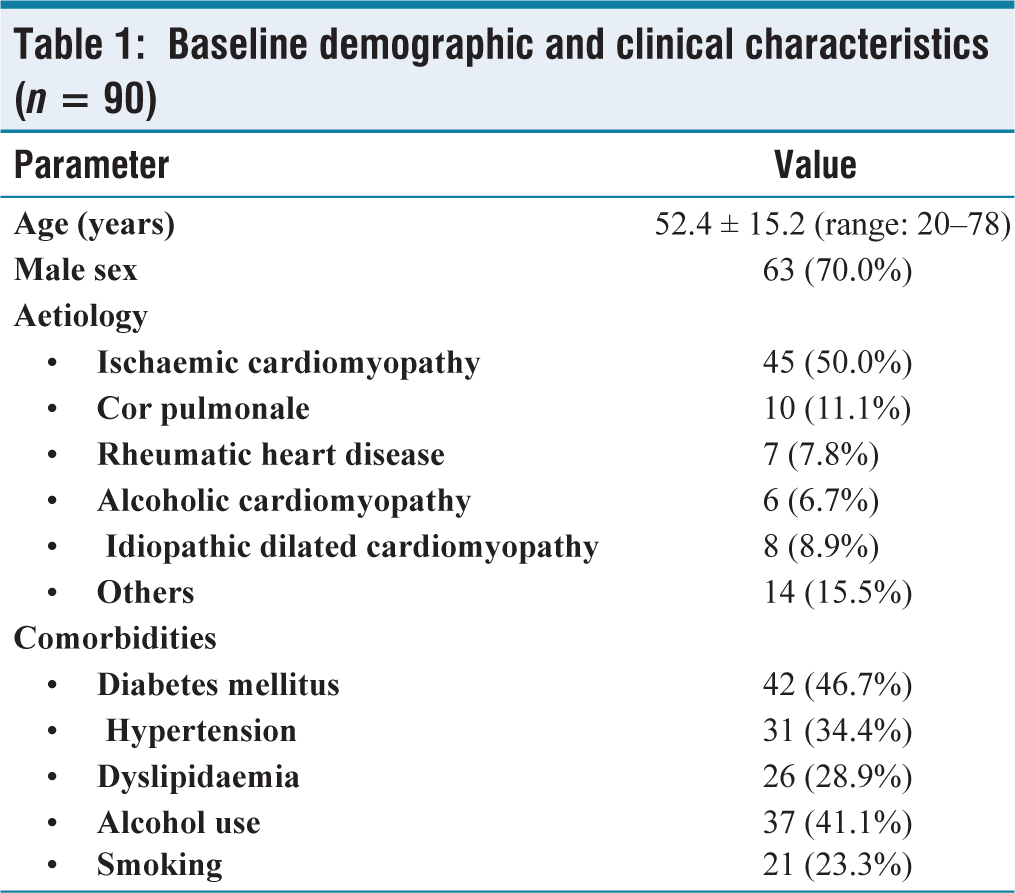
A total of 90 patients with HF were included in the final analysis. The mean age was 52.4 ± 15.2 years (range 20-78 years) and the majority were male (70%, n = 63). The most frequent aetiology was ischaemic cardiomyopathy (50%), followed by cor pulmonale (11.1%) and rheumatic heart disease (7.8%). Diabetes mellitus (46.7%) and hypertension (34.4%) were the most common comorbidities. Detailed baseline demographic and clinical characteristics are presented in [Table 1].
Baseline demographic and clinical characteristics (n = 90)
Laboratory and Echocardiographic Parameters
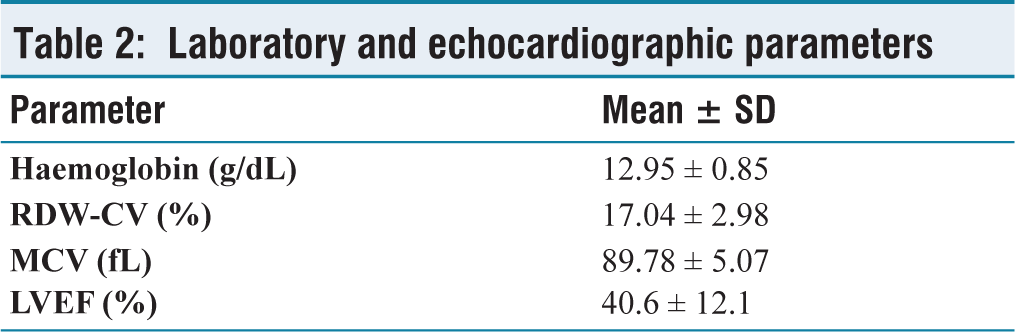
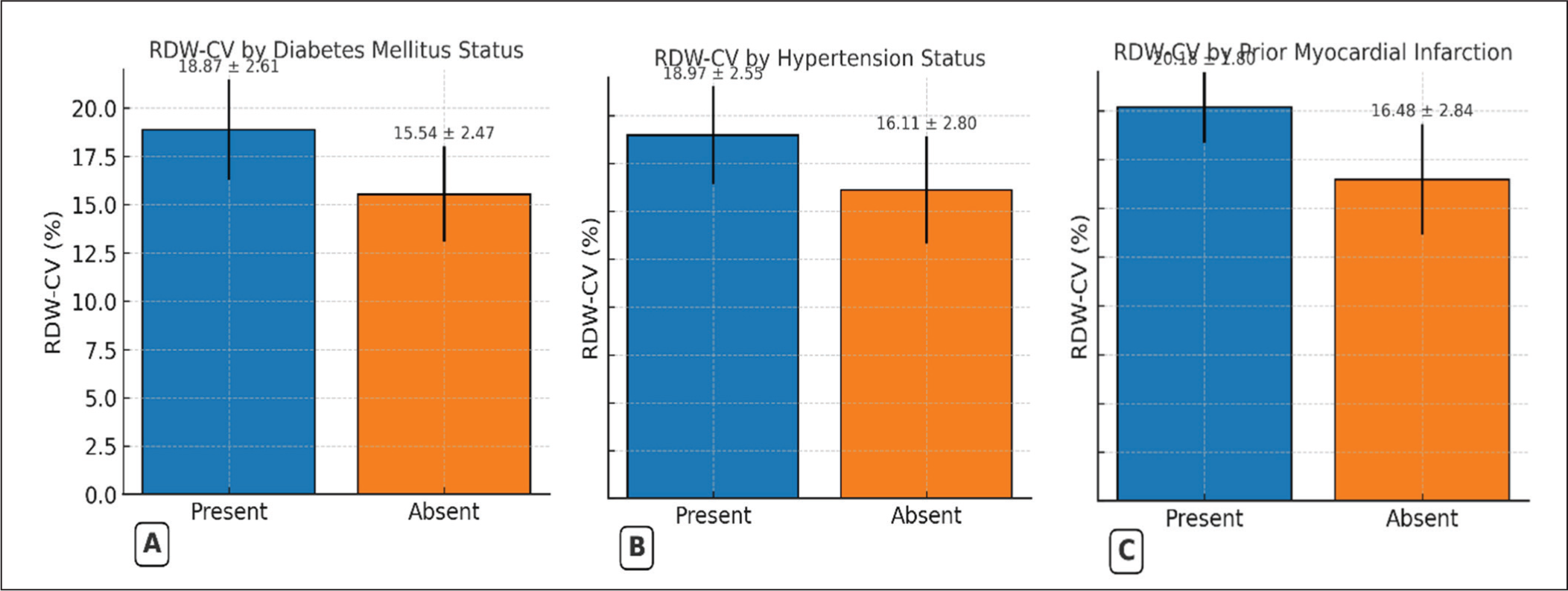
The mean RDW-CV was 17.04% ± 2.98%, the mean haemoglobin was 12.95% ± 0.85 g/dL and the mean MCV was 89.78 ± 5.07 fL. The mean LVEF was 40.6% ± 12.1% [Table 2]. RDW-CV was higher in patients with diabetes versus those without (18.87% ± 2.61% vs. 15.54% ± 2.47%; P < .001; [Figure 2A]). A similar pattern was seen for hypertension (18.97% ± 2.55% vs. 16.11% ± 2.80%; P < .001; [Figure 2B]) and prior MI (20.18% ± 1.80% vs. 16.48% ± 2.84%; P < .001; [Figure 2C]).
Laboratory and echocardiographic parameters
The mean haemoglobin level was 12.95 ± 0.85 g/dL and showed no significant correlation with RDW-CV (r = –0.04, P = .66). This suggests that RDW variation in our cohort was largely independent of anaemia severity.
RDW and NYHA Functional Class
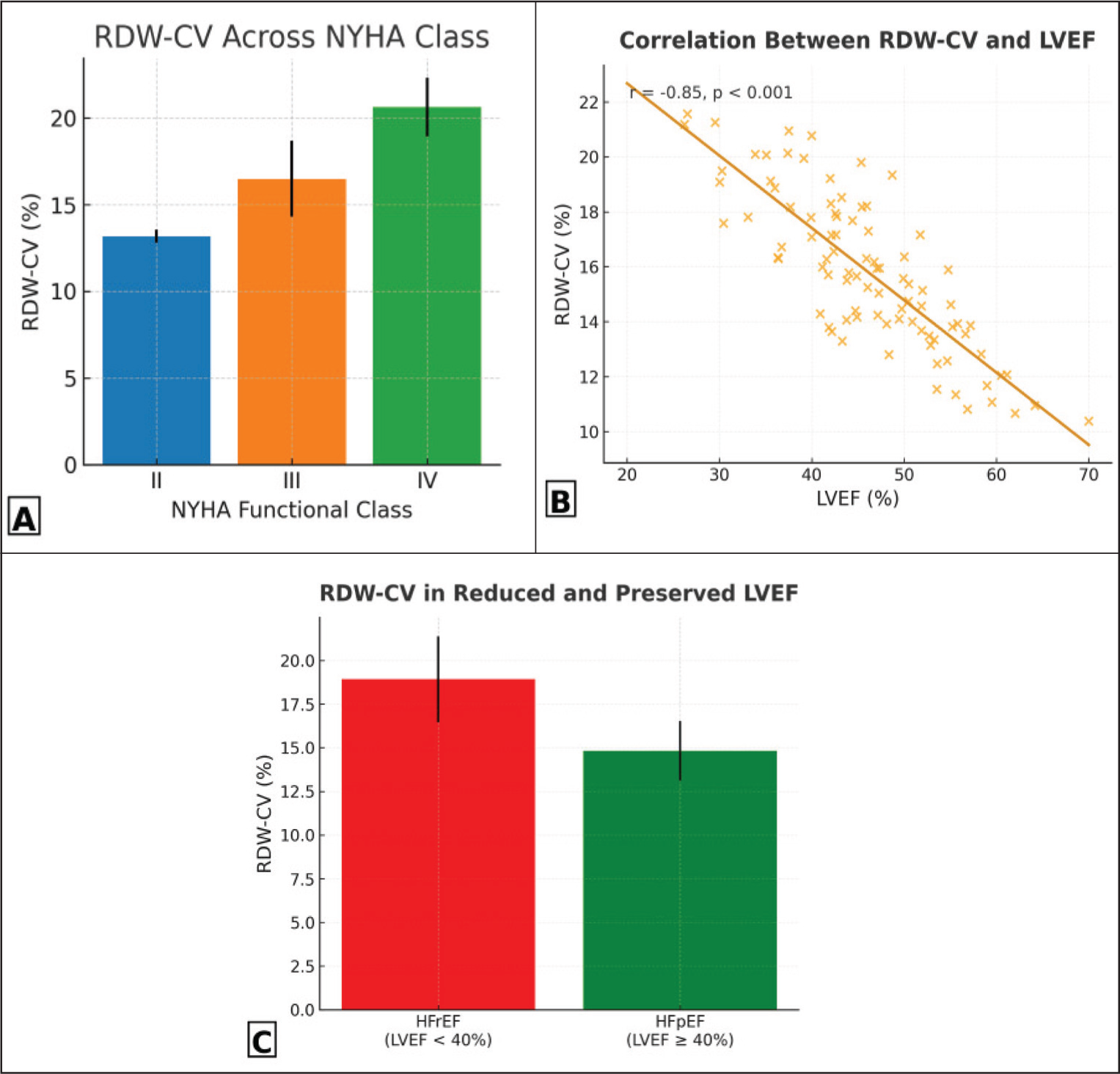
RDW increased significantly with higher NYHA class (P < .001, ANOVA) [Table 3, Figure 3A].
RDW-CV across NYHA functional classes
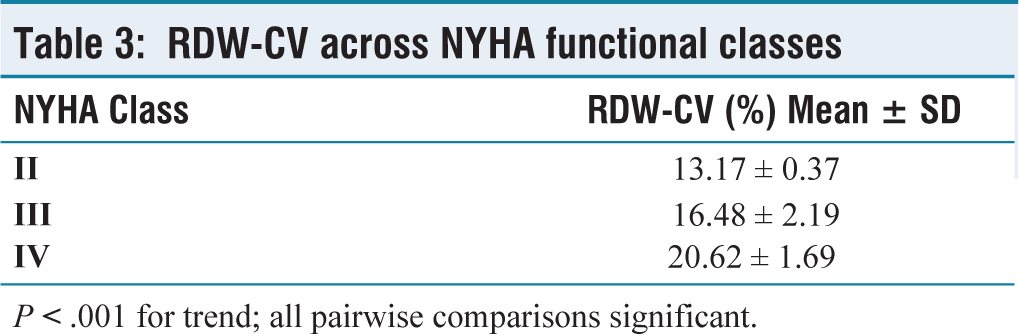
P < .001 for trend; all pairwise comparisons significant.
(A) Mean RDW-CV across NYHA functional classes in patients with HF (n = 90). RDW-CV increased progressively from class II to class IV (ANOVA P < .001; all pairwise comparisons significant). (B) Scatter plot showing strong negative correlation between RDW-CV and LVEF measured by Simpson’s biplane method (r = –0.85, P < .001). The shaded area represents the 95% confidence interval for the regression line. (C) Bar graph comparing mean RDW-CV in patients with reduced ejection fraction (HFrEF, LVEF < 40%) and preserved ejection fraction (HFpEF, LVEF ≥ 40%). RDW-CV was significantly higher in HFrEF (18.92% ± 2.47%) than in HFpEF (14.82% ± 1.71%; P < .001). Error bars represent SD
NYHA II: 13.17% ± 0.37%
NYHA III: 16.48% ± 2.19%
NYHA IV: 20.62% ± 1.69%
Correlation Between RDW and LVEF
Pearson correlation analysis demonstrated a strong negative correlation between RDW and LVEF (r = –0.85, P <.001). This relationship is depicted in [Figure 3B], where RDW values increased as LVEF declined. MCV showed a modest positive correlation with RDW (r = 0.43, P = .001), while haemoglobin did not correlate significantly (r = –0.04, P = .66). Patients with reduced ejection fraction (heart failure with reduced ejection fraction [HFrEF], LVEF < 40%) exhibited significantly higher mean RDW-CV values compared with those with preserved ejection fraction (HFpEF, LVEF ≥ 40%). The mean RDW-CV was 18.92% ± 2.47% in the reduced ejection fraction (EF) group versus 14.82% ± 1.71% in the preserved EF group (P < .001). This relationship remained significant after adjusting for age and haemoglobin levels. This difference between reduced and preserved ejection fraction groups is graphically illustrated in [Figure 3C]. The higher RDW among patients with HFrEF indicates greater erythrocyte size variability, suggesting a closer link with advanced disease stage and chronic inflammatory activity.
Association with Clinical Signs and Symptoms
Patients with hallmark signs and symptoms of HF, orthopnoea, PND, elevated jugular venous pressure (JVP), pedal oedema, rales and S3 gallop, had significantly higher RDW values compared with patients without these findings (all P < .001). These associations are illustrated in [Figure 4].
Mean RDW-CV by presence or absence of common HF symptoms and signs. Patients with each feature had significantly higher RDW-CV values than those without
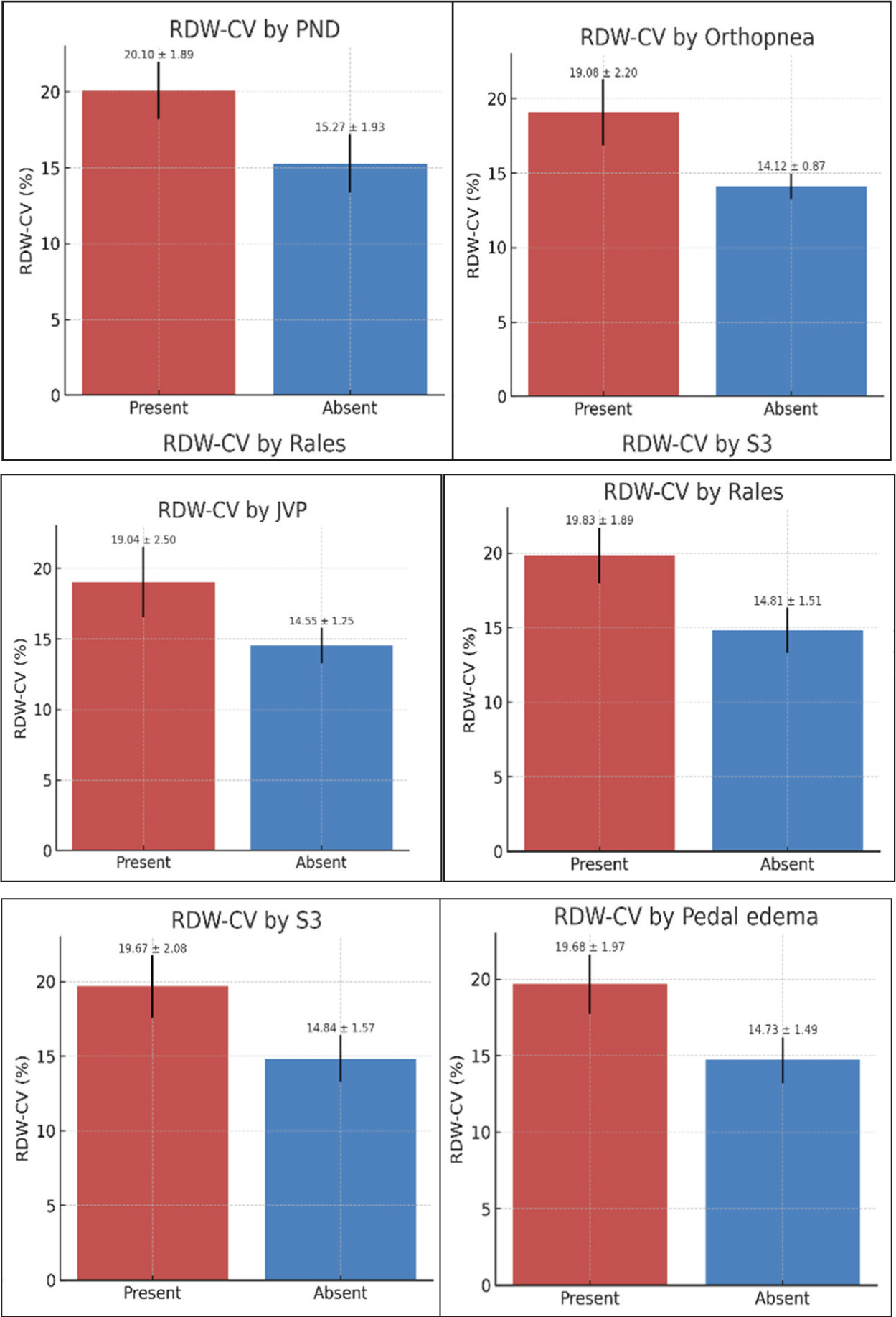
PND: 20.10% ± 1.89% vs. 15.27% ± 1.93%
Orthopnoea: 19.08% ± 2.20% vs. 14.12% ± 0.87%
Elevated JVP: 19.04% ± 2.50% vs. 14.55% ± 1.25%
Rales: 19.83% ± 1.89% vs. 14.81% ± 1.51%
S3 gallop: 19.67% ± 2.08% vs. 14.84% ± 1.57%
Pedal oedema: 19.68% ± 1.97% vs. 14.73% ± 1.49%
All comparisons were significant at P < .001 (unpaired t-test).
Diagnostic Performance of RDW
ROC analysis demonstrated excellent discriminative ability of RDW for predicting reduced LVEF (<40%). The area under the curve (AUC) was 0.97, indicating high diagnostic accuracy [Figure 5].
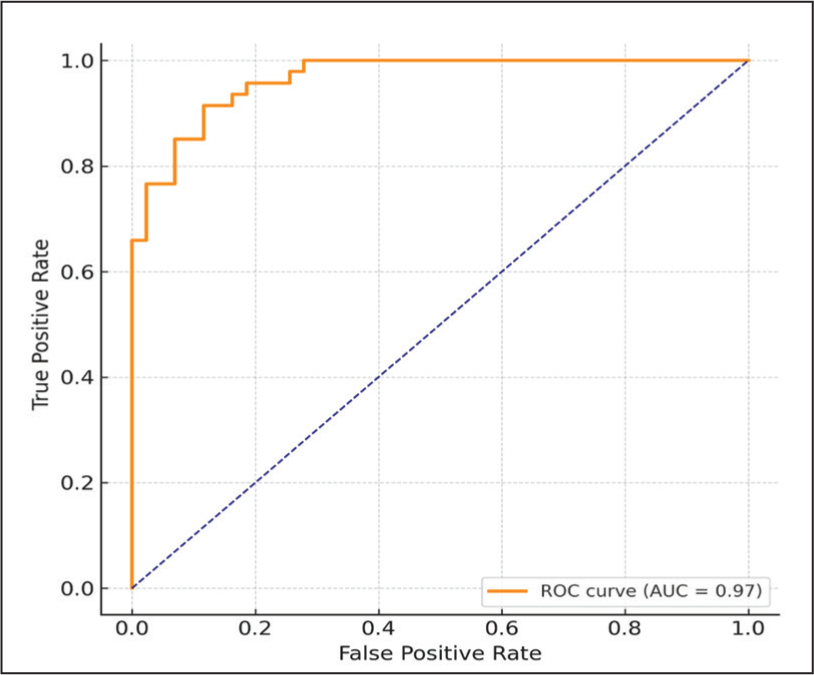
The diagonal dashed line represents the line of no discrimination (AUC = 0.5)
Discussion
The present cross-sectional study evaluated the relationship between RDW and both the clinical and echocardiographic severity of HF. A significant inverse correlation was found between RDW and LVEF (r = –0.85, P < .001) and RDW increased progressively across higher NYHA functional classes (P < .001). These findings highlight that RDW, a simple and routinely available haematological parameter, reflects disease severity in patients with HF.
The association between elevated RDW and worsening HF can be explained by several interrelated pathophysiological mechanisms. RDW reflects anisocytosis or variability in red cell size, which may result from inflammation, oxidative stress, impaired erythropoiesis and nutritional or iron-handling disturbances.[18,19] In HF, chronic systemic inflammation mediated by cytokines such as interleukin-6 (IL-6) and tumour necrosis factor-α impairs erythropoietin production and increases hepcidin levels, leading to restricted iron utilisation and functional iron deficiency even in the absence of anaemia.[20] In this study, the mean haemoglobin level did not correlate significantly with RDW (r = –0.04, P = .66), indicating that anisocytosis represents intrinsic disease-related alterations rather than merely the presence of anaemia. The observed RDW changes likely reflect a combination of inflammatory and metabolic dysregulation common in chronic HF.
Our results are consistent with previous studies demonstrating the association between RDW and HF severity. Lippi et al.[5] and Tonelli et al.[7] reported that higher RDW predicted adverse cardiovascular outcomes and hospitalisation in HF patients. Allen et al.[21] also found a strong association between RDW, neuro-hormonal markers such as NT-proBNP and poorer functional capacity. The present findings corroborate these reports in an Indian cohort, underscoring the reproducibility of RDW as a marker of disease burden across populations and care settings.
In subgroup analysis (Figure 3C), patients with reduced ejection fraction (HFrEF, LVEF < 40%) demonstrated significantly higher RDW-CV compared with those with preserved ejection fraction (HFpEF, LVEF ≥ 40%) (18.92% ± 2.47% vs. 14.82% ± 1.71%; P < .001), reinforcing its strong inverse relationship with myocardial function. This finding supports the hypothesis that RDW elevation parallels myocardial dysfunction severity. Similar trends have been observed in prior studies,[5,6,21] suggesting that RDW may capture systemic processes such as oxidative stress, chronic inflammation and impaired erythropoiesis that are more pronounced in advanced systolic dysfunction.
The clinical relevance of RDW lies in its simplicity, affordability and universal availability through routine complete blood counts. Although nonspecific, RDW could serve as an adjunctive marker for assessing HF severity, particularly in low-resource settings where advanced biomarkers or imaging modalities may not be readily available.[3] Its integration with established biomarkers such as NT-proBNP, troponin and echocardiographic indices could improve the accuracy of risk assessment and disease monitoring.
This study has certain limitations. Its cross-sectional design restricts causal inference regarding the prognostic impact of RDW. Although efforts were made to exclude patients with potential confounding conditions such as anaemia, hypothyroidism, chronic liver or renal disease, COPD, alcoholism and chronic inflammatory or autoimmune disorders, residual confounding due to subclinical or overlapping comorbidities cannot be entirely excluded. Iron studies (serum ferritin, transferrin saturation and reticulocyte count) were not performed, limiting the ability to evaluate functional iron deficiency as a contributor to RDW elevation. Furthermore, RDW tends to increase with age and while this was accounted for during analysis, residual age-related effects may persist.[22] As a single-centre study with a relatively small sample size, the generalisability of the results is limited and requires validation in larger, multicentric cohorts.
Despite consistent associations observed across studies, there is currently no universally accepted cut-off value for RDW in HF. Laboratory-to-laboratory variability and population heterogeneity further complicate its standardisation. Large-scale prospective multicentric studies are needed to establish population-specific reference ranges and clinically meaningful thresholds for RDW. Future work should also explore the role of serial RDW measurements as a potential tool for monitoring therapeutic response and predicting outcomes. Incorporating RDW into multimarker models alongside natriuretic peptides and echocardiographic indices may enhance comprehensive HF risk stratification.
In summary, this study reinforces the strong association between elevated RDW and increased severity of HF based on both clinical (NYHA class) and echocardiographic (LVEF) parameters. RDW represents a low-cost, easily measurable parameter that reflects the systemic inflammatory and metabolic milieu of HF. Although it should not replace established biomarkers, RDW may serve as a complementary index of disease burden. Further multicentric prospective studies are warranted to validate standardised RDW cut-offs and evaluate their long-term prognostic value in HF management.
Conclusion
In patients with HF, RDW is strongly and inversely associated with LVEF and rises progressively with increasing NYHA functional class, symptom burden and the presence of major cardiovascular risk factors. RDW demonstrated excellent discrimination for identifying reduced LVEF, highlighting its potential as a low-cost, readily available biomarker for risk stratification. Given its universal availability through routine complete blood counts, RDW may serve as a practical adjunct to established diagnostic and prognostic tools, particularly in resource-limited settings. Prospective studies are warranted to validate these findings, determine optimal cut-off values and evaluate the prognostic impact of temporal changes in RDW.
Clinical Implications
Low-cost, universally available biomarker: RDW is included in every complete blood count, requiring no additional cost or specialised equipment, making it particularly valuable in primary care and resource-limited settings.
Early risk identification: Elevated RDW can flag patients at higher risk of reduced LVEF or advanced NYHA functional class, prompting timely referral for echocardiography and specialist assessment.
Augmentation of current risk models: Integrating RDW with established prognostic markers such as NT-proBNP, troponin and echocardiographic parameters may improve the accuracy of HF risk stratification.
Symptom correlation: RDW elevation parallels symptom severity (orthopnoea, PND, JVP elevation, rales, pedal oedema), allowing clinicians to use it as an objective adjunct to subjective clinical evaluation.
Potential for serial monitoring: Periodic RDW measurement may help track disease progression or response to therapy, as changes in RDW have been associated with prognosis in HF in prior studies.
Limitations
Cross-sectional design: The study captures associations at a single time point, which prevents causal inference between RDW and the severity of HF.
Sample size: The relatively small cohort (n = 90) limits the statistical power and generalisability of findings to broader HF populations.
Single-centre study: Conducted in one tertiary care hospital, which may introduce selection bias and limit applicability to different healthcare settings.
Lack of longitudinal outcomes: Mortality, readmission rates and other long-term prognostic endpoints were not assessed, precluding evaluation of RDW’s predictive ability over time.
Incomplete haematologic and biochemical profile: Parameters such as RDW-SD, reticulocyte count, iron indices and inflammatory markers were not evaluated, which could have provided additional insight into the underlying mechanisms linking RDW and HF.
Iron studies not universally available: Serum ferritin and transferrin saturation were not performed in all participants, preventing assessment of subclinical iron deficiency as a contributor to elevated RDW.
Potential residual confounding: Although patients with anaemia, hypothyroidism, chronic liver or renal disease, COPD, alcoholism and chronic inflammatory or autoimmune disorders were excluded where possible, unmeasured or subclinical comorbidities may still influence RDW levels.
Age-related variation: RDW tends to increase with advancing age. Since no upper age limit was applied, residual confounding due to age cannot be excluded.
Limited external validity: Findings require confirmation through larger, multicentric, prospective studies incorporating comprehensive haematologic, inflammatory and iron metabolism profiles to validate and expand upon the present results.
Future Directions
Future multicenter prospective studies with larger cohorts are warranted to validate these findings and determine optimal RDW cut-off values for clinical decision-making. Incorporating RDW into multimarker prognostic models alongside NT-proBNP, troponin and echocardiographic indices may further enhance risk stratification. Additionally, serial monitoring of RDW could be explored as a tool for tracking disease progression or therapeutic response in HF.
Footnotes
Acknowledgements
The authors gratefully acknowledge the Department of Internal, Indraprastha Apollo Hospitals, New Delhi, for their continuous guidance, encouragement and logistical support throughout the study. We are also deeply indebted to all the patients and their families for their participation and cooperation, without whom this research would not have been possible.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
The study protocol was approved by the Institutional Ethics Committee of Indraprastha Apollo Hospital (approval number: IAH-BMR-032/05-22).
Informed consent
Written inFormed consent was obtained from all study participants in accordance with the Declaration of Helsinki.
Credit author statement
Dr Ramesh Krishnan: Conceptualisation, methodology, data curation, formal analysis, Writing, original draft, writing, review and editing, visualisation, supervision and project administration. Dr Vijay Kumar Aneja: Patient recruitment, clinical investigation, resources, validation, writing, review and editing, critical revision, final approval of the manuscript.
Both authors have contributed significantly, reviewed and approved the final version of the manuscript.
Data availability
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Use of artificial intelligence
No generative artificial intelligence tools were used in the preparation, writing or editing of this manuscript.