
Abstract
Background and Objectives:
With rising global temperatures, heat-related illness (HRI) poses a growing clinical challenge, often complicated by rhabdomyolysis, acute kidney injury (AKI), and hepatic dysfunction. Chronic medication (CM) use and pre-existing comorbidities may also have an impact on outcomes. With a focus on comorbid conditions, CM use, and laboratory predictors of survival, this study aimed to assess the clinical profile, treatment patterns, and outcomes of patients admitted with HRI.
Method:
A retrospective observational study of 54 patients who were admitted to a tertiary care hospital with HRI was carried out. The following information was gathered and compared between survivors and non-survivors: demographics, comorbidities, CMs, clinical features, laboratory parameters, treatment, and outcomes.
Results:
Overall mortality was 37%. Non-survivors had significantly higher heart rates (P = .008) and lower Glasgow Coma Scale scores (P < .001), indicating greater systemic involvement. Laboratory findings showed markedly elevated creatine phosphokinase in non-survivors, consistent with severe rhabdomyolysis, and higher rates of AKI (37%). Serum creatinine (P = .004) and AST (P = .02) were also significantly elevated, reflecting renal and hepatic dysfunction. In contrast, comorbidities (hypertension, diabetes, cardiovascular disease) and CM use were common but did not significantly influence survival. Supportive management included intravenous fluids, electrolyte correction, vasopressors, and cooling interventions.
Conclusion:
Neurological impairment, tachycardia, elevated CPK, creatinine, and AST levels were key predictors of mortality in HRI, while comorbidities and CM use were not. Early recognition of complications and timely supportive care, including standardised cooling methods, remains essential to improve outcomes.
Introduction
Global temperatures have been steadily rising due to climate change, increasing the frequency, intensity, and duration of extreme heat events. Recent years have seen record-breaking heatwaves in Europe (2022), India (2022), and the Pacific Northwest of the United States (2021). Climate change is now responsible for over one-third of warm-season heat-related deaths, and over the last 20 years, mortality among adults aged 65 years and older has risen by 54%.[1] According to current projections, global temperatures could rise by 2°C by the middle of the century if greenhouse gas emissions do not stop, significantly increasing the health burden of extreme heat.[2,3] For example, a recent prolonged heatwave in India resulted in over 100 deaths and more than 40,000 suspected cases of heatstroke.[4]
From minor heat oedema and cramps to potentially fatal heatstroke, which is characterised by core temperatures above 40°C and central nervous system dysfunction, heat-related illnesses (HRIs) cover a broad range of clinical manifestations.[5] Complications like acute kidney injury (AKI), disseminated intravascular coagulation, hepatic failure, and rhabdomyolysis frequently contribute to mortality.[6] Age extremes, pre-existing cardiovascular or mental health conditions, low physical fitness, and strenuous outdoor activities are some of the factors that raise the risk of HRIs.[7]
Chronic illnesses like Schizophrenia, Diabetes Mellitus (DM), and cardiovascular diseases can make people more prone to overheating, and their medications can make the condition more severe.[8] The risk of HRIs during heatwaves can be increased by medications that interfere with the body’s ability to regulate its temperature, such as antipsychotics, serotonergic agents, anticholinergics, diuretics, beta blockers, stimulants, and antihypertensives. While specific medications are not usually seen as primary triggers, they can amplify heat-induced health issues like heat exhaustion and heatstroke.[9]
This study aimed to assess the association of comorbidities, chronic medication (CM) use, and laboratory parameters with clinical outcomes in HRI and to identify prognostic markers of mortality.
Methodology
This retrospective study was conducted at a tertiary care hospital in Ahmedabad. All patients aged ≥18 years admitted with a diagnosis of HRI during the months of March to July of the year 2024 were included. As this was a retrospective study, all eligible consecutive inpatients identified through hospital records were analysed, and those with incomplete or missing data were excluded.
For each patient, demographic data, comorbidities, history of CM use, presenting temperature and vital signs, Glasgow Coma Scale (GCS), clinical findings, laboratory investigations, management details, and in-hospital outcomes were extracted from case records.
JERATO Score
The Japanese Early Risk Assessment Tool for Heat-Related Illness (JERATO) was used to assess severity at admission. The score has six binary components, each contributing one point if the criterion is met: Respiratory rate ≥22/min, GCS score <15, Systolic blood pressure ≤100 mmHg, Heart rate ≥100 bpm, Body temperature ≥38°C, age ≥ 65 years. Each variable scores one point, for a total range of 0–6, with higher scores indicating greater initial severity.
Ethical Approval
This retrospective study protocol was approved by the Institutional Review Board. In this study, data were collected from the hospital inpatient electronic medical records; the information collected was anonymised.
Statistical Analysis
Data were entered and analysed using Statistical Package for Social Sciences for Windows (SPSS version 26.0). Continuous variables were summarised as mean with standard deviation (SD) for normally distributed data and median with interquartile range (IQR) for skewed data. Categorical variables were expressed as frequencies and percentages. Comparisons between survivors and non-survivors were performed using: independent-samples t-test for normally distributed continuous variables, Mann-Whitney U test for non-normally distributed data, Chi-square test & Fisher’s exact test for categorical variables. Spearman’s rank correlation was used to assess associations between the JERATO score and key clinical variables such as complications, comorbidities, CM use, and survival. A P < .05 was considered statistically significant.
Results
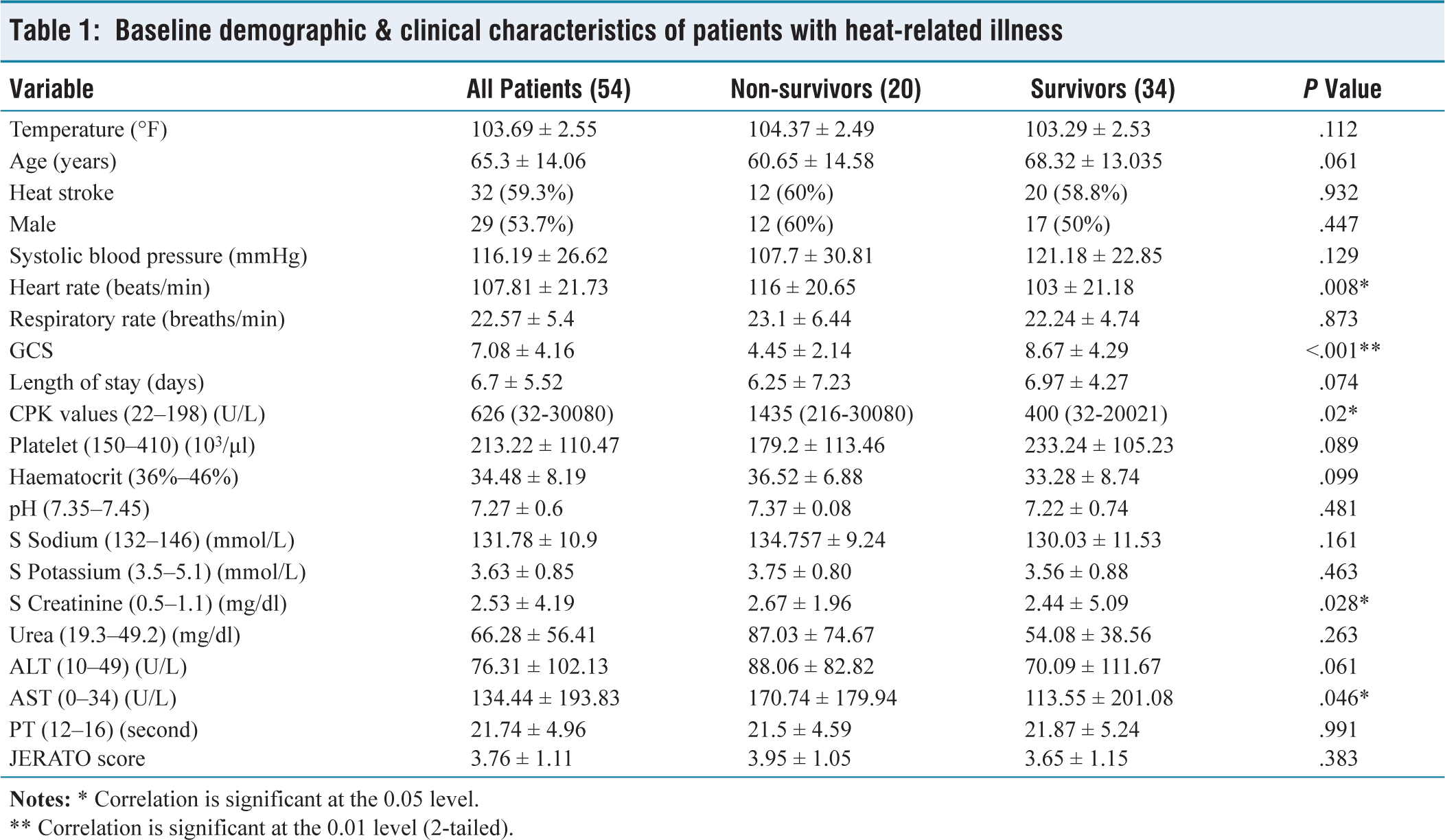
A total of 54 patients with HRIs were included in the study. Their baseline characteristics and laboratory values at the time of arrival are shown in Table 1. In this, 20 (37%) were non-survivors, and 34 (63%) were survivors. The mean age was 65.3 ± 14.06 years. Survivors were slightly older than non-survivors, although the difference was not statistically significant (P = .061).
Baseline demographic & clinical characteristics of patients with heat-related illness
** Correlation is significant at the 0.01 level (2-tailed).
There were no statistically significant differences in gender distribution, presence of heatstroke, body temperature, respiratory rate, systolic blood pressure or length of stay between the two groups.
Heart rate was significantly higher among non-survivors compared to survivors (P = .008). GCS scores were significantly lower among non-survivors than survivors (P < .001), indicating more severe neurological impairment in those who died.
Non-survivors also had statistically significantly higher CPK levels (P = .02), serum creatinine (P = .028), and AST levels (P = .046), indicating greater muscle and hepatic damage. Other parameters, such as platelet count, haematocrit, ALT, serum sodium, and urea, showed trends toward worse values in non-survivors but did not reach statistical significance. JERATO scores were higher in non-survivors but were not statistically different from survivors (P = .383).
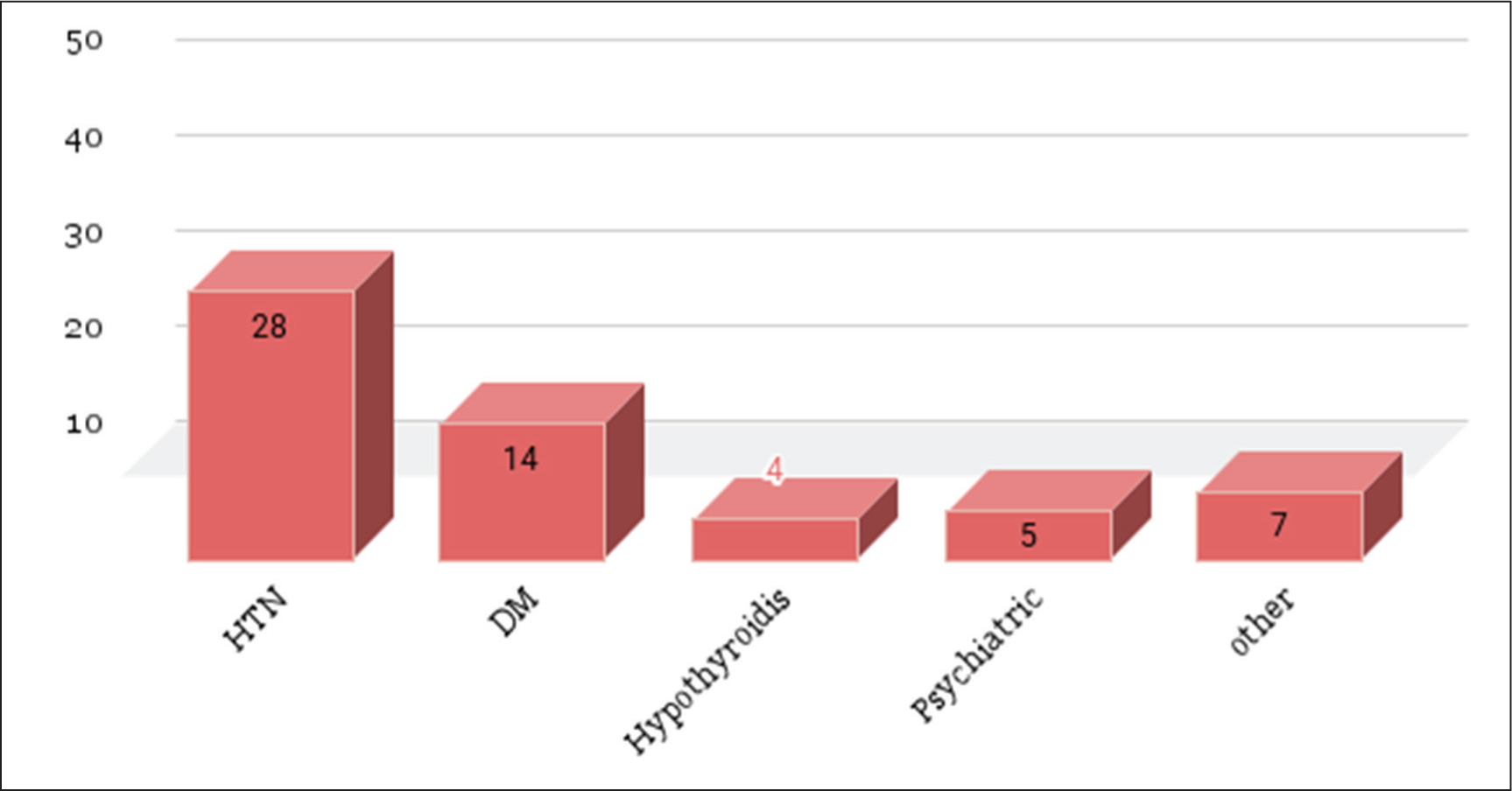
In the study, 34 patients had pre-existing comorbidities [Figure 1]. Hypertension (HTN) was the most frequent, 51.9%, followed by DM (24.1%), psychiatric illnesses and hypothyroidism. Seven patients had other comorbidities, which included Chronic Obstructive Pulmonary Disease, Chronic Kidney Disease, Chronic Liver Disease, Asthma and Rheumatic Arthritis. Eighteen patients had more than one comorbidity.
Comorbidities
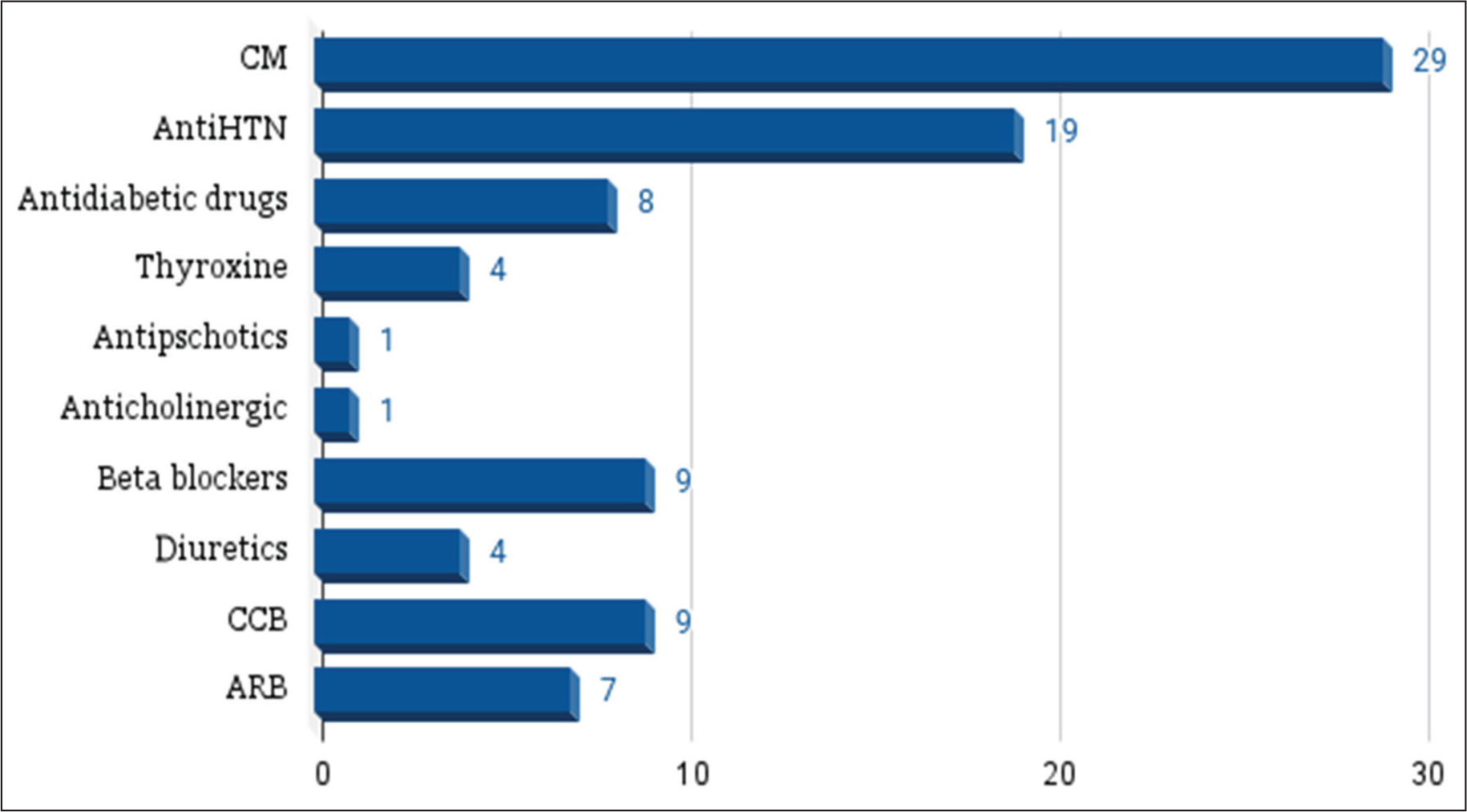
Out of the total patients, 29 (53.7%) were on one or more CM [Figure 2]. Among these, antihypertensive (AntiHTN) were the most commonly used drug class (n = 19), including beta blockers in nine patients, Calcium channel blockers (CCBs) in nine patients, Angiotensin receptor blockers (ARBs) in seven patients and diuretics in four patients. Antidiabetic drugs were taken by eight patients, and Thyroxine by four patients. Antipsychotic and anticholinergic medications were reported in one patient each. Some patients were on multiple medications, especially within the antihypertensive group.
Chronic medications
Among the 54 patients included in the study, 34 patients (63%) had at least one pre-existing comorbidity. There was no statistically significant difference in the overall presence of comorbidities between non-survivors (65%) and survivors (61.8%) (P = .812) [Table 2].
Comparison of comorbidities between survivors & non-survivors

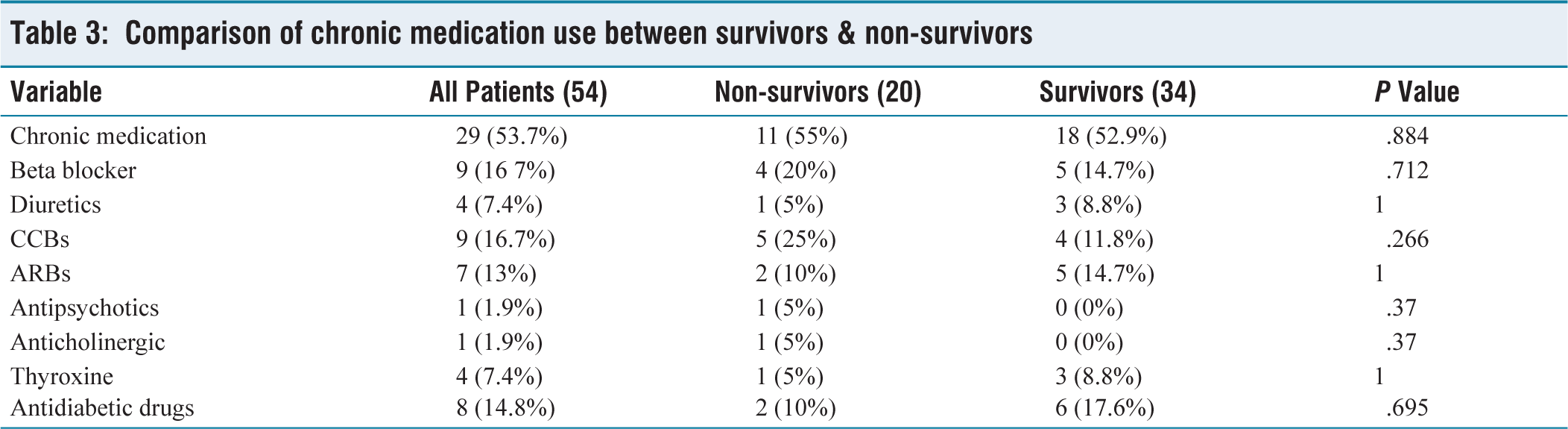
With regard to CM use, 29 patients (53.7%) were on at least one long-term medication before admission [Table 3]. The use of CM was similar in both groups: 55% in non-survivors and 52.9% in survivors (P = .884). No statistically significant associations were observed between survival status and the use of specific drug classes.
Comparison of chronic medication use between survivors & non-survivors
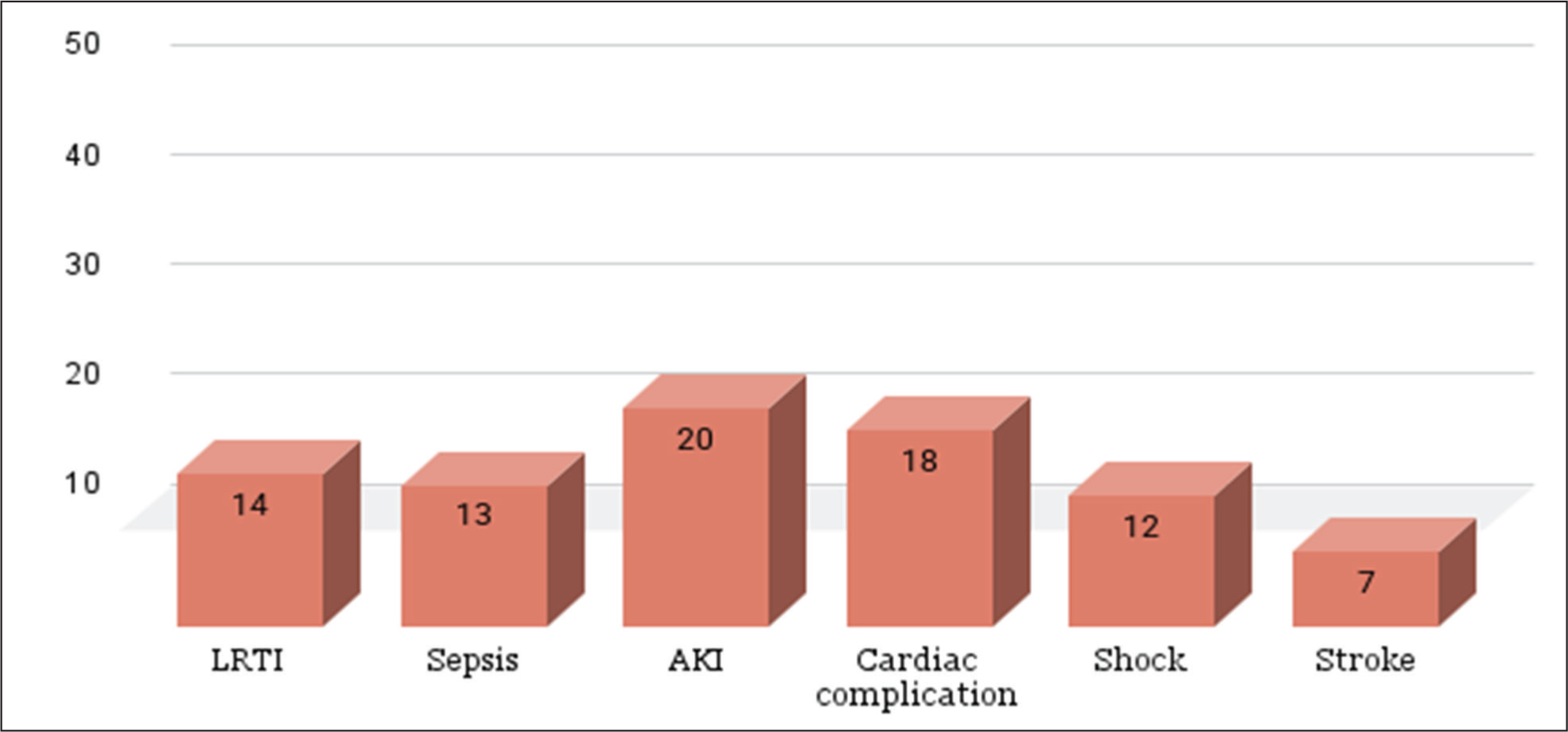
In this study, a wide range of complications were observed, reflecting the systemic impact of HRIs [Figure 3]. The most common complication was AKI, which occurred in 20 patients (37.0%), likely attributable to dehydration, rhabdomyolysis, or multi-organ dysfunction, followed by cardiac complications in 18 (33.3%), lower respiratory tract infections (LRTI) in 14 (25.9%) and sepsis was observed in 13 (24.1%) patients.
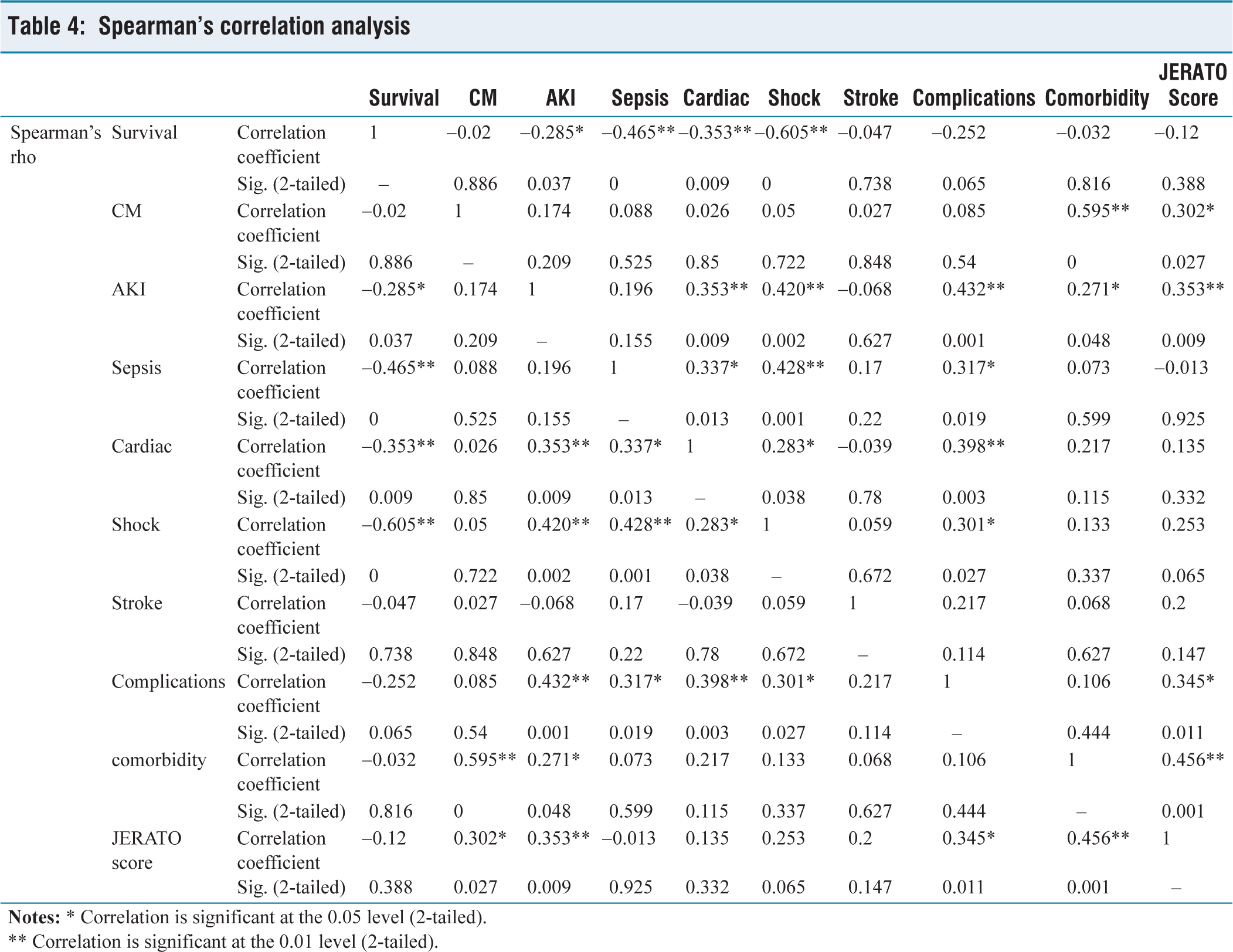
In patients with HRIs (n = 54), associations between survival, complications, comorbidities, pre-existing medications, and JERATO score were assessed using Spearman’s correlation analysis [Table 4].
Complications
Spearman’s correlation analysis
** Correlation is significant at the 0.01 level (2-tailed).
AKI, sepsis, cardiac complications, and shock all had negative correlations with survival, suggesting that these conditions considerably decreased the likelihood of survival. Although it was not directly related to survival, the JERATO score had a significant association with AKI, complications, comorbidities, and CM.
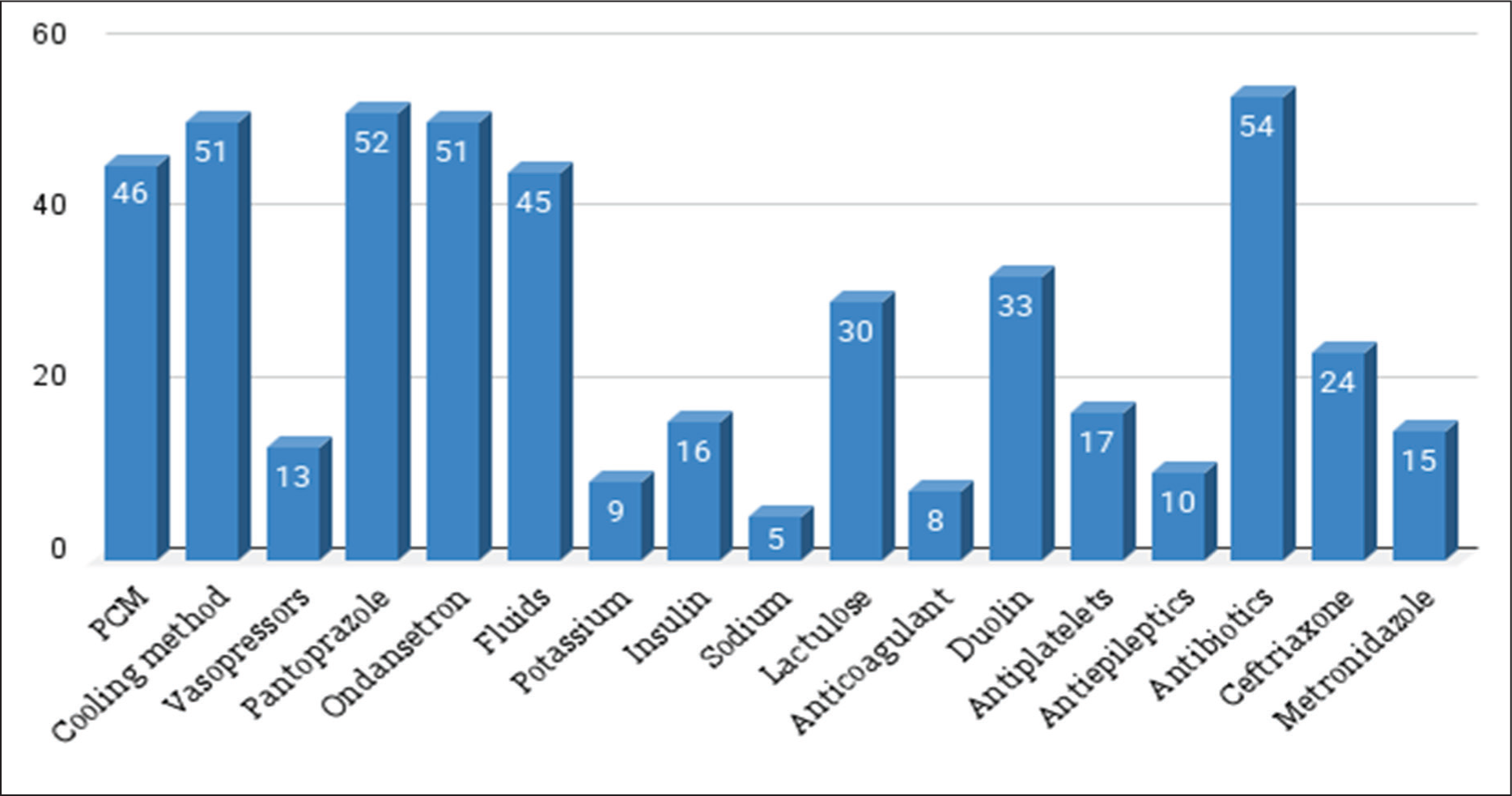
All patients received hospital-based care [Figure 4]. Antibiotics were prescribed to all patients; 44.4% received ceftriaxone, and 27.8% received metronidazole. Supportive therapy included intravenous fluids (83.3%), electrolyte correction (potassium chloride, KCl in 16.7%, sodium bicarbonate in 9.3%), Paracetamol (PCM) (85.2%), Pantoprazole (96.3%), Ondansetron (94.4%), and nebulised Duolin (61.1%). Insulin was used in 16 (29.6%) and Lactulose was prescribed in 30 (55.6%) patients. Other therapies included insulin (29.6%), lactulose (55.6%), vasopressors (24.1%), and antiepileptics (18.5%). Cooling methods were applied in 94.4% of cases. Antiplatelet agents were used in 31.5% and anticoagulants in 14.8% of patients.
Treatment modalities
Discussion
This is the first of its kind study done at our setup. In this study, we looked at how patients with HRI progressed during hospitalisation. The overall mortality in our study was 37%, consistent with previously reported figures in severe HRI, particularly among hospitalised or intensive care unit (ICU) populations.[10]
It is interesting to note that, while not statistically significant (P = .061), survivors in our cohort were slightly older than non-survivors. As per the majority of earlier studies, ageing is a predictor of poor outcomes because it impairs thermoregulation and decreases cardiovascular reserve.[11] This unexpected trend in our study may be due to earlier access to medical care among older individuals. Although the percentage of males in the non-survivor population was higher (60%) than in the survivors (50%), it was not statistically significant.
The heart rate and GCS were important indicators of mortality. In accordance with findings from previous studies, non-survivors had significantly lower GCS scores (P < .001), indicating more severe neurological impairment, and significantly higher heart rates (P = .008), which likely reflected systemic stress or early shock.[12,13] High core temperatures destabilise neuronal membranes, which increases permeability of the blood-brain barrier and neuroinflammatory cascades that lead to cerebral oedema and neuronal injury.[14]
Our complication profile is consistent with previous Indian cohorts reporting multi-organ involvement in HRIs, with AKI and cardiac events as the most common manifestations. The systemic impact of thermal injury was highlighted by (Titiyal et al.)[15] who reported that 44% of patients had renal dysfunction and nearly 78% had elevated hepatic enzymes, along with frequent rhabdomyolysis and coagulopathy.
Increased CPK levels in non-survivors point to more severe rhabdomyolysis, a known side effect of HRI caused by the breakdown of muscles under heat stress. Heat stress disrupts calcium homeostasis within myocytes, leading to protease activation, mitochondrial dysfunction, and ultimately cell death. Released myoglobin not only serves as a marker of muscle injury but also plays a vital role in the pathogenesis of AKI.[16] which explains why rhabdomyolysis and dehydration are frequent causes of AKI in these patients.
Similarly, higher serum creatinine and AST levels in non-survivors reflect renal and hepatic dysfunction. The hepatic damage in HRI is thought to result from multiple mechanisms, including direct thermal injury to endothelial cells and hepatocytes, ischaemic hepatitis from reduced splanchnic perfusion as blood is redirected to the skin for heat dissipation, and microthrombus formation, although the precise pathophysiology remains incompletely understood.[17] While markers like haematocrit, ALT, and urea trended worse in non-survivors, they did not reach statistical significance—possibly due to the limited sample size.
Comorbidities were common (63% of patients), with HTN and DM being the most frequent. Many epidemiological studies have shown that cardiovascular and cerebrovascular diseases, respiratory illnesses, and DM are linked to increased mortality and hospital admissions during periods of extreme heat. Through a variety of thermal stress-related mechanisms, these medical conditions may increase the risk of heatstroke.
People with cardiovascular diseases, for example, may have decreased cardiac output and altered peripheral circulation, which makes it harder for them to control their core body temperature because of impaired skin blood flow. Because diabetic neuropathy damages autonomic nerves, it affects the sweating response and skin blood flow, which restricts the skin’s ability to dissipate heat.[18] Despite these known physiological vulnerabilities, our study—consistent with previous research—did not find any significant associations between these medical conditions and the occurrence of heatstroke.
Many commonly used medications can impair the body’s ability to handle heat and increase the risk of falls. Strong anticholinergic effects of tricyclic antidepressants result in sedation, low blood pressure, and decreased sweating. SSRIs and SNRIs can impair heat perception and are linked to hyponatraemia. Additionally, anticonvulsants and antipsychotics decrease sweating, balance, and alertness, which raises the risk of falls and HRIs. Anticholinergic medications also affect cognition and thermoregulation. Electrolyte imbalances, hypotension, and dehydration can result from blood pressure medications such as ACE inhibitors and diuretics. These risks are particularly significant in older adults and during hot weather.[19] However, in our study, these medications did not have a significant impact on survival, possibly due to the small sample size or multifactorial compensation by clinical care.
Frequent complications included AKI, cardiac events, shock, and sepsis, all of which were negatively correlated with survival in Spearman’s analysis. This underlines the importance of prompt recognition and aggressive management of complications in HRI.
Interestingly, although the JERATO score correlated significantly with AKI, complications, comorbidities, and medication use, it did not predict mortality directly. This implies that other physiological and clinical factors may affect results, even though the score might represent severity. This result is in line with a prior study (Ninan et al.)[20] that discovered that the JERATO score was predictive of multi-organ dysfunction but not of mortality.
There remains debate about the role of empirical antibiotics in heatstroke. Because gut barrier compromise increases infection risk, in our study, all patients received antibiotics. Early infection is recognised as a key factor of morbidity and mortality in heatstroke, and when sepsis cannot be excluded, empirical coverage may be warranted, particularly in unstable patients with systemic involvement. Routine use, however, is not indicated, and stewardship principles dictate that therapy be de-escalated once microbiological results are available.[21,22]
All patients in our study received symptomatic management, including intravenous fluids, antibiotics, and individualised interventions such as vasopressors, insulin, and renal-protective measures (e.g., sodium bicarbonate). In addition, external cooling was uniformly implemented in accordance with institutional protocol, as it remains the cornerstone of heatstroke therapy. Rapid cooling is particularly critical in elderly patients, for whom conductive or evaporative techniques (such as cold fluid infusion, ice packs, wet sheets, and fanning) are generally better tolerated. Pharmacologic agents like antipyretics are ineffective in heatstroke and may even worsen outcomes. Organ dysfunction should primarily be managed with supportive care, as timely cooling frequently leads to reversal. In advanced or refractory cases, however, escalation to additional organ-supportive therapies may become necessary.[23]
These results demonstrate the growing threat to public health posed by rising temperatures and frequent heat waves. Public education regarding early warning signs of heat illness, staying hydrated, and avoiding exposure to the outdoors during periods of high temperatures should be an essential part of preventive measures. Reducing the growing burden of heat-related morbidity and mortality will require strengthening community-based cooling programmes and better integrating heat preparedness into existing medical and emergency response protocols.
Limitations
This study has several limitations. Being a single-centre and retrospective design, the findings may not be generalisable to other populations and regions. Small sample size (n = 54) reduces the statistical power to detect clinically important associations. The retrospective nature may introduce bias in documentation on certain variables (e.g., time to presentation, environmental exposure). Use of hospital-based data primarily reflected moderate to severe cases, while milder cases managed in the community may have been underrepresented.
Strengths
This is the first hospital-based cohort from our region to describe the in-hospital progression of HRI while linking each clinical outcome to plausible molecular mechanisms. Our findings show that cooling methods were applied in nearly all patients, reflecting strong adherence to evidence-based practice. Comorbidity and CM use, which are frequently underreported but are extremely important to vulnerable populations, were included in the study.
Conclusion
In this cohort of patients with HRI, neurological impairment, elevated heart rate, and biochemical evidence of rhabdomyolysis and organ dysfunction were significantly associated with mortality. While comorbidities and CM use were common, they were not independently associated with survival outcomes. Prompt supportive care and early detection of complications like sepsis, heart failure, and AKI are still essential. Future care should not only maintain this high rate of cooling but also focus on earlier initiation and standardised methods, ensuring patients benefit from the full protective potential of this intervention. To validate these results and improve risk prediction tools in HRI management, more prospective, multicentre research is necessary.
Footnotes
Data availability
The data supporting the findings of this study are not publicly available due to [privacy/ethical/legal restrictions] but can be made available from the corresponding author upon reasonable request and subject to institutional approvals.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed consent
Not applicable, as this was a retrospective study using anonymized data and did not involve direct patient contact or intervention.
Institutional ethical committee approval number
Ethical approval was obtained from the NHL Institutional Review Board (Approval Number: NHLIRB/2024/Sept/25th/no-05 already included in the cover letter).
Credit author statement
Vrunda T. Parikh: Conceptualisation; Methodology; Definition of intellectual content; Literature search; Data acquisition; Data analysis; Statistical analysis; Writing - original draft; Writing - review & editing.
Riya S. Shah: Conceptualisation; Methodology; Definition of intellectual content; Literature search; Data acquisition; Data analysis; Statistical analysis; Writing - original draft; Writing - review & editing.
Sapna D. Gupta: Conceptualisation; Methodology; Definition of intellectual content; Literature search; Writing - original draft; Writing - review & editing.
Bhavesh S. Jarwani: Writing - original draft; Writing - review & editing.
Ami P. Parikh: Writing - original draft; Writing - review & editing.
Supriya Malhotra: Writing - original draft; Writing - review & editing.
Use of artificial intelligence
The authors used Quillbot for language editing of the manuscript draft.