
Abstract
Background
This study aimed to describe the clinical characteristics and epidemiology of heat-related illnesses presented at a tertiary hospital in Singapore.
Method
This retrospective observational study utilized electronic health records from the emergency department (ED) of Singapore General Hospital. Patients primarily diagnosed with heat-related illnesses from 2008 to 2020, were analyzed. The annual number of cases and the temporal trend of heat-related illnesses were described, along with the characteristics of patients.
Results
Among the 1,833,908 patients registered at the ED, 426 patients had diagnoses of heat-related illnesses. The median age (interquartile range [IQR]) was 32 (22, 43) years, with 303 (71%) being male and 201 (47%) not being Singapore citizens. The annual number of cases ranged from a minimum of 21 in 2019 to a maximum of 49 cases in 2015, except for four cases in 2020. Heat-related illnesses occurred most commonly on Sundays (233, 55%) and in December (97, 23%). A significant number of cases in December coincided with the day of an annually organized marathon (91, 21%). Approximately half of the total cases required hospitalization, with 183 (43%) admitted to the general ward and 31 (7%) admitted to the intensive care unit. The 30-day mortality was 2 (0.5%).
Conclusion
This descriptive study indicated the unique characteristics of heat-related illness in a tertiary care hospital in Singapore. These local contexts may be valuable to consider preventative measures for heat-related illness, in preparation for future extreme weather events related to climate change.
Keywords
Introduction
Heat-related illnesses, including heat cramps, heat exhaustion, heat syncope, and heat stroke are emergency conditions that can result from exposure to a hot and humid environment. 1 With the increasing severity of heatwaves worldwide due to climate change, the incidence of heat-related illnesses is on the rise, and more than 166,000 people have died due to heatwaves between 1998 and 2017. 2 Consequently, heat-related illness has become a significant challenge in public health. Close understanding of its clinical characteristics and epidemiological features is an important step in its prevention and prompt recognition, leading to appropriate medical management.1–3
As the population is aging, heat-related illness happens particularly for individuals older than 65 years with chronic health problems. 1 In Japan in the 2000s, for instance, the occurrence of heat-related illnesses was predominantly in young individuals who participated in sports activities or outdoor work (Exertional heat illness).1,4,5 However, the scenario has changed in 2015 with more than half of the reported cases now involving older individuals in indoor settings or during their daily activities (Classical heat illness).1,5–9 Similarly in the United States and Australia, most heat-related deaths are recorded among individuals aged 65 years and older.3,10 Consequently, older adults are a vulnerable population that requires particular attention in heat-related illness prevention efforts.
Moreover, the severity of the heat-related illness can range from minor to life-threatening, with high associated mortality if severe cases are not promptly recognized and treated. 1 Previous studies in Japan have reported the clinical characteristics of severe cases, revealing an overall mortality rate of 4%–8%.6–8,11 These severe cases often present with a body temperature exceeding 40°C, altered consciousness, and impaired liver and kidney function.6,7,8 Thus, heat stroke occurs in diverse patient populations according to the characteristics of each region, and the clinical picture differs, so it is necessary to understand the characteristics of patients in each region and to consider prevention and response measures.
However, limited information is available regarding the occurrence of heat-related illnesses among the general population in Singapore. A previous study developed a prediction model for the occurrence of heat-related illness based on weather conditions using data from 1991 to 2010; however, it did not aim to investigate patient characteristics. 12 The other studies primarily focused on the military settings.13,14,15 There is presently a knowledge gap on the epidemiological features and characteristics of heat-related illnesses in Singapore. The present study aims to describe the epidemiological features of occurrence and characteristics of heat-related illness presented at a tertiary medical center in Singapore.
Methods
This study was approved by Singapore Health Services’ Centralized Institutional Review Board (ID: CIRB Ref: 20201/2122), and a waiver of consent was granted for data collection and analysis because of the retrospective nature of the study.
Study design, settings, data source
This was a retrospective analysis of the database of patients who attended the emergency department (ED) of Singapore General Hospital (SGH). Singapore is a city-state in Southeast Asia and the SGH is the largest and oldest public tertiary care hospital in Singapore and the flagship hospital of SingHealth which is the country’s largest group of three public healthcare sectors in Singapore. SGH ED mainly covers the south and central areas of Singapore and receives more than 120,000 visits and has 36,000 inpatient admissions annually. 16 This study used the database that included all the patients who visited or were transferred to the SGH ED between January 2008 to December 2020. The database was developed by extracting the clinical data from the hospital’s electronic health record using the SingHealth electronic health intelligence system to build the machine-learning triage system.17,18
Study population
This study included patients primarily diagnosed with heat-related illness among the patients who attended the ED of SGH between January 2008 to December 2020 and registered in the database. The primary diagnosis of heat-related illness was defined by the description of the heat-related illness including heat cramps, heat exhaustion, heat syncope, heat stroke, and sunstroke in the first-line or second-line primary diagnosis category.
Data management
We extracted the available clinical data as follows: age, gender, nationality, date and time of ED registration, the diagnosed type of heat-related illness (heat stroke, heat exhaustion, heat cramps, heat syncope, and others), the Charlson comorbidity index, triage class (P1, P2, P3, and P4), primary ED diagnosis, vital signs (systolic blood pressure, pulse rate, body temperature), laboratory data at the ED admission (creatinine, potassium) if it was available, disposition (discharge from ED, admitted to the ward, or ICU), length of hospital stay, and 30-day mortality.17,18 The detailed explanation of variables is shown in supplementary file (S-Method 1). Based on the registration date, we divided the date of incidence into weekdays and weekends (Sunday and Saturday). As we have experienced multiple cases occurring in a single day such as the day of the Singapore Marathon, we summarized the number of cases that happened on the day of the Singapore Marathon and related events.
Weather data
We also showed some summary data of weather conditions below for reference. We extracted the annual and monthly trend of the mean, maximum, and minimum daily air surface temperature, and relative humidity from the Singapore government open data site (https://beta.data.gov.sg/). Generally, wet bulb globe temperature is commonly used as the index to show the risk of heat-related illness; however, it is not available on the website above. 19 Instead of that, we obtained an hourly trend of wet bulb temperature (WB temperature). WB temperature is the lowest temperature a portion of air can acquire by evaporative cooling only, and the 30°C of WB temperature in hot and humid conditions is reported as a critical limit for human adaptability. 20
Statistical analysis
First, we described the patient characteristics for the variables mentioned above using the median and interquartile range (IQR) for continuous variables and number with proportion for the categorical variables for the variables mentioned above. We indicated the missing as “unknown” or “missing” and also showed the availability of the blood test results in the table describing patients characteristics. Second, to better understand the patterns and trends in the occurrence of heat-related illnesses, we showed the number of cases of heat-related illness and several time spans (annually, monthly, daily, and hourly) by the following subgroups: weekday/weekend, and age categories (<18, 18–39, 40–64, 65 or more years), because heat-related illnesses manifest differently across countries due to seasonal or temporal trends and can affect various age groups.1,4,5,6,7,8,9,21 We also summarized the number of cases that occurred in a single day. Third, to investigate the clinical features of minor or severe cases, we showed the trend of number of the cases and boxplots of the vital signs and laboratory data by severity (disposition, type of heat-related illness, and triage category). A sample size estimation was not performed since this study did not intend to test a specific hypothesis. All statistical analyses were performed with R software, version 4.1.2 (R Foundation for Statistical Computing).
Results
Basic demographics and those by age groups
Patients characteristics by age category.

AU/NZ: Australia and New Zealand; The SG Marathon: day of the Singapore marathon and related events generally held in 1st week of December.
Overall timely trend and by age groups
The annual number of cases ranged between a minimum of 21 in 2019 and a maximum of 49 cases in 2015, except for only four cases in 2020, which was during the coronavirus pandemic period (Figure 1, S-Results 3). The most common timings were weekends (284, 67%), especially on Sundays (233, 55%), during the daytime (8:00–16:00, 249, 58%), and surprisingly in December (97, 23%), which is the month with relatively lower temperature. The Singapore marathon and related sports events are usually held on the weekend of the 1st week in December, and almost one in four cases happened on the day of the Singapore marathon or related events (91, 21%) (Figure 1 and S-Results 3 in Supplementary file). Throughout all time periods, most cases occurred in young or middle-aged adults, and there was no apparent specific timing for the occurrence of cases in younger (<18 years) or older (≥65 years) individuals (Figure 1). Time trend of heat-related illness by age category. Temp, mean daily air surface temperature, WB Temp, Water bulb temperature.
Trend: Weekday/weekend
Heat-related illness cases consistently occurred on weekdays throughout the year, but more cases were observed, particularly during the dry season from March to August when the mean air temperature was higher compared to other periods (Figure 2). In contrast, cases on weekends were concentrated from August to December. Regarding the timing within a day, cases on weekdays were mainly observed in the afternoon to evening when temperatures peaked and remained high, while cases on weekends were consolidated in the morning as temperatures were rising (Figure 2). There were no notable differences in patient characteristics between weekdays and weekends (S-Results 4). Time trend of heat-related illness by the weekday and weekend. Temp, mean daily air surface temperature, WB Temp, Water bulb temperature.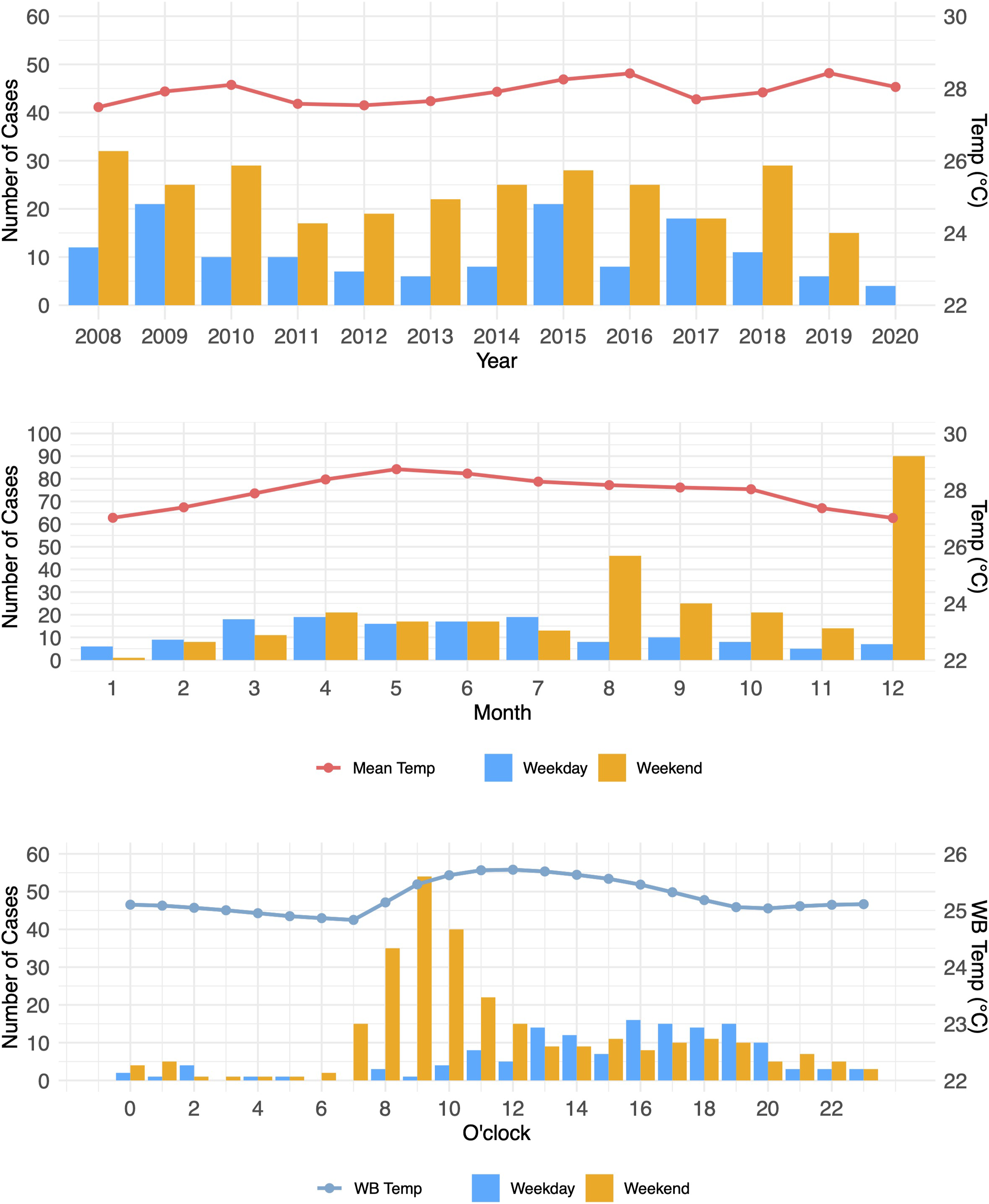
Multiple cases occurred on the same day
During the survey period, there were 259 days with reported cases of heat related illness. The breakdown of these days is as follows: 204 days with one case, 29 days with two cases, 7 days with three cases, and 19 days with four or more cases. A maximum of 15 cases happened on the same day. Of 19 days with four or more cases, all the days were weekends, 11 days were in December, and 12 days were days of the Singapore Marathon and related events.
Clinical features of the patients with heat-related illness
Clinical information by disposition.
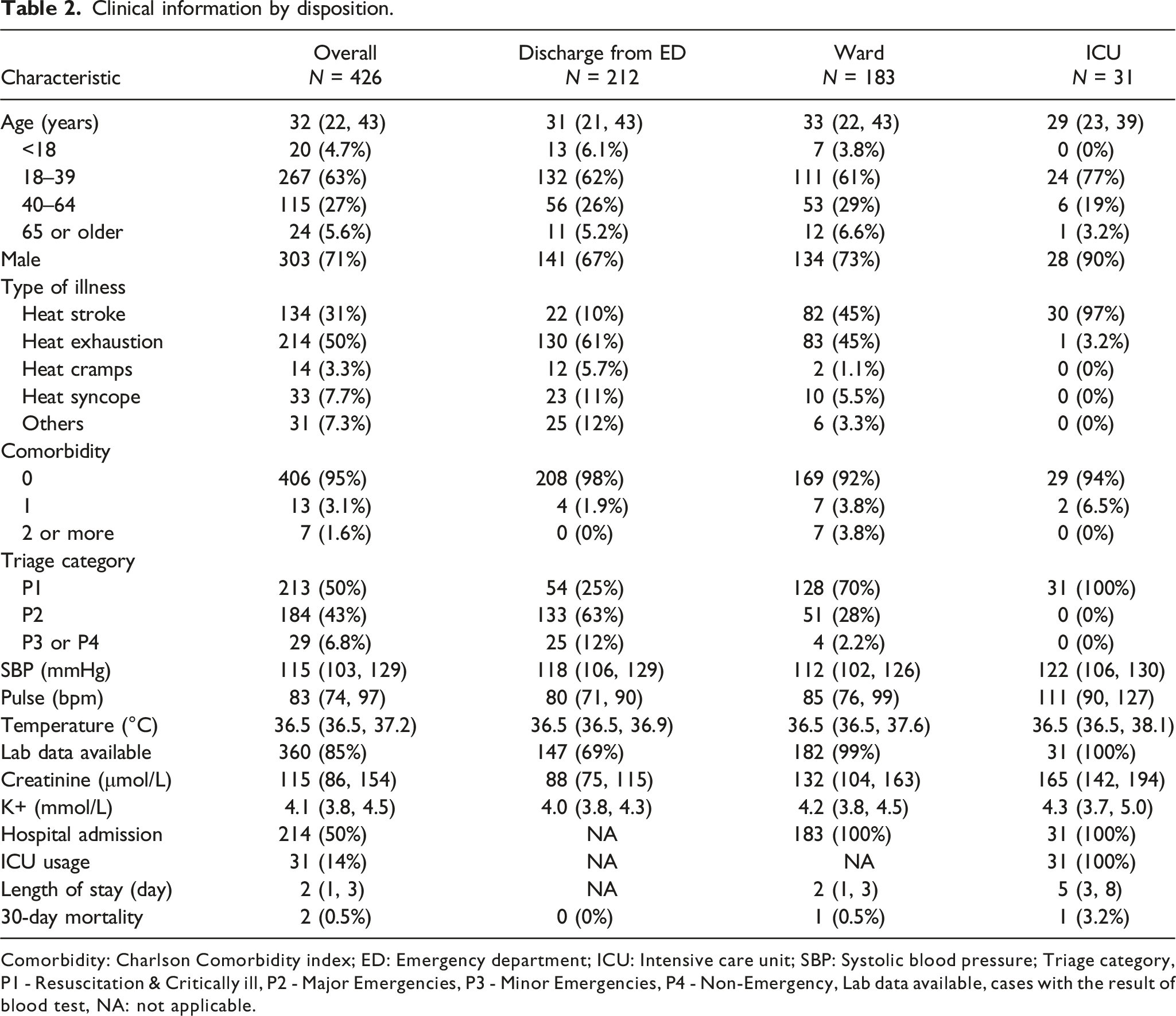
Comorbidity: Charlson Comorbidity index; ED: Emergency department; ICU: Intensive care unit; SBP: Systolic blood pressure; Triage category, P1 - Resuscitation & Critically ill, P2 - Major Emergencies, P3 - Minor Emergencies, P4 - Non-Emergency, Lab data available, cases with the result of blood test, NA: not applicable.

The vital signs and laboratory data of heat-related illness. ICU: Intensive care unit; Cr: Creatinine; K+: Serum potassium. The patients admitted to the ICU have higher pulse rates and higher creatinine values suggesting dehydration and acute kidney injury.
Other detailed epidemiological data regarding time trends, the patients characteristics, and clinical information by the disposition, type of heat-related illness, and triage category were shown in the supplementary file (S-Results 5).
Discussion
Key findings and strengths
This observational study about heat-related illness in the central area of Singapore showed several unique features of occurrence. Firstly, most patients were adults between 18 and 64 years, the older population was limited, and nearly half of the patients were not Singaporean. Secondly, multiple incidents in the morning on weekends especially in December, are often associated with sports events. Thirdly, half of the cases resulted in admission to the hospital, which may be attributed to dehydration and acute kidney injury; however, the case with mortality was rare. Since few studies about the epidemiology of heat-related illness in Singapore were previously performed, this study has novel and original clinical insight into the trend of heat-related illness in the central area of Singapore and is expected to be valuable, especially for discussing preventive measures considering the regional contexts.
Interpretation and clinical implication
This study suggests that most of the patients suffered from the type of exertional heat illness, which is typically induced by vigorous physical activity in hot or humid environments. In contrast, classical heat illness, which typically affects older populations during their daily activities, is less common in Singapore. This differs from other East-Asian countries where the majority of patients are older individuals. For example, in Japan, approximately 60% of heat-related illness patients are over 65 years old which is considerably higher than in Singapore.6–8 Even in Korea in which the proportion of the older population was comparable to Singapore (14.9% in Korea, 2019 vs 14.4% in Singapore, 2019), 22 the most affected age group is in their 50s (24%), and nearly 60% of heat-related illness cases involve individuals over 50 years old. 21
One potential explanation we guess for this difference is that people in Singapore are physiologically and behaviorally adapted to the tropical climate in their daily life while the vulnerable people in Japan or Korea especially the older population have the difficulty adapting to hot and humid environments related to seasonal climate changes. Adaptation to the heat and environment (heat acclimation) is an essential process to reduce the risk of serious heat illness and it includes physiological adaptations such as adjusting thermoregulation to produce a greater amount of sweat, and behavioral adaptations such as avoiding unnecessary exposure to sunlight or heat, preventing the body temperature become high using fan or air conditioning and drinking water.23,24,25,26,27 In countries like Japan and Korea, temperatures fluctuate significantly between seasons. In Japan, maximum temperatures can exceed 35°C during the summer (July to September), while dropping below 10°C in winter (December to February). 28 Consequently, people in East-Asia need to adapt physiologically and behaviorally to heat exposure based on seasonal changes. However, in Japan, some vulnerable populations such as the elderly, may struggle to adapt to the heat, resulting in a higher incidence of heat-related illnesses especially when temperatures start to rise in early July.6,7,8 Furthermore, people living in the north side of Japan with lower temperatures were reported to have a higher risk of heat-related illness than those in southern regions with subtropical climates potentially due to a lack of adaptation to hot and humid environments. 29 In contrast, while Singapore experiences some seasonal temperature trends, it remains consistently hot and humid throughout the year. Therefore, it was understandable that most cases were not elderly people but were observed in situations associated with special circumstances such as sports events on weekends.
Notably, the study revealed that approximately one-fourth of the patients were individuals from countries which are non-tropical climates such as East Asia, the EU, and North America. Although it was unclear whether they were travelers or residents in Singapore, this result supports the hypothesis that people who recently traveled from cooler climates need to exercise greater caution, as mentioned in an advisory for managing heat stress from the National Environment Agency in Singapore. 19 These unique aspects may highlight the importance of implementing measures to prevent heat-related illnesses for special populations without adapted to hot and humid environment as well as typical cases of exertion-related illness like people working in outdoor settings during daytime. Further, the results also suggested the necessity of preparing the ED for multiple cases related to special circumstances such as mass-gathering events or sports events.
Limitations and future directions
This study has several limitations. First, this study was not population-based data; thus, the incidence or trend per population is not available. Second, the study focused on patients who presented to our ED and may not capture all cases of heat-related illness in the community. Third, the diagnosis of heat-related illness was based on the description in the medical chart on diagnosis by physicians in charge, and there had been no standardized diagnostic criteria or independent adjudication. Sometimes, it is challenging to accurately differentiate heat-related illness from patients with infection or sepsis in the ED phase. Accordingly, there might have been the risk of bias in the process of patient selection. Fourth, due to the nature of retrospective data collection, some clinical information was not available, especially, since blood test result in some cases was unavailable. Furthermore, the occupation of the patients, situation of incidence, or in-hospital management are also helpful information for discussing preventive measures or treatment; however, this kind of information was not available. Also, the data about treatment for severe cases in ICU were not available. Fifth, this study was a single-center study only covering the south and central areas of Singapore; thus, it might be difficult to generalize the results to other areas in Singapore.
Currently, the climate is dramatically changing and the day with extreme heat weather is increasing, we are anticipating more cases of occurrence of heat-related illness. Future research should consider conducting prospective studies to obtain more accurate and comprehensive data on the epidemiology of heat-related illnesses in Singapore, especially exploring the underlying mechanisms and risk factors associated with heat-related illnesses in specific population subgroups, such as outdoor workers or vulnerable populations, which could provide valuable insights for targeted interventions.
Conclusion
This descriptive study indicated the unique characteristics of heat-related illness in a tertiary care hospital of Singapore. These local contexts may be valuable to consider preventative measures for heat-related illness, in preparation for future extreme weather events related to climate change.
Supplemental Material
Supplemental Material - Heat-related illness in Singapore: Descriptive analysis of a tertiary care center from 2008 to 2020
Supplemental Material for Heat-related illness in Singapore: Descriptive analysis of a tertiary care center from 2008 to 2020 by Yohei Okada, Joel Aik, Andrew Ho Fu Wah, Yilin Ning and Marcus Eng Hock Ong in Proceedings of Singapore Healthcare
Footnotes
Acknowledgements
We thank A/Prof Nan Liu for contributing to the data management.
Author contributions
Y.O.: conceptualization, formal analysis, and writing the manuscript, J.A.: review and editing, A.H.F.W.: review and editing, Y.N., data curation, and M.E.H.O.: supervision, conceptualization, data curation, review, and editing.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: YO has received a research grant from the ZOLL Foundation and overseas scholarships from the Japan Society for Promotion of Science, the FUKUDA Foundation for Medical Technology, and the International Medical Research Foundation. MEHO reports grants from the Laerdal Foundation, Laerdal Medical, and Ramsey Social Justice Foundation for funding of the Pan-Asian Resuscitation Outcomes Study an advisory relationship with Global Healthcare SG, a commercial entity that manufactures cooling devices; and funding from Laerdal Medical on an observation program to their Community CPR Training Centre Research Program in Norway. MEHO is a Scientific Advisor to TIIM Healthcare SG and Global Healthcare SG. These funds had no role in conducting this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the scientific research grant from the JSPS KAKENHI of Japan (JP23K16253).
Ethics statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.