
Abstract
Introduction:
Musculoskeletal trauma is frequently encountered in the emergency department and can lead to significant disability if not treated properly. The spectrum of trauma includes fractures, joint dislocations and injuries of soft tissue structures like muscles, ligaments, tendons, labrum, etc.
Methods:
In this article, we provide a comprehensive review of the spectrum of musculoskeletal injuries and their imaging appearance. The main clinical applications and limitations of various imaging modalities in evaluation of musculoskeletal trauma will be discussed.
Results:
Plain radiograph remains the primary modality in the evaluation of bone injuries. Ultrasonography is highly sensitive in assessing superficial soft tissue injuries with the advancement of high-resolution probes. Computed Tomography with multiplanar and 3D reconstruction is being widely used in complex fractures, spine injuries and as a part of pre-surgical workup. MRI continues to be the gold standard in evaluation of trauma to soft tissue structures like ligaments, tendons, labrum and cartilage owing to its high soft tissue contrast.
Conclusion:
The choice of optimal imaging modality is critical in the accurate diagnosis of the extent and severity of trauma, thereby influencing management decisions, resulting in better patient outcomes.
Abbreviations
MRI: Magnetic resonance imaging
CT: Computed tomography
US: Ultrasonography
POCUS: Point-of-care ultrasound
3D: Three-dimensional
Tc-99m MDP: Technetium-99m methylene diphosphonate
SPECT: Single-photon emission computed tomography
PET: Positron emission tomography
ER: Emergency room
T1WI: T1-weighted imaging
Introduction
Musculoskeletal trauma constitutes one of the major components of Orthopaedic Radiology, contributing to a significant proportion of workload in day-to-day practice. The trauma can involve bones, joints, ligaments, tendons, muscles, cartilage, labrum or neurovascular structures. Sometimes the injury may be in the form of a minor fracture or minimal soft tissue injury, which is easy to heal. However, major musculoskeletal trauma may result in limb deformities or significant residual morbidity if not properly treated. Prompt and accurate assessment of bone or soft tissue injury by imaging is the cornerstone of optimal management of musculoskeletal trauma.[1] Although plain radiography has been the primary modality for many years,[2] imaging in musculoskeletal trauma has advanced by leaps and bounds in the last 20 years. One major contributor to this advancement is the advent and widespread use of helical multidetector CT, which resulted in multiplanar image reconstruction.[3] Another significant change is refinement of MRI with faster acquisition times and more specific sequences.[4]
Mechanisms of Trauma
The knowledge of mechanism of injury is highly essential before imaging, as it provides insights into the possible structure involved and severity of injury. There is a wide range of mechanisms which can result in musculoskeletal trauma.[5]
Blunt trauma with high-energy impact usually results from motor vehicle accidents, falls from height or sports collisions. It usually results in fractures, bone contusions or joint dislocations. Occasionally, low-energy trauma such as a fall from standing height or less can lead to fractures, particularly in the setting of osteopenia. Twisting injuries can result in ligament injuries. Repetitive trauma in athletes can lead to stress fractures.
Certain mechanisms and types of trauma may be specific to certain ages of the patients. Non-accidental injuries are seen in infants. Salter-Harris injuries are seen in children or adolescents, where growth plates are not fused. As these growth plates or physes are responsible for longitudinal bone growth, the Salter-Harris fractures may result in growth disturbances.[6] In general, young population is more prone to sports-related injuries, whereas the older population is susceptible to insufficiency fractures on account of osteoporosis.
Types of musculoskeletal trauma based on anatomical structure involved:
Bones: Fracture is the most common type of bone injury, which is defined as a breach in continuity of cortex. The fracture can be open or closed, based on whether the fracture fragment penetrates the skin or not. A fracture is described as open when it penetrates skin and is in contact with outside environment. Fractures can be described as complete or incomplete. Complete fractures extend across the bone. Complete fractures are described as transverse, oblique or spiral based on orientation of fracture line, relative to bone axis. Another type of complete fracture is a comminuted fracture, where the fracture results in more than two fragments. Incomplete fractures do not cross the bone completely and are commonly seen in children. Incomplete fractures are of three types: Greenstick fracture (cortical breech only on one side), Torus fracture (buckling of cortex) and plastic bowing fracture (deformed bone without cortical break).[7] Stress fracture (fatigue fracture) is the result of abnormal repetitive stress on normal bone, in locations like anterior cortex of tibia (shin splint), 2nd to 4th metatarsal heads (March fracture), etc.[8] Avulsion fractures are due to application of tensile force on musculoskeletal unit or ligament. They are more common in skeletally immature individuals due to weakness of apophyses, although they can occur in adults, usually at tendon attachment sites, particularly when there are degenerative tendon changes.[9] Bone contusion is another important pattern of bone injury, due to trabecular compression microfracture, causing oedema or haemorrhage within the bone marrow, without a visible fracture line. The pattern of contusion can be a footprint of underlying soft tissue injury, particularly in the knee joint.[10] Joints and Intra-articular structures: Joint injury can be in the form of subluxation or dislocation. Labrum, cartilage and ligaments are the intra-articular structures which may be injured. Cartilage has a low capacity to heal, as it is relatively less vascularised than other structures. Cartilage injury, if untreated, leads to early osteoarthritis. Osteochondral injuries, which involve articular cartilage and subchondral bone injury, are also included in the spectrum of intra-articular injuries. Soft tissues: Muscle injury can be in the form of a simple strain, which manifests as oedema, or it can be in the form of a partial tear or complete tear. Tendon injury can be in the form of laceration, partial or complete rupture. Retraction of torn ends is an important factor which determines the treatment plan and outcome. Neurovascular structures: Neurovascular injury may be associated with musculoskeletal trauma. Nerve injury can be graded as neuropraxia, axonotmesis or neurotmesis.[11] Occasionally displaced bone fragment or haematoma may cause compression or entrapment of neurovascular structures.
The Goals of Imaging in Musculoskeletal Trauma
In cases of trauma, imaging helps to detect the presence of fracture, to describe the exact site, extent and type of fracture. It also helps to identify if there is any soft tissue injury, to describe and grade the injury. Imaging is crucial to identify and report emergencies like cervical spine trauma, which may compromise spinal cord and to identify any fracture, which may result in acute, uncontrolled bleeding or neurovascular compromise.
Detailed knowledge of various types of musculoskeletal trauma and their imaging appearance is important in prompt recognition of these injuries. The role of different imaging modalities, their advantages and limitations are discussed here.
Various imaging modalities in musculoskeletal trauma:
Plain radiograph Ultrasound Computer tomography MRI Nuclear scintigraphy
Plain Radiograph
Plain radiograph is the most important and primary investigation in cases of extremity skeletal trauma. AP, lateral and oblique views are most commonly used. However, special views like scaphoid view of wrist, axillary view of shoulder, etc., may need to be used depending on site of injury. The main advantage of a plain radiograph is that it is widely available, simple, economical, and requires only basic skills for interpretation.[1]
Applications
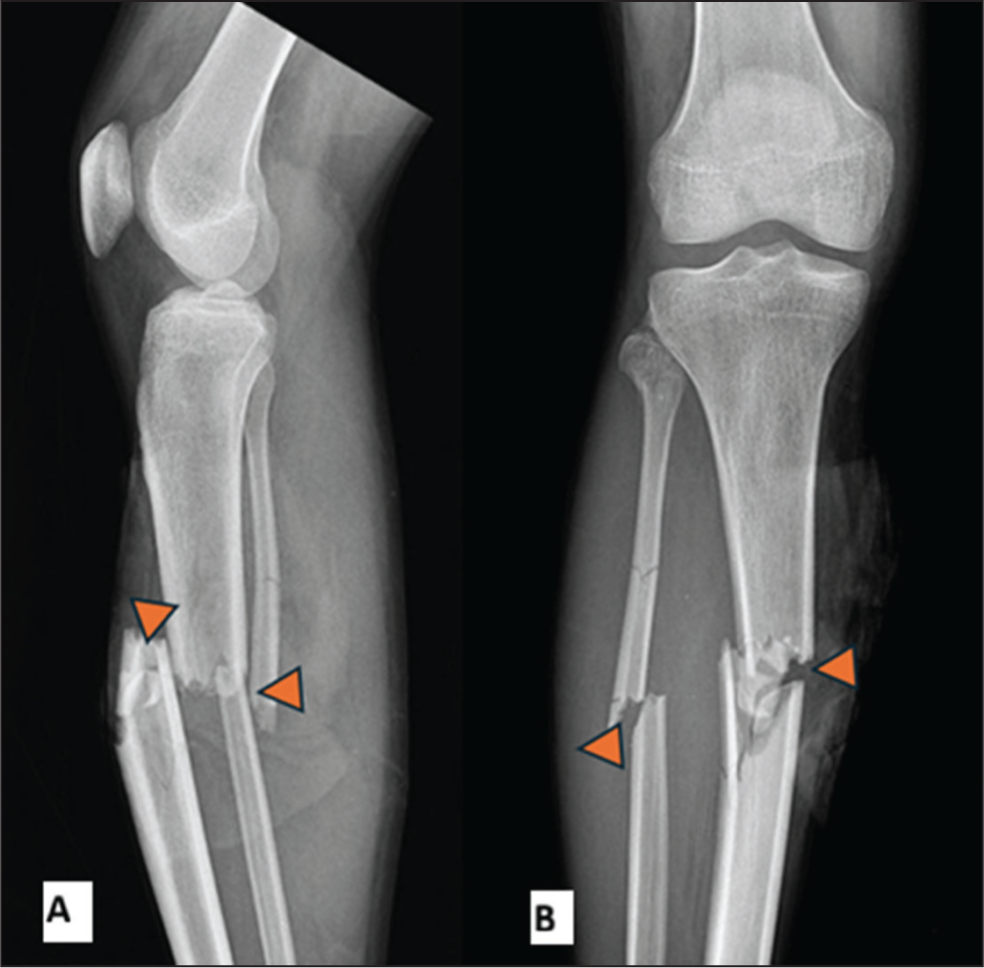
Plain radiograph can detect the presence of a fracture and can describe type, extent of fracture [Figure 1]. It is useful in assessing joint injuries like dislocation or subluxation. It can detect soft tissue changes like soft tissue haematoma or hemarthrosis. Radio-opaque foreign bodies in soft tissue and air foci in soft tissues due to surgical emphysema can be detected.
Lateral (A) and Antero-posterior(B) views of right leg X-ray showing both bone comminuted fractures () with marked displacement
Limitations
Plain radiograph has less sensitivity in detecting subtle fractures or stress fractures. It may be difficult to interpret fractures of complex anatomical parts like pelvis, skull and spine, due to bone overlap. Poor sensitivity to detect soft tissue injury is another limitation. A major disadvantage of a radiograph is that it involves ionising radiation.
Ultrasound
Ultrasound is the primary modality for evaluation of superficial soft tissue trauma. With the rapid development of technology and high-frequency probes, the US has gained a significant reputation in demonstrating soft tissue injuries.
The main advantage of Ultrasonography is that it is non-ionising. It is less costly when compared to CT and MRI, widely available and non-invasive. Point-of-care Ultrasound (POCUS) can be done bedside in emergencies. Dynamic ultrasound allows the examination of suspected anatomical structures while in motion. This is particularly helpful in a few situations when the abnormality does not appear when the structure is at rest, for example, shoulder impingement, biceps tendon subluxation, etc. The possibility to directly examine the area of maximum tenderness and ease to compare with the normal side are the other potential advantages of Ultrasonography. It is the best modality for repeated follow-ups due to low cost when compared to MRI, non-ionising nature and wide availability. It can be an alternative modality for MRI to assess soft tissue injuries in very young paediatric patients to obviate the need for sedation.[12]
Applications
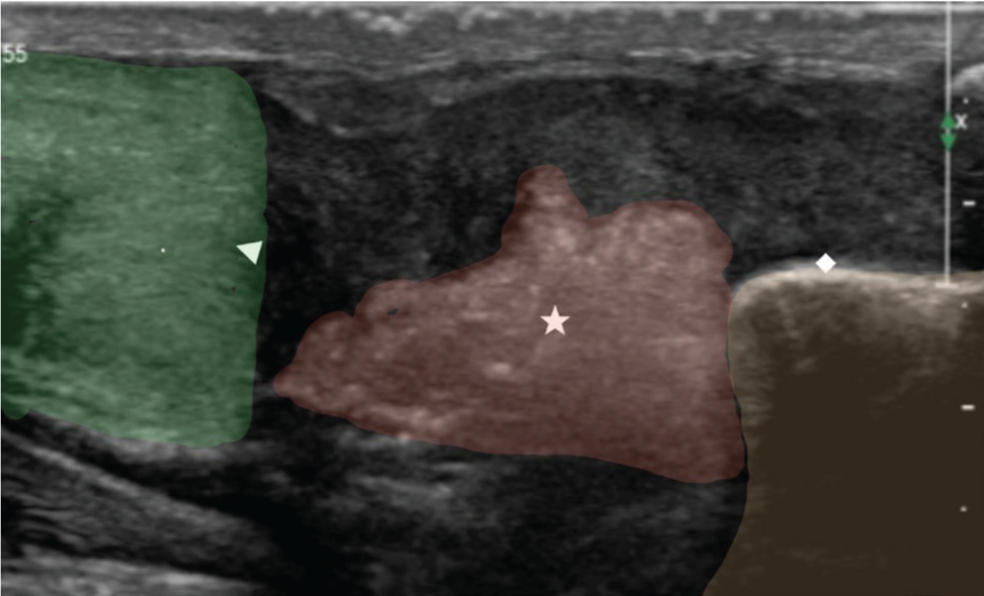
With its high resolution, ultrasound is an excellent modality to assess injuries of muscles and tendons. It is highly efficient in the differentiation of partial and total tears of muscles and tendons [Figure 2]. We can detect and quantify soft tissue haematomas using US. Foreign bodies in superficial soft tissues can be clearly depicted. Joint effusion or hemarthrosis can be detected and quantified. The US is also useful to depict subtle fractures as areas of cortical disruption. Nerves can be examined along their course to demonstrate and grade nerve injuries. Doppler can be used to assess vascular injuries or vascular entrapment caused by trauma without the need for intravascular contrast.
US of the ankle shows a complete Achilles tendon tear (Δ) with retraction of fibres from calcaneal () insertion and hematoma (☆) formation
Limitations
Inability to assess deeper structures, particularly in patients with thick body habitus, is a limitation for US. Inability to assess bone marrow oedema is another limitation. It is operator-dependent, as it needs high expertise, with a steep learning curve. There is a lack of knowledge of musculoskeletal applications amongst referring clinicians and amongst a few Radiologists.
Role of Computed Tomography in Musculoskeletal Trauma
With the advent of multidetector CT, voxels of near-isotropic volume can be obtained, which led to efficient multiplanar imaging. Post-processing techniques like 3D CT and Volume Rendered CT are the other most important developments in CT in trauma imaging. Its high resolution, high sensitivity and specificity make CT a valuable technique in evaluation of skeletal trauma. Short scan time is another significant advantage, particularly in unstable patients with polytrauma, where delay in taking multiple radiographs may result in loss of crucial time.[13]
Applications
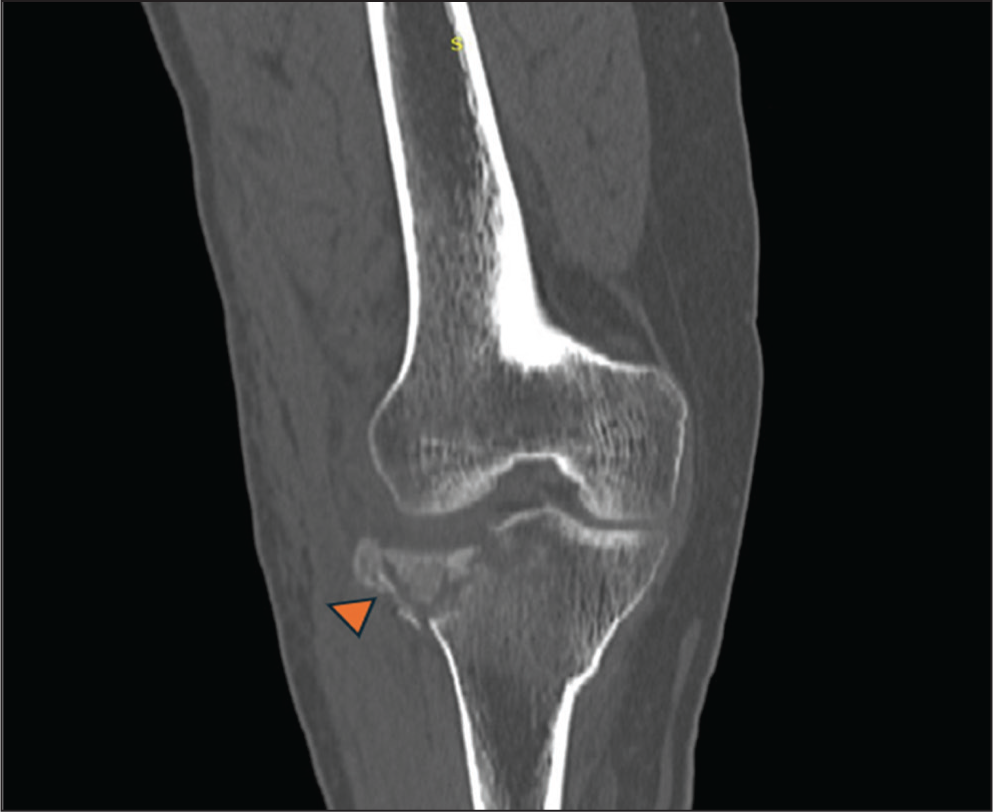
CT can detect or exclude subtle fractures which are occult on radiographs. It can help in the detailed evaluation of fractures of complex structures like pelvis, shoulder joint, cranio-facial bones and spine, where there is superimposition of multiple anatomical structures limiting visibility on plain radiograph. 3D and volume rendered images are crucial in grading and classifying the fractures, which help in surgical planning of complex trauma by demonstrating the plane of fracture, number of displaced fragments, degree and direction of displacement [Figures 3 and 4]. It helps in assessing avulsion fractures. It can detect major soft tissue injuries and hematomas, although with low sensitivity.
Volume rendered CT image of the left shoulder showing a comminuted fracture of the proximal humerus
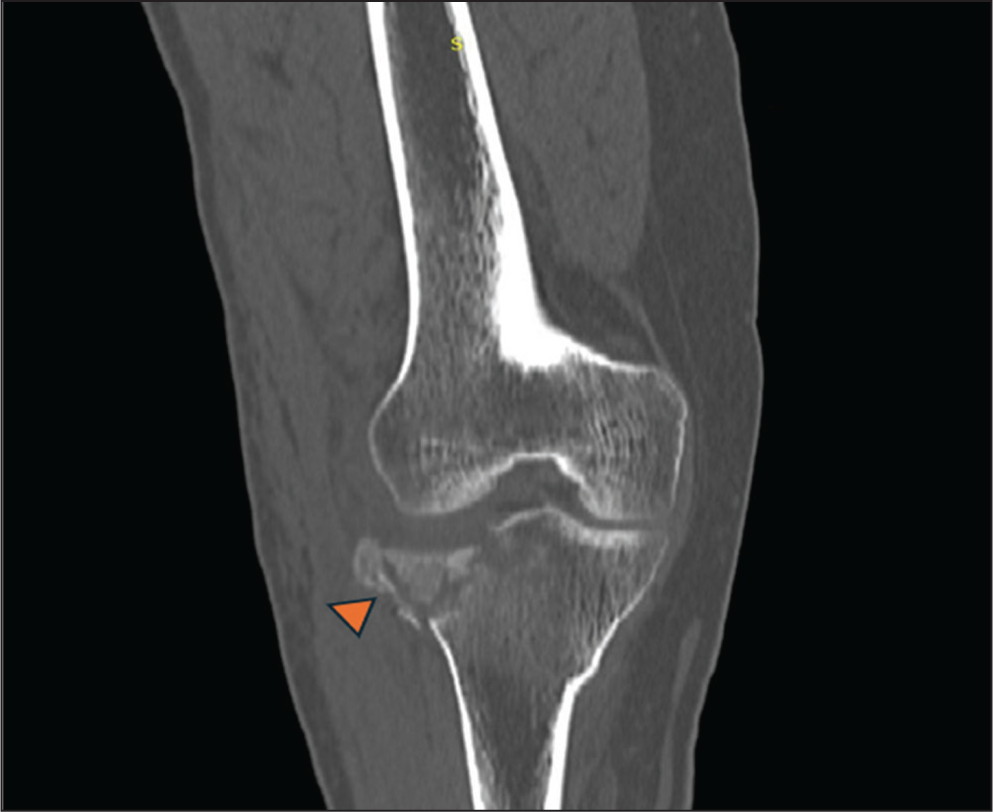
CT image of right knee showing a split depressed fracture () of lateral tibial plateau
Dual energy CT can be used to detect bone marrow oedema. Contrast-enhanced CT is useful in detecting vascular injuries like laceration, thrombosis, and pseudoaneurysms associated with skeletal trauma. This is useful in prompt and effective treatment planning.
In the post-treatment setting of trauma, CT may be used to check hardware-related complications like malpositioned screws and dislocation or deformity of the implant.
Limitations
It involves ionising radiation, which may be of significant concern in paediatric or pregnant patients. Routine CT has poor sensitivity to detect bone marrow oedema or contusion, which is often a primary contributor to pain. It has poor sensitivity in assessing soft tissue structures like ligaments, tendons, labrum, etc.
Tips for Radiation Dose Reduction
As CT has become indispensable in many cases of skeletal trauma, there has been an increasing emphasis on dose reduction. The following tips can be followed to limit the dose. The scan area should be limited to the area of concern. Low-dose protocols may be used in imaging of extremity trauma without much effect on image quality. In polytrauma cases, scanning multiple consecutive regions like neck, thorax, abdomen and pelvis in a single examination reduces radiation dose, as it eliminates the need for repeated scout images and image overlap.
MRI
MRI has revolutionised the imaging of the musculoskeletal system with its excellent soft tissue contrast, high spatial resolution, multiplanar capability and lack of ionising radiation.[14]
Applications
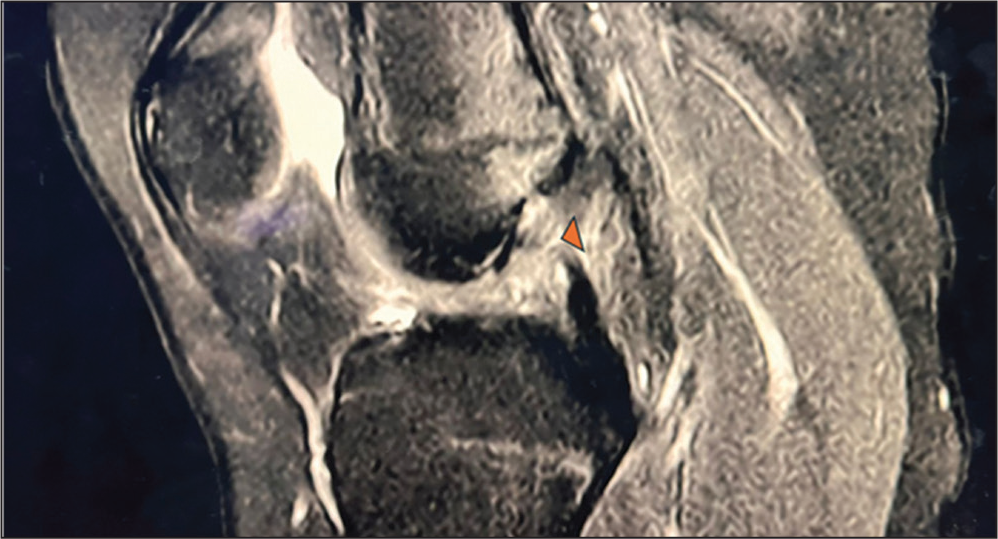
MRI is the investigation of choice in joint trauma, where there is suspicion of injury to soft tissue structures like ligaments, tendons, labrum or menisci. Most commonly evaluated joints due to trauma are knee, shoulder, and hip, followed by ankle. However, other joints like elbow and wrist can also be effectively evaluated by MRI. Muscle injuries can be accurately graded as strain, partial tear or complete tear using MRI [Figure 5].
Sagittal PDFS MRI image of the knee showing an anterior cruciate ligament tear ()
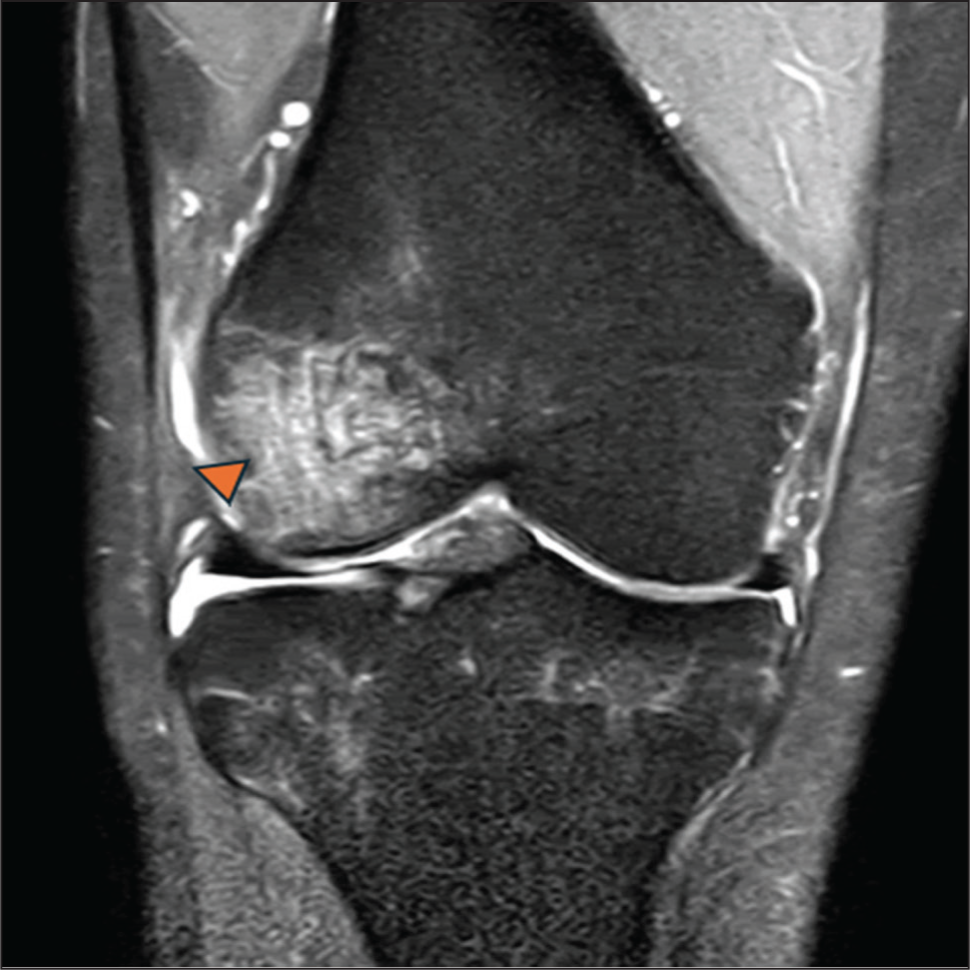
MRI is the modality of choice in depicting undisplaced avulsion fractures or fractures with unossified epiphyses by demonstrating bone marrow oedema at the avulsion site. MRI is an excellent modality for early depiction of stress fractures. Fluid-sensitive sequences are extremely useful to demonstrate osseous oedema, which is the earliest feature of a stress fracture [Figure 6]. MRI can also show other late features like cortical breach and adjacent soft tissue oedema. Radiographically occult fractures can be demonstrated on MRI as areas of bone marrow oedema, with a low signal intensity line on T1WI.
Coronal PDFS MRI image of right knee showing bone marrow oedema () involving lateral femoral condyle
MRI is the modality of choice in the detection of cartilage injury, which may result in debilitating joint degeneration if left untreated. It plays a major role in spinal trauma, where complications like spinal cord involvement need to be assessed.
Limitations
Long duration of examination due to multiple sequences may limit the use in an acute setting, particularly in haemodynamically unstable patients. High cost and low availability are the limitations in remote rural settings. It may not be suitable for patients with Claustrophobia. MRI is contraindicated in patients with cochlear implants, MR-incompatible pacemakers and implants.
Nuclear Scintigraphy
Nuclear scintigraphy uses the injection of a radionuclide and acquisition of images which show uptake of radiotracer by bone. Tc 99m-MDP (Methylene Diphosphonate) is the most commonly used radiotracer. The uptake is increased in areas of increased bone turnover and vascularity, which helps to detect fractures. SPECT and PET are the modalities used. Fusion imaging, where SPECT/PET is combined with CT, improves the anatomical localisation.[15]
Although the use of scintigraphy has been significantly replaced by MRI in trauma, it may be used in a few cases where MRI is contraindicated.
Applications
It is useful in detecting stress fractures before they become visible on a plain radiograph. It is also useful in detecting acute occult fractures like toddler’s fracture of tibia, fracture of scaphoid, by demonstrating areas of increased uptake. Occult insufficiency fractures in areas like the sacrum, femoral neck and pelvis can be detected. It can be used to differentiate between benign and malignant fractures.
It helps in assessing metabolism and blood flow at the injury site, which is useful in assessing fracture healing.
Limitations
It involves ionising radiation. It has high sensitivity in detecting stress or occult fractures, but low specificity.
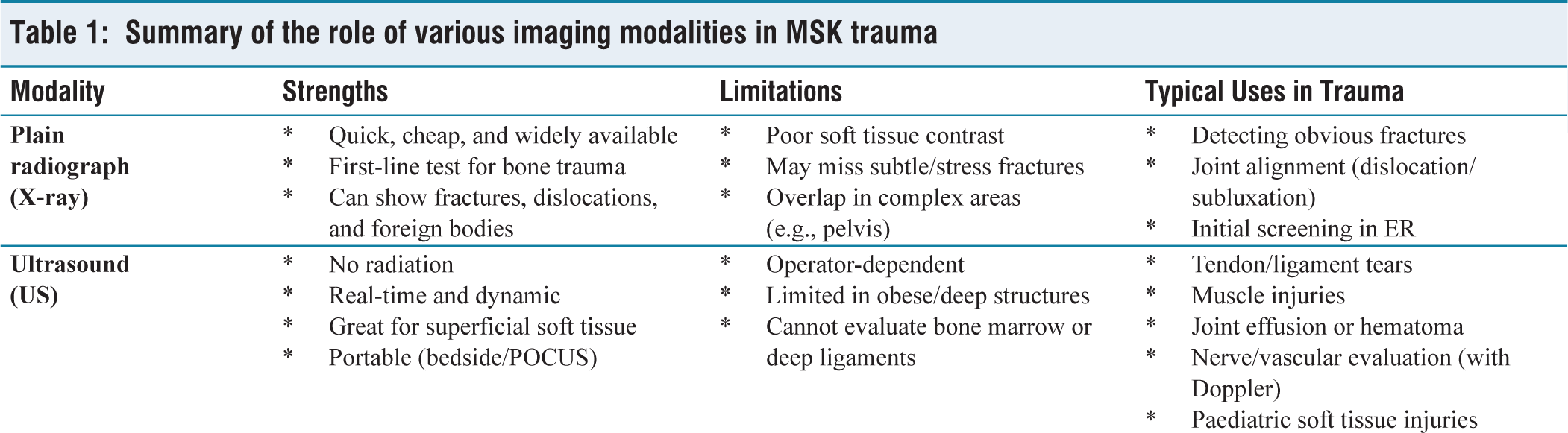
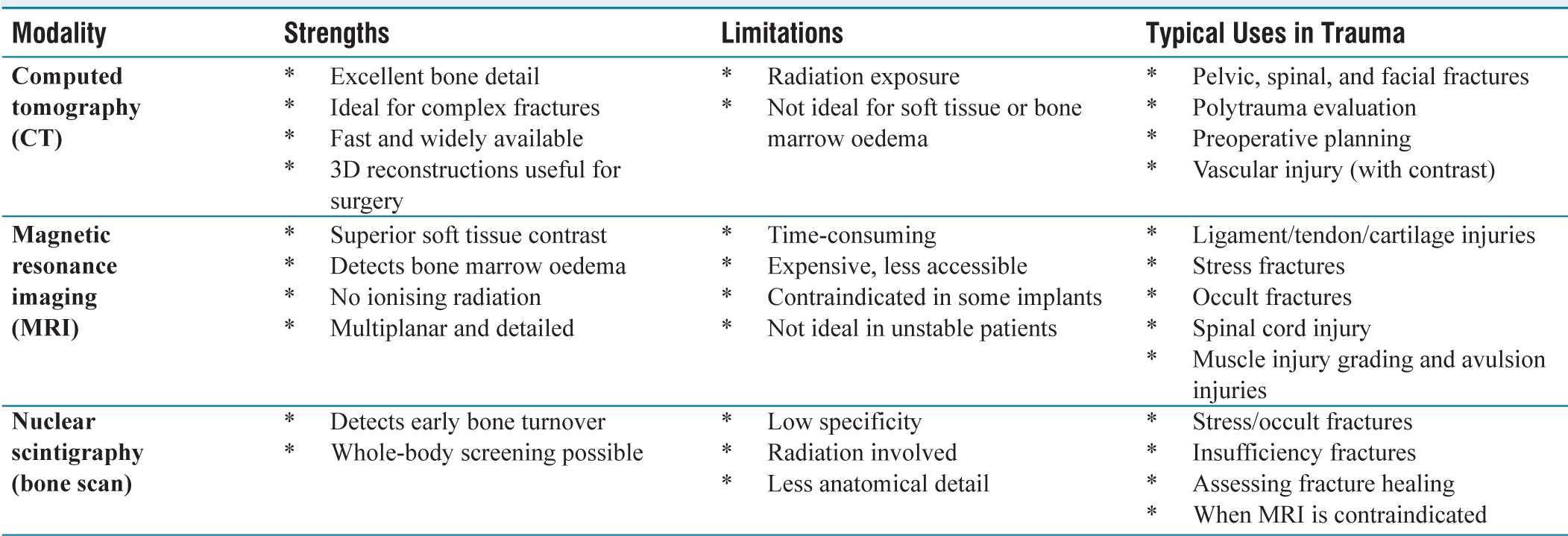
Summary
Summary of the role of various imaging modalities in MSK trauma
Conclusion
The use of imaging modalities should be guided by the mechanism of trauma, site of trauma, anatomical structure suspected to be involved and other factors like age of patient.
While plain radiographs are most often sufficient in detecting extremity fractures, CT may be required to detect occult fractures, to evaluate fractures of complex anatomical structures and in pre-surgical planning. The US has become a promising imaging modality in the assessment of superficial soft tissue injuries due to its superior resolution. MRI is an excellent and gold standard imaging modality in trauma of soft tissues, intra-articular structures and spine.
Awareness of advantages, specific applications of various imaging modalities in various scenarios and their limitations is important in daily practice.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Not applicable.
Informed consent
Nil.
Credit author statement
Madhavi Chamarthi: Study design, Manuscript drafting, Image analysis.
K.J.S.S. Raghu Teja: Study design, Image analysis.
Anil Kumar Kallepalli: Image analysis, Manuscript drafting.
Rajesh Allu: Manuscript drafting.
Sonica Sharma: Image analysis.
Data availability
Nil.
Use of artificial intelligence
Nil.