
Abstract
Purpose:
Reducing unnecessary testing may benefit patients, as some computed tomography (CT) and magnetic resonance imaging (MRI) expose patients to contrast, and all CTs expose patients to radiation. This observational study with historical controls assessed shifts in CT and MRI utilization over a 9-year period after a private health insurer’s implementation of a nondenial, consultative prior authorization program.
Methods/Materials:
Normalized rates of exams per 1000 person-years were plotted over 2005 to 2014 for people with commercial and Medicare Advantage health plans in the San Antonio market, with 2005 utilization set as the baseline. The program was implemented at the start of 2006. Computed tomography and MRI utilization changes were compared with contemporaneous changes in low-tech plain film and ultrasound utilization.
Results:
Growth in high-tech imaging utilization decelerated or reversed during the period. In 2006, CT utilization dropped to between 76% and 90% of what it had been in 2005, depending on the plan. In 2014, it was between 52% and 88% of its initial level. MRI utilization declined to between 86% and 94% of its initial level in 2006, and then to between 50% and 75% in 2014. Ultrasound utilization was greater in 2014 than in 2005 for some plans. Plain film utilization declined between 2005 and 2014 for all plans.
Conclusion:
There was an immediate and sustained decline in CT and MRI utilization after the introduction of the program. While many factors may have impacted the long-term trends, the mixed trends in low-tech imaging suggest that a decline in low-tech imaging was not responsible for the decline in CT and MRI utilization.
Keywords
Introduction
Diagnostic imaging plays a vital role in care, yet it exposes patients to harm that may not always outweigh the benefits. In cases where the imaging machine utilizes intense ionizing radiation, as happens with computed tomography (CT), patients face a greater increased risk of cancer than when imaging is performed with plain film radiographs. 1,2 Even when no radiation is involved, as is the case with magnetic resonance imaging (MRI), patients experience potential risks. The contrast agents used when performing CTs and MRIs have infrequent but serious side effects, including contrast-induced nephropathy and nephrogenic systemic fibrosis. 3 In rare instances, MRI scanning procedures have caused patients to experience burns, implant malfunctions, and harm from objects attracted to the magnetic field. Between 1995 and 2005, 389 people were reported to have been injured, and 9 people were reported to have been killed by MRI exams. 4 Furthermore, researchers are examining whether the magnetic field itself can cause harm. 5
Despite the potential risks entailed, inappropriate imaging utilization has occurred as a part of defensive medicine. One survey found that 93% of physicians in high-risk specialties reported practicing defensive medicine, with 43% of those reporting that their most recent defensive act was using clinical imaging. 6 A prospective audit of imaging decisions among orthopedists found that 41% of CT orders and 39% of MRI orders were made for defensive reasons. 7 Furthermore, patient-initiated requests have the potential to drive imaging utilization of little clinical value. 8
The issue of inappropriate utilization of medical imaging has been combatted by stakeholders ranging from the American College of Radiology’s select imaging appropriateness initiative to the health care commentator Atul Gawande, who has brought attention to low-value and no-value testing. 9 Beginning in the mid-1990s, a number of radiology benefits management firms were launched to reduce inappropriate utilization through prior authorization. 10 Prior authorization programs have the potential to reduce clinically unnecessary imaging by discouraging imaging that is not indicated.
The national health insurer examined by this study experienced annual utilization growth of approximately 10% for CT and MRI until the introduction of a nondenial prior authorization program. The previously published findings on the program only examine its first 3 years of performance and do not examine contemporaneous changes in low-tech imaging. 11 Thus, the program’s long-term impact and the relationship between high-tech and low-tech imaging trends have not been explored.
While research has identified trends in CT 11 -19 and MRI utilization, 11,12,15,16,18 -21 these studies have primarily examined data from traditional Medicare or commercial insurance. Although the literature has shown that imaging utilization began declining after 2008, little has been reported on the trend after 2012, in part due to the lags associated with public data reporting on outcomes experienced by people with traditional Medicare insurance. Furthermore, there has been limited research on change in utilization following the implementation of a nondenial prior authorization program. 12 This study extends the literature by reporting on utilization trends experienced by people with commercial insurance and Medicare Advantage insurance between 2005 and 2014, after the implementation of a nondenial prior authorization program on January 1, 2006.
Methods
Study Design and Data Sources
This retrospective longitudinal study assessed changes in CT and MRI utilization 1 year and 9 years after the introduction of a nondenial prior authorization program by [Humana Inc.], a health care company providing medical and pharmacy benefit plans nationally. As the program was launched in different regions at different times, only data from the San Antonio, Texas, market was considered in this analysis. Changes in low-tech imaging (plain film X-ray and ultrasound) were additionally assessed as a contemporaneous comparator. Administrative claims data from commercial and Medicare Advantage health plans were used to conduct this research. As this study was conducted as part of ongoing quality improvement efforts, it did not meet the definition of research requiring institutional review board review under the U.S. Department of Health and Human Services 45 CFR 46:102. Patient data were managed securely, in accordance with the Health Insurance Portability and Accountability Act.
Prior Authorization Program
On January 1, 2006, the insurer launched a nondenial prior authorization program run by [HealthHelp] in the region examined by the study. The prior authorization program relies upon clinical evidence and guidelines from multiple professional societies to determine which practices are considered to be consistent with high-quality care. Providers inform the prior authorization program of their imaging orders in order to obtain authorization. When provider orders appear to be less than optimal, the prior authorization program outreaches to ordering providers to arrange peer-to-peer conversations with practicing radiologists contracted by the prior authorization program. The prior authorization program operates on a nondenial model in which providers may proceed with their initially requested orders, even if prior authorization program–contracted radiologists do not agree. Thus, conversations are intended to be educational rather than adversarial. Ordering physicians receive an e-mail at the end of the conversation, memorializing the decisions that were made. This e-mail can serve as proof that the consult physician believed that a particular course of action was consistent with the standard of care.
Sample Selection
Data were collected from administrative claims made between January 1, 2005, and December 31, 2014. People included in the sample had fully insured commercial or Medicare Advantage health plans. People with individual (nongroup) commercial health plans were not included. The health plans had both health maintenance organization (HMO) and preferred provider organization (PPO) designs.
As people may participate in a health plan for under a year for a number of reasons (eg, change of job, relocation, or other life events), the size of the sample has been reported in person-years. One person-year represents 12 months of health plan membership by 1 person. A total of 1 538 917 person-years of data were included in the study. All people belonging to the health plans being examined, in the geography and time period specified, were included in the study. Table 1 lists the number of person-years in each year included in the study, by health plan type. The table additionally features the percentage of person-years attributed to people aged 65 years or older in each of the plans during each of the years. Undercounting utilization due to dual enrollment in a commercial health plan and traditional Medicare does not bias the findings, as when people are dually enrolled, the commercial health plan pays the imaging claims.
Population.

Abbreviations: HMO, health maintenance organization; PPO, preferred provider organization.
Outcomes and Analyses
The analysis only included orders for CT, MRI, plain film X-ray, and ultrasound. While CT and MRI orders were reviewed by the prior authorization program, plain film X-ray and ultrasound orders were not. The claims data set was used to calculate the annual number of imaging exams performed per 1000 person-years. Imaging exams were counted using the prior authorization program’s records. In order to understand how utilization shifted over time, imaging exams performed per 1000 person-years were trended over time. Utilization was examined separately for CT and MRI and for each commercial and Medicare Advantage plan. The utilization measures included exams performed across all sites of care. Spearman’s rank correlation coefficient was calculated to assess whether each of the trends was monotonic and if the correlation between time and utilization was negative.
Rates of change in utilization for each plan were indexed relative to the rate of utilization in 2005, the value of which was set at 100. Values after 2005 were computed annually to reduce the impact of seasonal variation and were expressed as a percentage of the 2005 utilization value.
Results
High-Tech Imaging Trends
As is shown in Figures 1 and 2, CT and MRI utilization underwent both immediate and sustained decreases. In 2006, 1 year after the nondenial prior authorization program was launched, CT utilization per 1000 person-years was between 76% and 90% of its initial level, depending on the health plan type examined. Magnetic resonance imaging utilization immediately declined as well, with 2006 utilization ranging between 86% and 94% of its 2005 level, depending on the health plan type.

Computed tomography (CT) utilization: normalized, annual rate per 1000 person-years.

Magnetic resonance imaging (MRI) utilization: normalized, annual rate per 1000 person-years.
The decreases in CT and MRI utilization were sustained in 9 years following the launch of the nondenial prior authorization program. In 2014, CT utilization rates were between 52% and 88% of their 2005 levels, whereas MRI utilization rates were between 50% and 75% of their 2005 levels. All of the health plans had lower rates of CT utilization in 2014 than in 2006, with the exception of the Medicare PPO. The Medicare PPO had CT utilization at 76% of its 2005 level in 2006 and then increased CT utilization to 88% of its 2005 level in 2014. Magnetic resonance imaging utilization rates were lower for all health plans in 2014 than they were in 2006.
Spearman’s rank correlation coefficients were significant (P < .05) and negative for all trend lines except for those for Medicare PPO CT utilization (P = .99; ρ = .0061) and Medicare HMO MRI utilization (P = .13; ρ = −.52). The lack of a significant, monotonic negative trend in Medicare PPO CT utilization is consistent with the dip, and then increase in utilization is shown in Figure 1. Spearman’s ρ for the Medicare HMO MRI utilization trend suggests a declining, albeit insignificantly monotonic trend.
Low-Tech Imaging Trends
Contemporaneously with these changes in high-tech imaging, there were mixed trends in low-tech imaging. Figure 3 shows that 2006 and 2014 plain film utilization rates per 1000 person-years were below their 2005 level for all health plans. However, as is shown in Figure 4, ultrasound utilization did not exhibit a consistent pattern. In 2006, rates of ultrasound utilization were between 67% and 95% of their 2005 levels, depending on the health plan. By 2014, Medicare HMO ultrasound utilization rates were 125% of their 2005 level, and commercial PPO ultrasound utilization rates were 117% of their 2005 level. However, Medicare PPO ultrasound utilization rates and commercial HMO ultrasound utilization rates were below their respective 2005 levels.

Plain film utilization: normalized, annual rate per 1000 person-years.
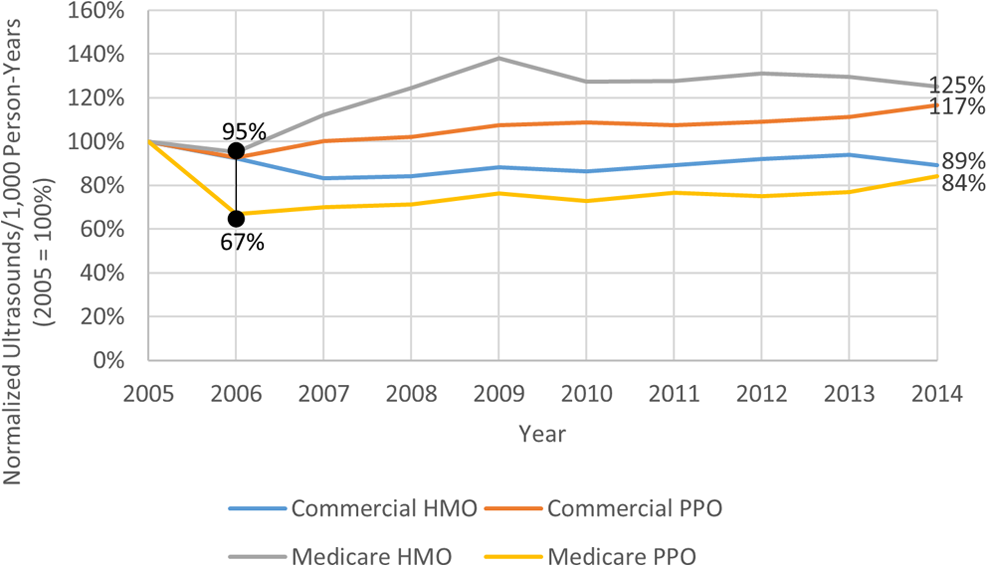
Ultrasound utilization: normalized, annual rate per 1000 person-years.
Statistical tests found a mixture of monotonically positive, monotonically negative, and nonmonotonic trends in low-tech imaging. Spearman’s rank correlation coefficients were significant and positive for the commercial PPO ultrasound and Medicare HMO ultrasound utilization trends. This suggests that there was a monotonic increase in ultrasound utilization in these populations. Meanwhile, it was significant and negative for commercial HMO plain film and commercial PPO plain film utilization. The coefficient was not significant for Medicare HMO plain film utilization (P = .56; ρ = −.21), Medicare PPO plain film utilization (P = .56; ρ = .21), commercial HMO ultrasound utilization (P = .88; ρ = .055), and Medicare PPO ultrasound utilization (P = .26; ρ = .39).
Discussion
The results of this study show that over the past decade, progress has been made toward reducing imaging utilization. The deceleration of growth occurred concurrently with the adoption of a nondenial approach to prior authorization—an approach with the potential to increase utilization. The insurer’s compound annual growth rate for CT and MRI utilization nationally before the introduction of the program was approximately 10%. 11 All of the health plans examined had less CT and MRI utilization after 9 years than they did in the initial year, indicating that the growth ceased during the period of the study. A test for monotonicity found that all high-tech imaging trends were negative and statistically significant, except for the trends for Medicare PPO CT and Medicare HMO MRI utilization, which were not significant. In both cases, the trends were not monotonic, as utilization rates were below 2005 levels in 2006 and 2014 but were above 2006 levels from 2007 to 2012.
The trend in CT and MRI utilization compares favorably to findings from the traditional Medicare population. The national traditional Medicare population had CT utilization in 2006 which was 106% of its 2005 level. 22 Likewise, traditional Medicare MRI utilization in 2006 was 105% of its 2005 level. 23 Upward trends in CT and MRI utilization also occurred between 2005 and 2006 in Texas.
There are multiple factors which may be driving the decline of utilization growth. Low-tech imaging exams can instigate high-tech imaging utilization, as the findings of low-tech exams may require follow-up high-tech exams. The concurrent decline in low-tech imaging utilization among some of the health plans examined may be one explanation for the drop in high-tech imaging. Furthermore, while traditional Medicare CT and MRI utilization (which is not subject to a nondenial prior authorization program) grew between 2005 and 2006, it contracted in subsequent years. 21,22 After the passage of the Affordable Care Act in 2010, the gradual implementation of value-based payments may have placed downward pressure on utilization. Nonetheless, the migration to value-based payments was not substantially underway when the program was first implemented in 2006. Nationally, physician participation in accountable care organizations grew from 3% in 2011 to 30% in 2014. 24
The utilization trends observed may have been additionally impacted by a learning or sentinel effect, which has been described previously in the prior authorization program and radiology benefits management literature. 11,25 The prior authorization program operates under an educative model by which academic radiologists consult with ordering physicians on appropriateness of certain health care services. If there is a sentinel effect or a learning effect, a prior authorization program may impact utilization both directly through the recommendation of fewer exams and indirectly by making physicians aware that their performance is being monitored.
Limitations
This study has several limitations. First, data from only one payer in a single region were analyzed. While there may have been some region-specific factors that influenced findings, a deceleration in CT and MRI utilization was also found in a national analysis of the program, suggesting that the results may be nationally generalizable for the payer. 26 However, the payer’s utilization patterns may not be typical of those experienced by other payers. Secondly, trends may have been impacted by a combination of factors, including the introduction of the prior authorization program, changes in reimbursement, the shift toward value-based payment, and increased industry awareness of the harms of irradiation. Because physicians treating Medicare Advantage patients likely treat traditional Medicare patients as well, changes in the traditional Medicare payment structure may impact ordering behavior. Although CT and MRI were relatively mature technologies during the time examined, there were some changes in the standard of care during the study time frame. Furthermore, there were changes in the prior authorization program itself, which was periodically modified in response to the development of new evidence and guidelines. While statements cannot be made about the precise causes of the trends observed, the trends do reflect changes in patient care experiences. Nonetheless, another study of an implementation of the program in 2011 by a state Medicaid program also showed a sharp drop in CT and MRI utilization following implementation. 27 Given that the Medicaid findings occurred in another state and in another time frame, it provides some support to the generalizability of the findings.
Conclusion
The findings of this study showed that after the adoption of a nondenial, educational approach to prior authorization within a large provider of commercial and Medicare Advantage health insurance coverage, CT and MRI utilization per 1000 person-years declined the following year and remained lower 9 years later. These results provide a unique view into the imaging trends applicable to individuals covered by the commercial and Medicare Advantage plans examined through 2014, since these data are not publicly available.
The authors conducted this study as a part of their normal job responsibilities at HealthHelp and Humana. AP reports employment by Payer+Provider Syndicate and the reimbursement of travel expenses by the American College of Radiology. DL reports board membership at Outpatient Imaging Affiliates.
Footnotes
Acknowledgment
The authors would like to acknowledge Laura E. Happe, PharmD, MPH, Stephen E. Price, DPT, MBA, and Teresa L. Rogstad, MPH for their contributions to the manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AP, DL, EK, and AG conducted this research as a part of their job responsibilities for HealthHelp. RB and JL conducted this research as a part of their job responsibilities for Humana. HealthHelp and Humana were involved in the collection of data, its analysis and interpretation, and determining whether to publish the finished manuscript. JL additionally reports Humana stock. AG additionally reports HealthHelp stock.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.