
Abstract
Background:
Timely, accurate diagnosis can enable early inception of treatment, and thereby, potentially improve the overall outcome in patients with orthopaedic pathologies. To achieve this, mutual communication and direct consultations between radiologists and orthopaedist are essential. The current scoping review comprehensively assesses the expectations of an orthopaedic surgeon about radiologists and their interpretations of different imaging studies.
Methods:
A comprehensive search of the literature was performed on three different databases (Google search, PubMed, and Embase) on 19 June 2025, using specific keywords. The manuscripts, which pertained to the topic of interest, were considered.
Results:
An effective communication strategy between the radiologist and orthopaedic surgeon is critical in order to optimise patient care. The completeness and clarity of information provided by a clinician to the radiologist are essential to ensure appropriate choice of imaging sequences by the radiologists and excellent reporting. The radiologists need to develop specific knowledge and understanding of different orthopaedic pathologies (orthopaedic trauma, sports injuries or ligament/ tendon tears, infections or tumours, spinal pathologies, paediatric orthopaedic scenarios and postoperative complications) in order to provide management-driven reports, which may be of greatest interest to the treating surgeon.
Conclusions:
The radiologists must be appropriately educated by the clinician regarding the specific reasons underlying the diagnostic demands. Mutual consideration of the patients’ functional status and direct communications between orthopaedic surgeons and radiologists (in the appropriate situations) can substantially improve the treatment strategy and ameliorate the overall outcome in a majority of patients.
Introduction
Over the past decade, substantial strides have been made in the fields of orthopaedics and radiology alike, which have tremendously improved the overall quality of health care delivery.[1,2] With the technological advancements in recent years, the goals have shifted from graduated, slow recuperation strategies to rapid and focused recovery programmes after surgical interventions.[3] The enhanced recovery approaches are always reliant upon the cooperative efforts on the part of multidisciplinary teams.[4] In this context, the importance of accurate interpretation of the imaging studies, precise identification of the problems classification of the pathology in devising the correct treatment strategies for patients cannot be understated.
With the recent explosion in the use of labelled data (i.e., the ‘big data’), the era of artificial intelligence (AI)-based innovations has emerged. ‘Deep learning’ is a machine learning technology utilising an algorithmic neural network (such as a convoluted neural network [CNN]), and has tremendous potential to perform equally well or even better than humans in image interpretation and classification.[1,2,4–8] Nevertheless, in the current situation, the AI technology is still far from completely replacing the coordinated efforts between the radiologists and treating physicians in achieving the diagnosis for pathologies on a routine basis.
For a coordinated diagnostic approach, the radiologist must be well aware not only of the criteria to diagnose or identify a particular condition, but also the nuances and philosophies underlying the diverse treatment approaches, indications for different interventions, assessment of the severity of the condition, as well as the evaluation of healing or recovery of the patient following the particular intervention.[2,9–17] Timely, accurate diagnosis can enable the early inception of treatment, as well as substantially enhance the possibilities of an excellent outcome through minimally invasive surgeries. The current narrative review was thus planned to comprehensively evaluate the available literature, and address the questions vide-infra: (a) what are the ways by which an orthopaedic surgeon and a radiologist can establish mutual communication and direct consultation, such that the best strategy for the patients’ treatment can be planned? (b) How can the orthopaedic surgeon provide the radiologist with sufficient information in order to help him choose the best imaging modality? and (c) what are the necessary details and information, which the radiologist needs to be educated on (with regard to different orthopaedic pathologies), in order to generate reports which enable the surgeon to plan the optimal management?
Methods
Literature Search
A comprehensive search of the literature was performed on three different databases (Google search, PubMed, and Embase) on 19 June 2025. The manuscripts, which pertained to the topic of interest (i.e., what an orthopaedic surgeon expects from the radiologist), were considered. The keywords employed in the search using Boolean operators included: (((orthopaedic surgeon) OR (orthopaedist) AND (radiologist) OR (imaging) OR (MRI report) AND (information) OR (expectation) OR (clinical relevance))).
Inclusion/Exclusion Criteria
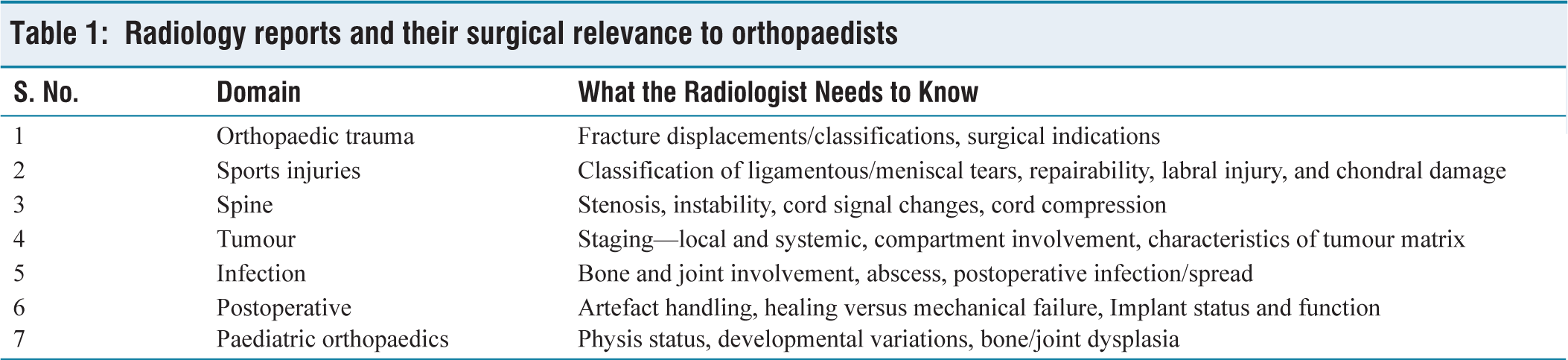
All the manuscripts that discussed the general expectations from an orthopaedic surgeon’s point of view with regard to the interpretation (or reporting) of an imaging study by a radiologist were considered for the study. Studies without the availability of complete manuscripts (abstracts, letters, opinions, or editorials) and manuscripts not pertaining to the relevant topic were excluded from the review [Table 1].
Radiology reports and their surgical relevance to orthopaedists
Article Selection and Data Extraction
The outputs from the search were extracted onto En-note, and then relevant articles were first selected manually after eliminating duplicates and non-relevant recommendations. The titles and abstracts were initially screened for the relevant manuscripts (Stage 1 screening); following this, complete manuscripts were appropriately scrutinised (Stage 2 screening). The most relevant manuscripts, on the basis of the aforementioned criteria, were finally selected to answer the specified questions.
Research Objective
The major research objectives of the current review include:
RO1: What is the best strategy to establish mutual communication between an orthopaedic surgeon and a radiologist in order to effectively plan a patient’s treatment? RO2: What are the details the orthopaedic surgeon needs to furnish to the radiologist in order to help him choose the best imaging modality for a patient? RO3: What is the level of knowledge a radiologist needs to gain, so as to generate the optimal reports on orthopaedic pathologies?
Results and Discussion
Outcome of Literature Search
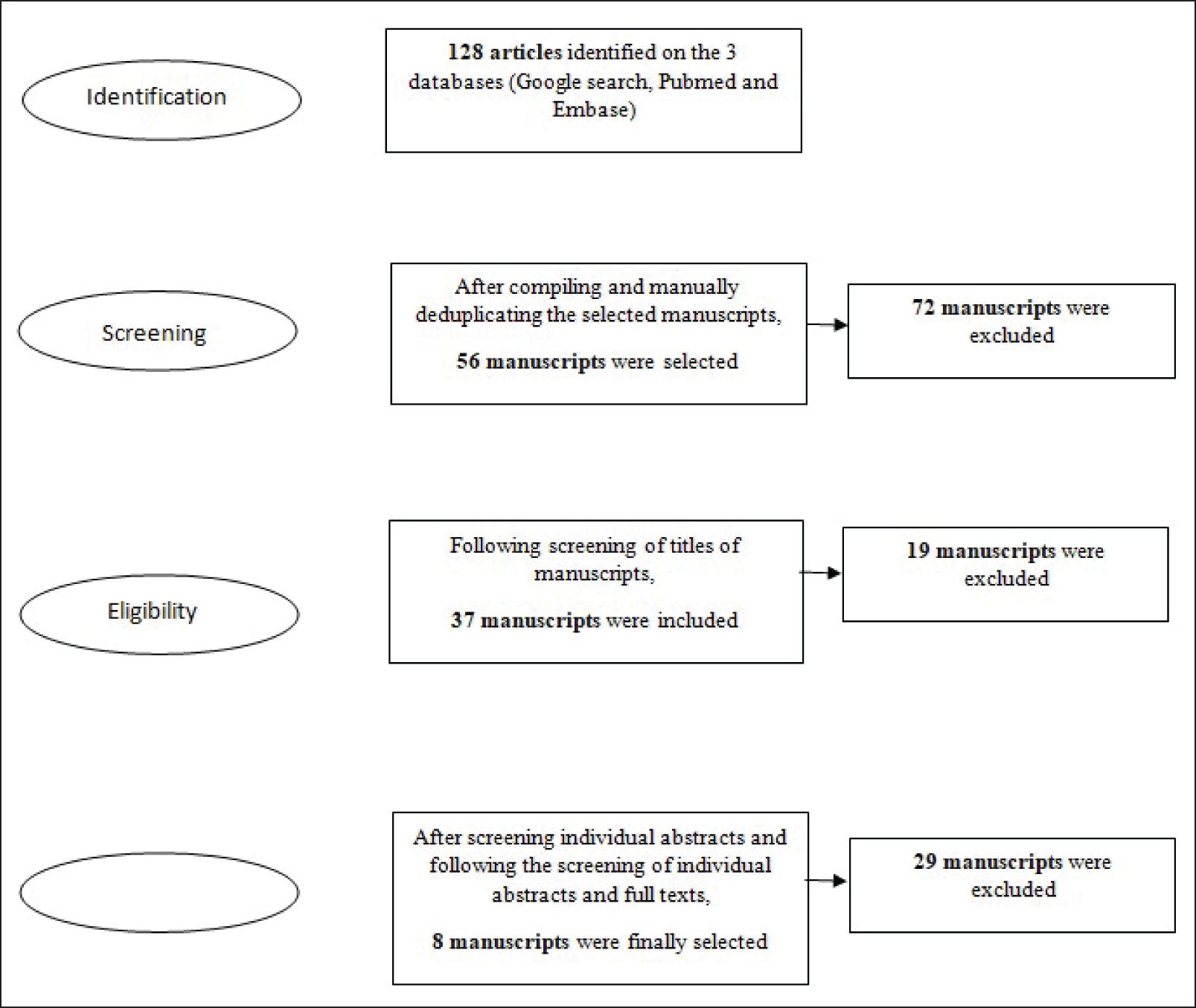
The initial literature search yielded 128 manuscripts. After elimination of duplicate manuscripts and two rounds of detailed screening, eight manuscripts were finally selected for the scoping review [Figure 1].
Seach strategy for the review
RO1: An effective communication strategy between the radiologist and orthopaedic surgeon is critical in order to effectively optimise patient care.[9–17]
Some of the realistic strategies to establish such effective communication include (a) regular multidisciplinary meetings (wherein interdisciplinary discussions involving musculoskeletal radiologists and surgeons can enhance decision-making and surgical planning, especially in challenging situations like complex trauma and oncology),[18] (b) direct one-on-one consultations to clarify in situations of diagnostic dilemma or communication of critical findings like spinal cord compression (including hospital-approved chat platforms or apps like EPIC Secure Chat), (c) shared PACS workstations (where orthopaedic and radiology attendings can co-review the imaging studies), (d) structured requisition forms with focused clinical questions, (e) collaborative software/electronic medical records (EMR), where flags and comments sections can enable bidirectional accountability,[19] (f) collaborative reviews involving quality improvement projects and joint audits, (g) cross-disciplinary teaching (or CME session), (h) feedback loops and surgical correlations (regarding intraoperative findings), (i) integrated reporting pathways (e.g., situations like tumour boards or trauma conferences, where consensus statements and reports are co-signed by orthopaedists and radiologists).[20]
RO2: It is well-acknowledged that the completeness and clarity of information provided by a clinician to the radiologist is essential to ensure appropriate choice of imaging sequences by the radiologists and excellent reporting.[21] The systematic approach to ascertain the transfer of such clear information to the radiologists includes the following steps[22]: provision of focused and detailed clinical history (including evolution of symptoms, details of prior medical history and clinical suspicion), the actual question or diagnosis which the clinician is trying to rule in or rule out (say, whether the ACL graft is intact, or whether the intervertebral fusion is complete), clinical urgency in the management of the patient (such an information can enable the radiologist to decide upon whether the patient needs an MRI/CT scan whether or not a contrast study is necessary, etc.), presence of any metallic implants or its compatibility with imaging, sharing prior imaging details or operative notes; and use of standard or templated imaging referral forms. In addition, whenever clinically appropriate, it is also appropriate on part of the orthopaedic surgeon to call and directly discuss the specific cases, such as atypical scenarios, postoperative complications, complex prior medical history and major diagnostic dilemmas.
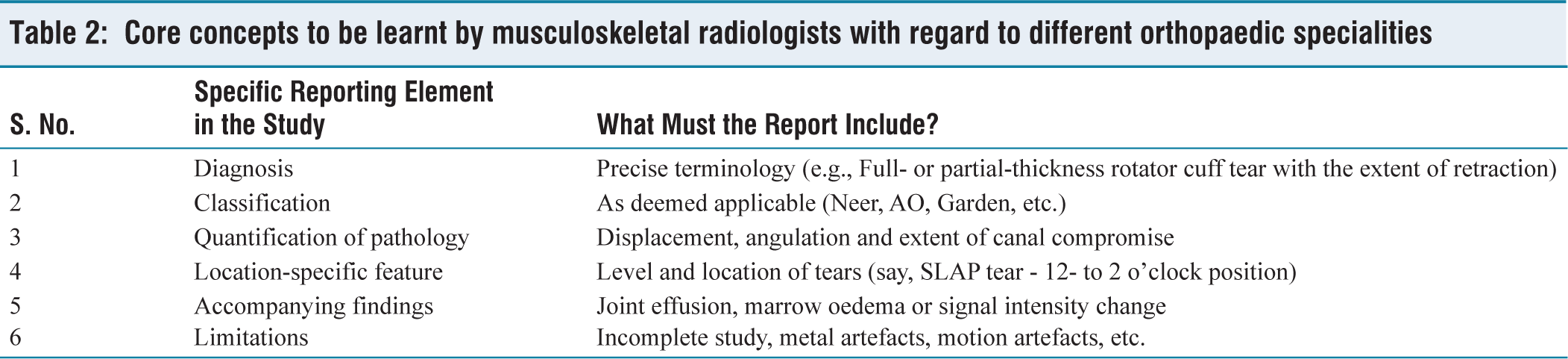
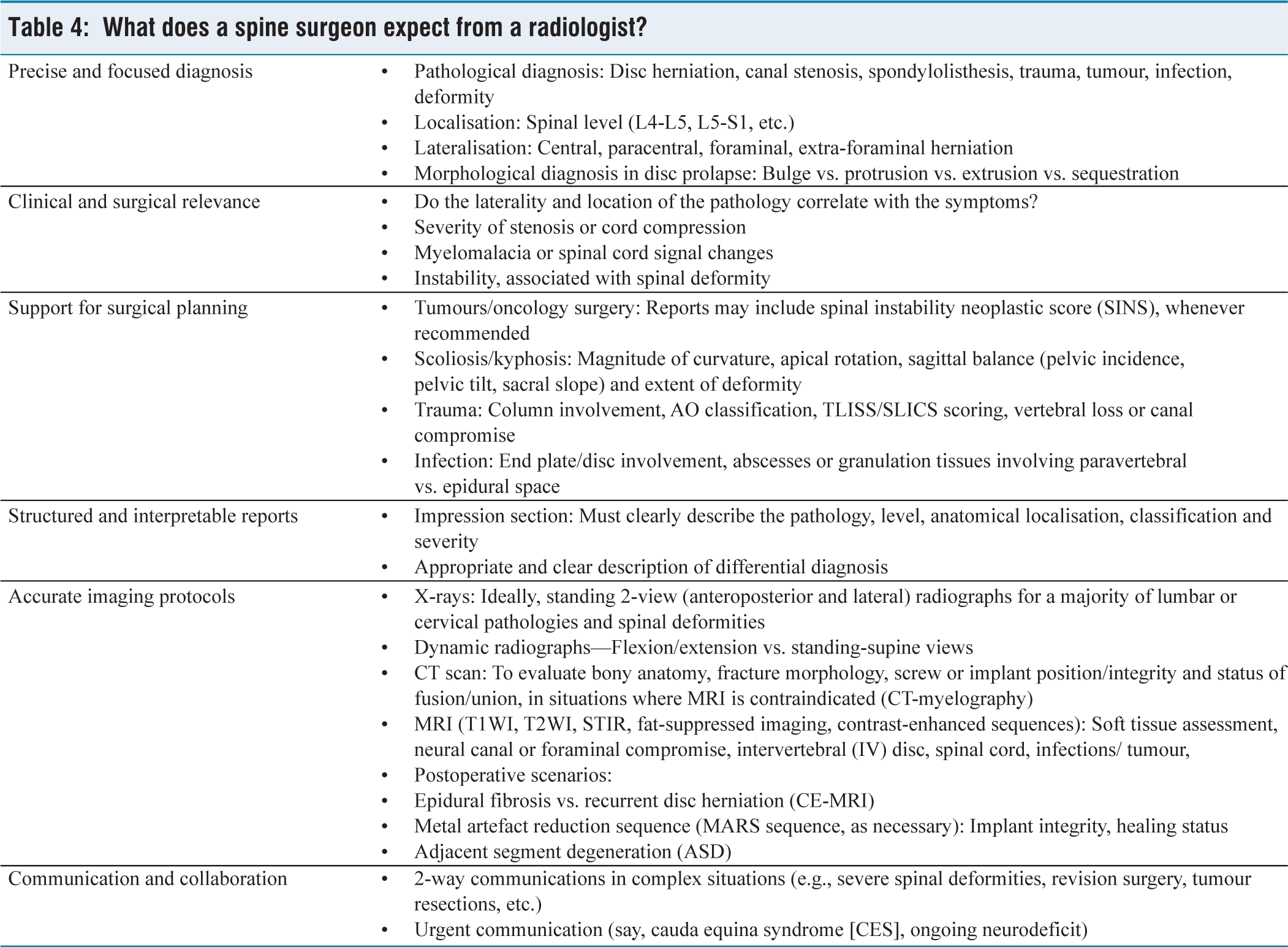
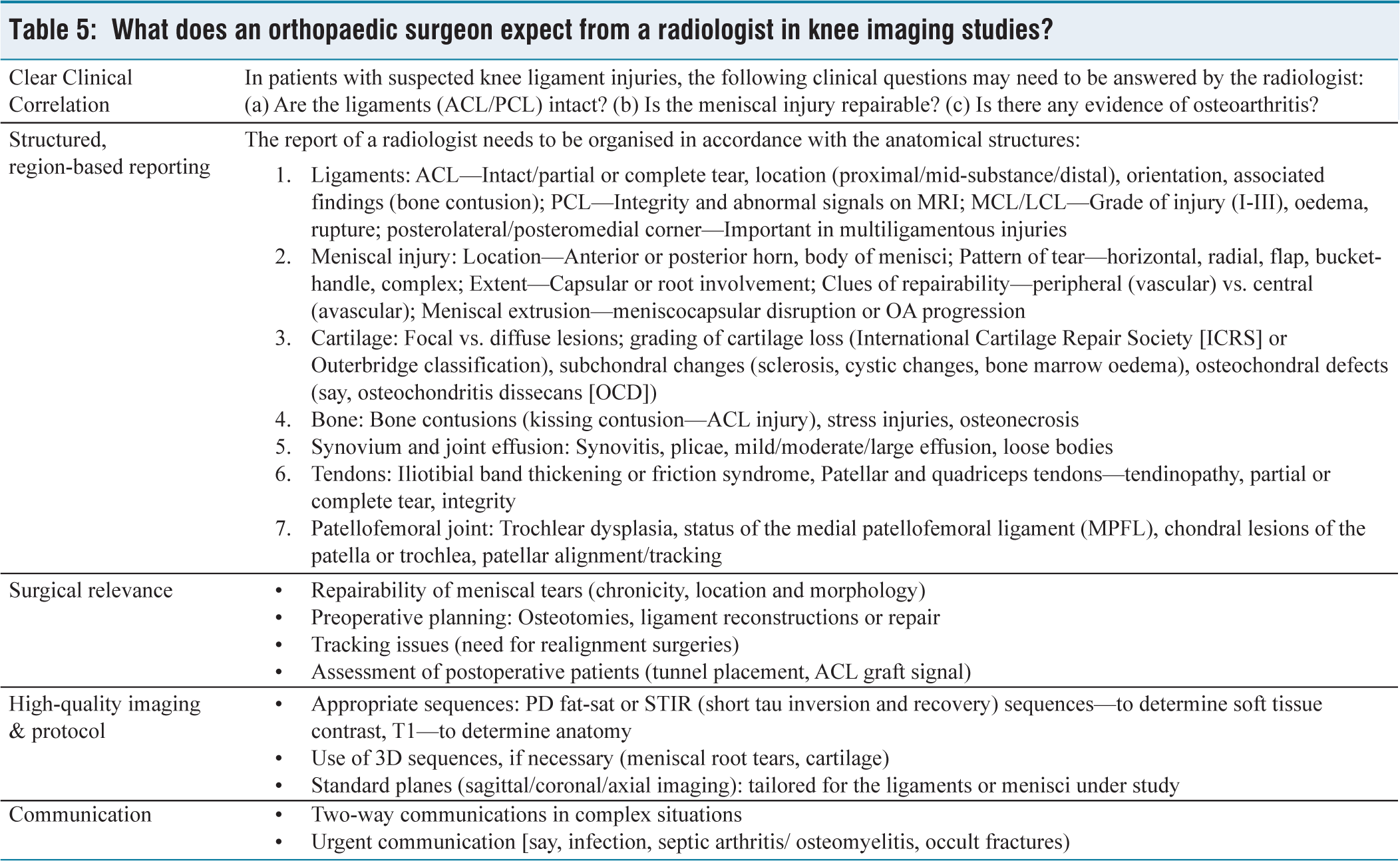
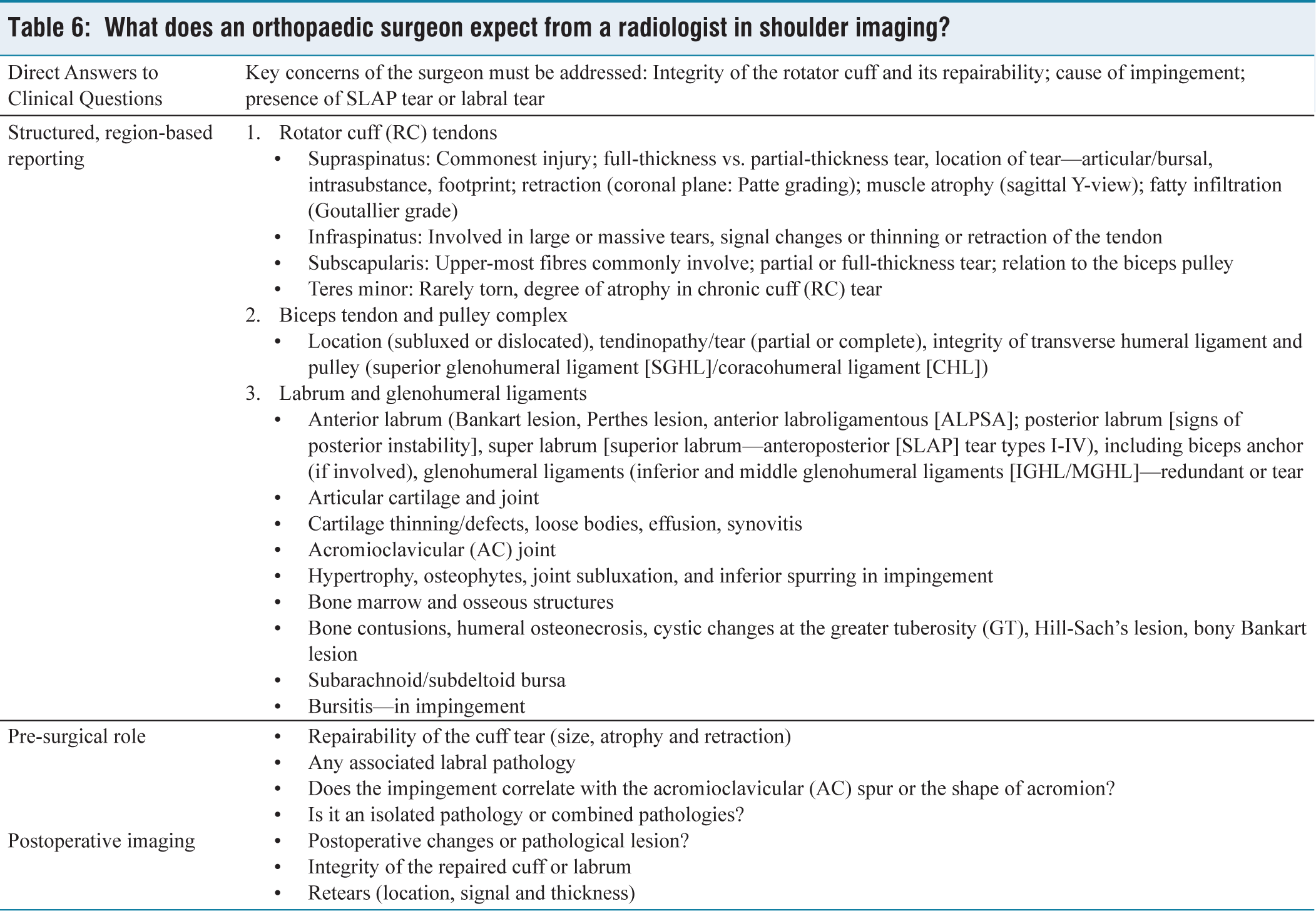
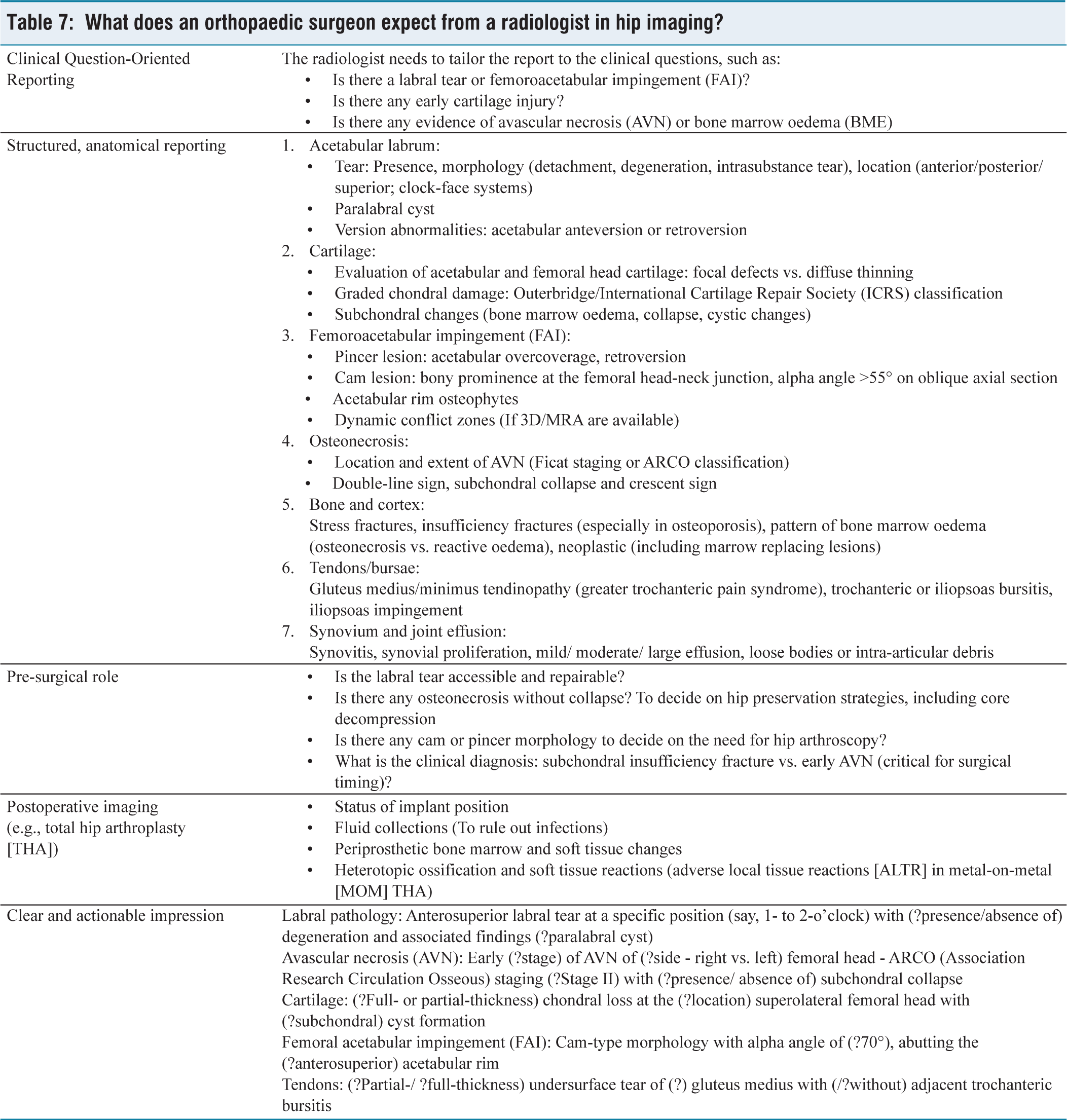
RO3: The radiologists need to develop specific knowledge and understanding of different orthopaedic pathologies in order to provide management-driven reports, which may be of greatest interest to the treating surgeon [Tables 2–8].
Core concepts to be learnt by musculoskeletal radiologists with regard to different orthopaedic specialities
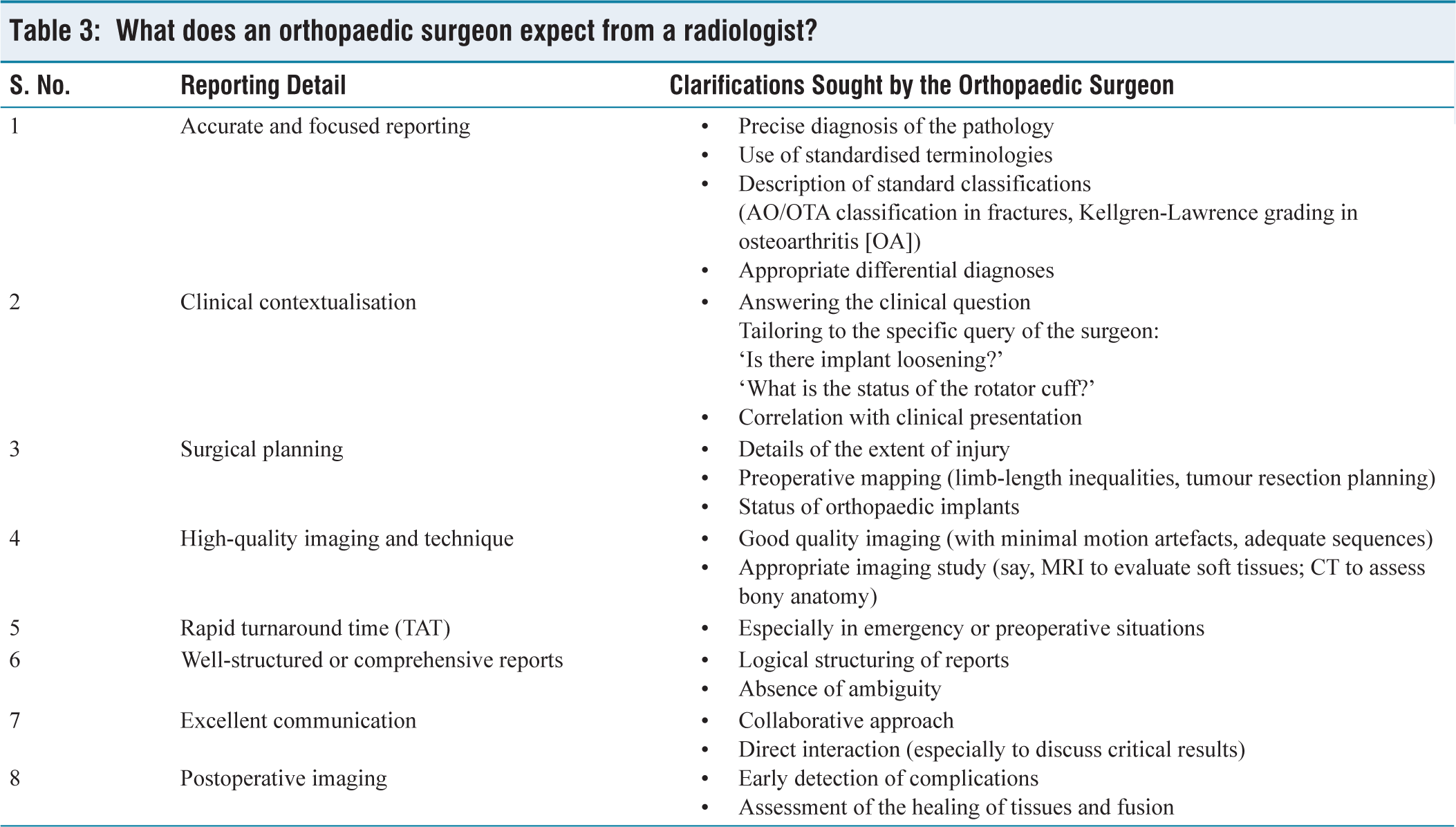
What does an orthopaedic surgeon expect from a radiologist?
What does a spine surgeon expect from a radiologist?
What does an orthopaedic surgeon expect from a radiologist in knee imaging studies?
What does an orthopaedic surgeon expect from a radiologist in shoulder imaging?
What does an orthopaedic surgeon expect from a radiologist in hip imaging?
What does an orthopaedic surgeon expect from a radiologist in orthopaedic trauma situations?
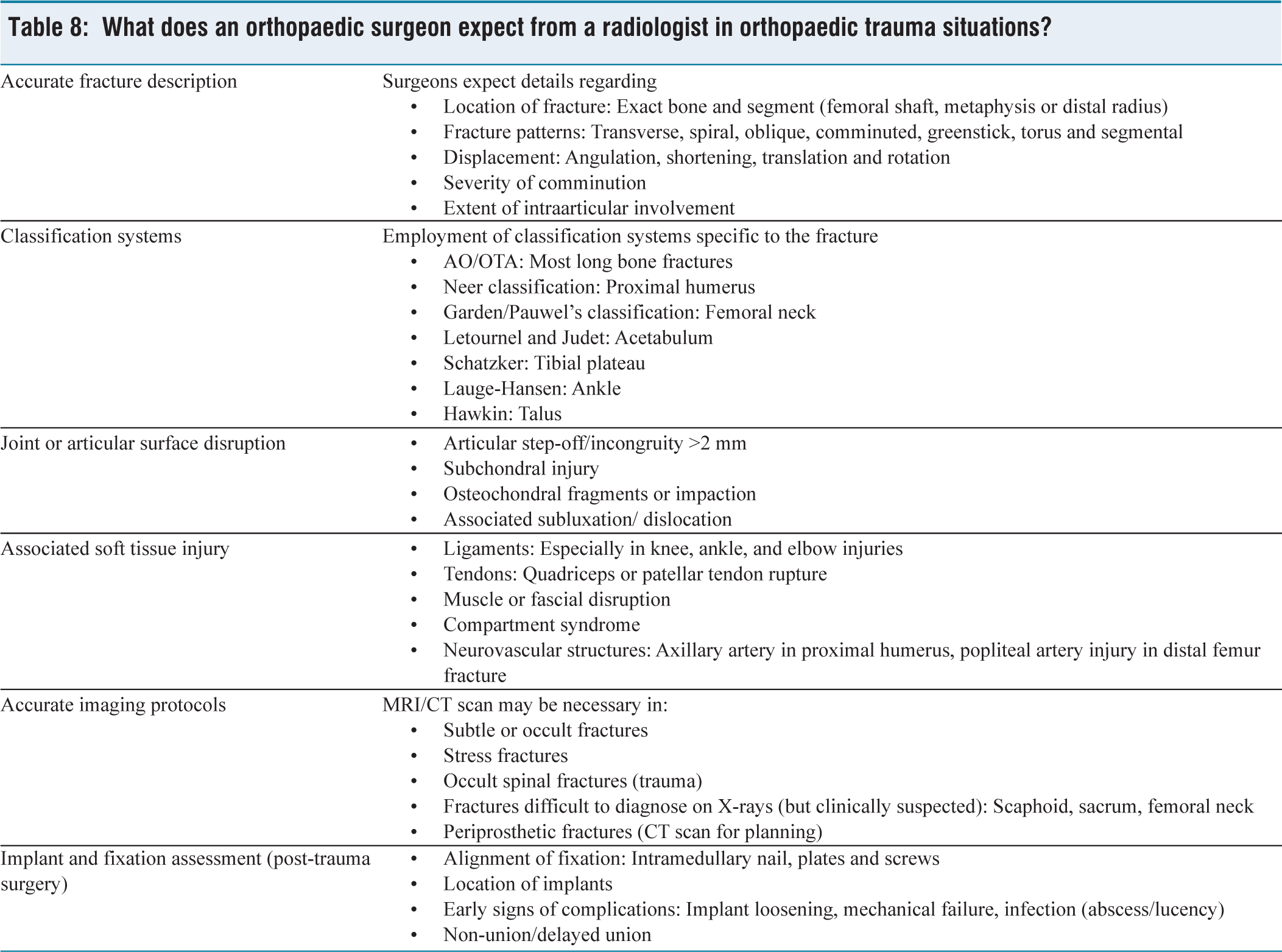
Pathology-based imaging details:
Orthopaedic trauma (Fracture management): Radiologists must be aware of diverse crucial parameters in the context of fracture management (a) commonly-used fracture classification systems (e.g., Schatzker classification for proximal tibia fractures, Neer classification for proximal humerus fractures, Garden classification for femoral neck fractures), (b) Thresholds for displacements and angulations (conservative vs. operative), (c) threshold for intraarticular step-off or displacements, (d) physeal involvement and status in paediatric trauma, as well as (e) associated ligament or chondral damage. While the surgeon usually expects the radiologist to evaluate the stability of the fractures, and even provide opinions regarding surgery (including the surgical approach or type of implant for fracture pattern), the radiologists need to be educated on the general recommendations on surgically- or conservatively-managed fractures.[18,21,23,24] Sports injuries and ligament tears: In general, radiologists’ reports on sports injuries must throw light upon (a) type, location and retraction of the injured ligament or structure, (b) surgical indications for a particular injury, (c) repairability (or re-constructability) of the tear. In order to provide a useful report, the radiologists must be aware of the specific structures of interest in a specific athlete, the relevance of partial and complete tear of the ligament or concerned tissues, grading systems (of ligament [ACL{anterior cruciate ligament}, collateral ligaments] or meniscal tears/labral tears of the hips and shoulders), as well as the surgical relevance of the accompanying findings (e.g., chondral injuries, ramp lesions or osseous contusions in ACL injuries).[21,25,26] In addition, the radiologists must also be aware of clinically relevant sports injury scenarios such as meniscal root versus parrot beak tears. In a recent study, the importance of coordinated association between radiologists and orthopaedic surgeons in the context of treating professional athletes was comprehensively discussed. While they observed that reproducible, plain radiographs must always remain the first step in the radiological evaluation in such challenging situations, the entire diagnostic process in professional athletes must broadly focus upon clearly differentiating acute post-traumatic injuries from chronic, overuse-associated pathologies.[16] In a similar study by Khoury et al.,[11] the critical importance of meticulous communication between radiologists and surgeons in contextualising the data procured from knee MRI (including crucial postoperative details like graft status, alignment and cartilage integrity) was emphasised. Hanna et al.[10] observed that the combined interpretation of preoperative MRI by radiologists and orthopaedic surgeons can aid in the accurate prediction of expected autograft size (as well as identify high-risk patients with a cut-off below 8 mm) in patients undergoing ACL reconstruction. Spinal pathologies: With regard to spinal pathologies, radiological reports ideally provide information on the symptomatic level/segment of spinal pathology, presence of any significant cord compression or canal stenosis, status of the spinal cord (evidence of myelomalacia), and any evidence of intervertebral instability (such as spondylolisthesis, facet arthrosis, or disc space collapse).[9,17,21,27] In a typical scenario of disc herniation, the radiologist needs to provide critical information regarding the location, migration and grading of the disc, the extent of central canal, lateral recess or foraminal stenosis, and the inherent status of the bony canal. Based on these details, the surgeons’ ability to decide on the management strategy can be positively impacted by the radiologist’s interpretation of the imaging studies. In the study by Weber et al.,[17] the clinical impact of detailed reporting of imaging studies by radiologists in the context of emergency thoracolumbar (TL) fractures was discussed from the perspectives of financial logistics and clinical delays. They concluded that radiologists’ interpretation of preoperative X-rays and CT had a significant cost-benefit advantage; however, such an advantage was not extended to routine reporting of intraoperative fluoroscopy and postoperative radiographs. Infections/tumours: A radiologist must be aware of the ideal MRI sequences (STIR, fat-suppressed sequences or contrast-enhanced images) sensitive to infective or neoplastic pathologies, relevant information critical to decision-making on the management (including the localised or diffuse presentation of the pathology, relevant margins, and extent of joint/physeal or intervertebral disc involvement); as well as staging (e.g., Enneking staging in musculoskeletal malignancies) of these pathologies.[28–31] Radiologists must be able to clear the diagnostic dilemma in differentiating between infections and neoplasms (in difficult clinical scenarios), identify the patterns of osseous involvement (say, type of tumour matrix [chondroid or osteoid matrix in tumours], patterns of bony infection [Brodies abscess or subperiosteal spread of purulent material], etc.); and determine the thresholds or provide recommendations for surgical interventions. Postoperative imaging: An ideal postoperative reporting must clearly distinguish between normal postoperative findings and complications or adversities (such as non-union/mal-union, mechanical failures such as implant loosening or migration, and infections). The radiologists must be aware of the normal timelines for tissue healing (such as soft tissue healing, fracture union, graft incorporation and fusions), types of orthopaedic implants (and their typical appearances on different imaging studies), specific imaging findings for the concerned surgical interventions (e.g., early peri-prosthetic lucencies in aseptic loosening, and pseudotumor formation in total hip arthroplasties [THA]); and the intended outcome following diverse surgeries.[9,13,21,32,33] In the study by Ghodasara et al.,[9] the role of radiologists in clearly assessing postoperative CT scans after spinal surgeries was discussed. It was observed that radiologists must be aware of the different spinal instrumentations (integrity and positions), normal postoperative findings (and be able to clearly distinguish from a wide array of potential complications like collections, pseudo meningocele, fistulae, infections, adjacent segment degeneration and mechanical hardware failures) in order to ensure optimal patient management. In another study by Marshall et al.,[13] the importance of timely evaluation of patients with periprosthetic fractures (after THA) by a radiologist was discussed. The crucial information in such scenarios includes the patterns of fractures, stability of prosthesis and quality of the individuals’ bone stock (critical parameters in Vancouver classification). Paediatric orthopaedic pathologies: The radiologists must understand the anatomy of physis (and conditions which lead to injuries to physis/Salter-Harris classification of physeal injuries), congenital or developmental variations in different paediatric disorders (e.g., differentiate between Perthes disease and transient synovitis), and the underlying pathophysiology’s of diverse common paediatric conditions (like Perthes disease, slipped capital femoral epiphysis, developmental hips dysplasia’s, etc.).[34,35] The reports must clearly describe the thresholds for surgical interventions in various paediatric pathologies, congenital limb pathologies and different paediatric fractures (or situations which led to potential arrests of growth plates).
What are the expectations of an orthopaedic surgeon from a radiologist w.r.t pathologies of diverse osteoarticular regions?
Irrespective of the osteoarticular region under evaluation, there are specific expectations from a clinician’s perspective regarding the imaging protocol carried out and the final report provided by a radiologist. The presentation of an accurate and comprehensive diagnosis (or provision of relevant differential diagnosis, which may need to be ruled out), interpretation of the clinical and practical relevance of these imaging findings, recommendations regarding the treatment strategies (including surgical planning), comprehensive utilisation of relevant sequences and imaging protocols (to clearly define the pathology based on the available clinical scenario); as well as timely communication of the relevant results to the clinical team are some of the primary expectations from a radiologist.[9–13,20,21] The general expectations from an orthopaedist’s perspective with regard to the imaging studies for different osteoarticular pathologies (spine, hip, knee, shoulder and musculoskeletal trauma) have been presented in Tables 3–8.
In a recent study by Thierfelder et al. (2018),[15] the investigation pathway to arrive at a clinical diagnosis in ankle injuries was discussed. They observed that, as with any injury, clinical assessment (involving inspection, palpation and stability evaluation) along with appropriate history-taking forms the foremost step. Conventional X-rays (anteroposterior and lateral projections) are crucial to exclude associated osseous injuries. In the context of ligament and tendon injuries, ultrasound (USG) examination can hold a critical role, and in the hands of an experienced assessor, has excellent accuracy too. According to USG guidelines of the ESSR (
In another recent study by Putz et al.,[14] the role of gait assessment in clinical evaluation of foot pain was discussed. Based on interdisciplinary communication, the reasonable imaging diagnostic modalities must be planned, keeping in mind their relative costs and radiation exposure. They observed that imaging forms the basis for monitoring the course of disease progression, surgical planning, intraoperative radiological support, and postoperative assessment (especially in challenging situations of foot deformity correction and Charcot’s arthropathy).
In another article by Lenz et al.[12] on a radiologist’s role in the assessment of elbow pathologies, a similar imaging armamentarium was recommended, which includes conventional plain X-rays, USG, CT (to assess for bony anatomy, especially in intra-articular pathologies), and MRI. They concluded that good interdisciplinary communication (between the radiologists and physicians) was essential to improve the quality of radiological assessment and interpretation in the context of traumatic and non-traumatic elbow disorders. The responsibility of ascertaining optimal availability of images by the time the patient reaches the operating room (OR) must be shared by the radiologists (including efforts such as the employment of internet-based solutions to compensate for insufficient image resolution, and procure appropriate image analysis, like length and angle measurements). Detailed radiological reports also have crucial medicolegal consequences, which may not be overlooked in the present-day situation.
Limitations
Our review has limitations inherent to non-systematic review studies. No specific criteria were employed to evaluate the methodological quality or ‘risk of bias’ of the reviewed studies. There are only a few studies, hitherto published, which have directly evaluated the importance of close communication and mutual participation of radiologists and orthopaedic surgeons in diverse clinical situations.
Conclusion
The radiologists must be appropriately educated by the clinician regarding the specific reasons underlying the diagnostic demands, in order that the ideal imaging modality is chosen in a given scenario. Different imaging modalities have specific roles in diverse clinical scenarios (like preoperative diagnosis, surgical or treatment planning, and postoperative surveillance). Mutual consideration of the patients’ functional status and direct communications between orthopaedic surgeons and radiologists (in appropriate situations) can substantially improve the treatment strategy and ameliorate the overall outcome in a majority of patients.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Not applicable.
Credit author statement
Vibhu Krishnan Viswanathan: Methodology, Formal analysis and investigation, Writing – original draft preparation.
Vijay Kumar Jain: Conceptualisation, Methodology, Writing – review and editing, Resources, Supervision.
Surabhi Subramanian: Methodology, Writing – review and editing, Resources, Supervision.
Karthikeyan P Iyengar: Conceptualisation, Methodology, Writing – review and editing.
Data availability
Not applicable.
Use of artificial intelligence
None.