
Abstract
Introduction:
Acute kidney injury (AKI) is a leading cause of morbidity and mortality in critically ill and its progression invokes substantial resource utilisation. Both early preemptive renal replacement therapy (RRT) and late reactive RRT worsen outcomes. Availability of a bedside tool to predict the need for RRT will help tailor the care of patients with AKI better. Our objective was to evaluate the ability of the Furosemide Stress Test (FST) in predicting the progression of AKI and requirement of RRT within a week.
Material and Methods:
Participants included were critically ill adults with Acute Kidney Injury Network (AKIN) Stage 1 and 2 kidney injury, admitted in a tertiary-level multidisciplinary critical care unit. The two-hour urine output of more than 200 ml was considered a positive response after a single weight-based dose of furosemide (1 or 1.5 mg/kg in the presence of prior exposure).
Results:
After screening 118 patients, FST was performed in 75 critically ill patients who met the inclusion criteria. By the end of the first week, 27 patients out of the 30 non-responders and five patients out of the 45 responders had progression of AKI. Analysis showed negative FST to have 90% positive predictive value (PPV), 88.9% negative predictive value (NPV) with a significant P value (<.01) and an area under the receiver operator characteristic (ROC) curve of 0.896 in predicting progression of AKI. At the end of seven days, 25 patients among the 30 non-responders, and four patients out of the 45 FST responders, ended up requiring RRT. Analysis showed negative FST to have 83.3% PPV, 89.1% NPV with a significant P value (<.01) and an area under the ROC curve of 0.888 in predicting the requirement of RRT at the end of one week.
Conclusion:
FST is an effective clinical tool for predicting AKI progression, the need for RRT in critically ill patients and can guide decision-making regarding initiation of RRT.
Introduction
Acute kidney injury (AKI) is common in critically ill patients and leads to increased morbidity and mortality.[1] The incidence of AKI among hospitalised patients ranges from 7.0% to 18.3%, but can be as high as 20%–50% in critical care units.[2] The course of AKI after it occurs depends on host factors, aetiology and disease severity. There are currently no bedside tools to accurately stratify and predict the course of early-stage AKI[3] in the intensive care unit (ICU) setting. Definitive treatment of progressive AKI with physiologic derangements in this population is renal replacement therapy (RRT). The decision to initiate RRT is based on both objective criteria and the physician’s clinical judgment. Both early pre-emptive RRT and delayed RRT seem to adversely affect outcomes. Studies have clearly demonstrated that a large proportion of patients with AKI improve their renal function and never need RRT.[4,5] On the other hand, outcomes are poor when RRT is started after the onset of acidemia, fluid overload and other organ dysfunctions. Although several risk prediction models and biomarkers are being evaluated to identify patients with AKI progressing to requiring RRT, their current clinical use is limited by a lack of good data or unavailability. A standard dose of furosemide and the urine output response (Furosemide stress test- FST) is a surrogate of the integrity of renal perfusion and tubular function and has been shown to be a good predictor of the severity of AKI and its progression.[6] Considering its easy application at the bedside and its low cost, we sought to evaluate the utility of FST in predicting AKI progression and need for RRT in our single-centre study.
Material and Methods
The study was conducted after Internal Ethical Committee approval (AMH-DNB-027/08-20), between August 2020 and October 2021 at a tertiary-level urban teaching hospital. After obtaining informed consent, we enrolled critically ill patients above 18 years with AKIN Stage I and Stage II AKI from our mixed medical-surgical and cardiothoracic units. Patients with baseline estimated Glomerular Filtration Rate (eGFR) <30 ml/min/1.73 m2 and renal allograft, pregnancy, obstructive uropathy, chronic liver disease (CLD), burns, rhabdomyolysis, known furosemide allergy, recent use (<48 hours) of diuretics other than furosemide, hypovolemia, noradrenaline requirement greater than 0.1 mcg/kg/min or multiple vasopressors were all excluded from our study.
As per Rewa et al.,[7] the sensitivity of FST in predicting AKI progression was considered to be 73.9%. Considering a standard normal variate of 95% with a confidence interval of 1.96, our calculated sample size was 73. A weight-based furosemide bolus dose of 1 mg/kg was given over five minutes to furosemide naïve patients, and a bolus dose of 1.5 mg/kg was given over five minutes to patients who were exposed to furosemide within the previous seven days. Following a furosemide bolus, hourly urine output was monitored for the first six hours. Intravenous fluid administration to replete any volume loss due to excessive diuresis was allowed at the discretion of the treating physician after the first two hours and continued for six hours after the FST.
All continuous variables are represented by mean ± SD. Numbers and percentages (%) are used for the presentation of the categorical variables. Sensitivity, specificity, PPV and NPV were computed by taking a cut-off urine output of 200 ml at two hours in our study.[6] Comparison of categorical variables was done by chi-square test or Fisher’s exact test. Comparison of continuous variables was done by a sample t-test. A ROC curve was obtained to find the optimal cut-off in predicting the progression of AKI and the need for RRT. Data entry was done on an MS-Excel spreadsheet. Data analysis was done using SPSS version 25.0. All P values <.05 were considered statistically significant.
Our outcomes were to observe the ability of FST to predict progression of AKI (Stage I to II, Stage I to III, Stage II to III) and the need for RRT within seven and 14 days of FST. We also observed whether FST can predict the length of ICU stay, hospital mortality and RRT dependence at 30 days.
Results
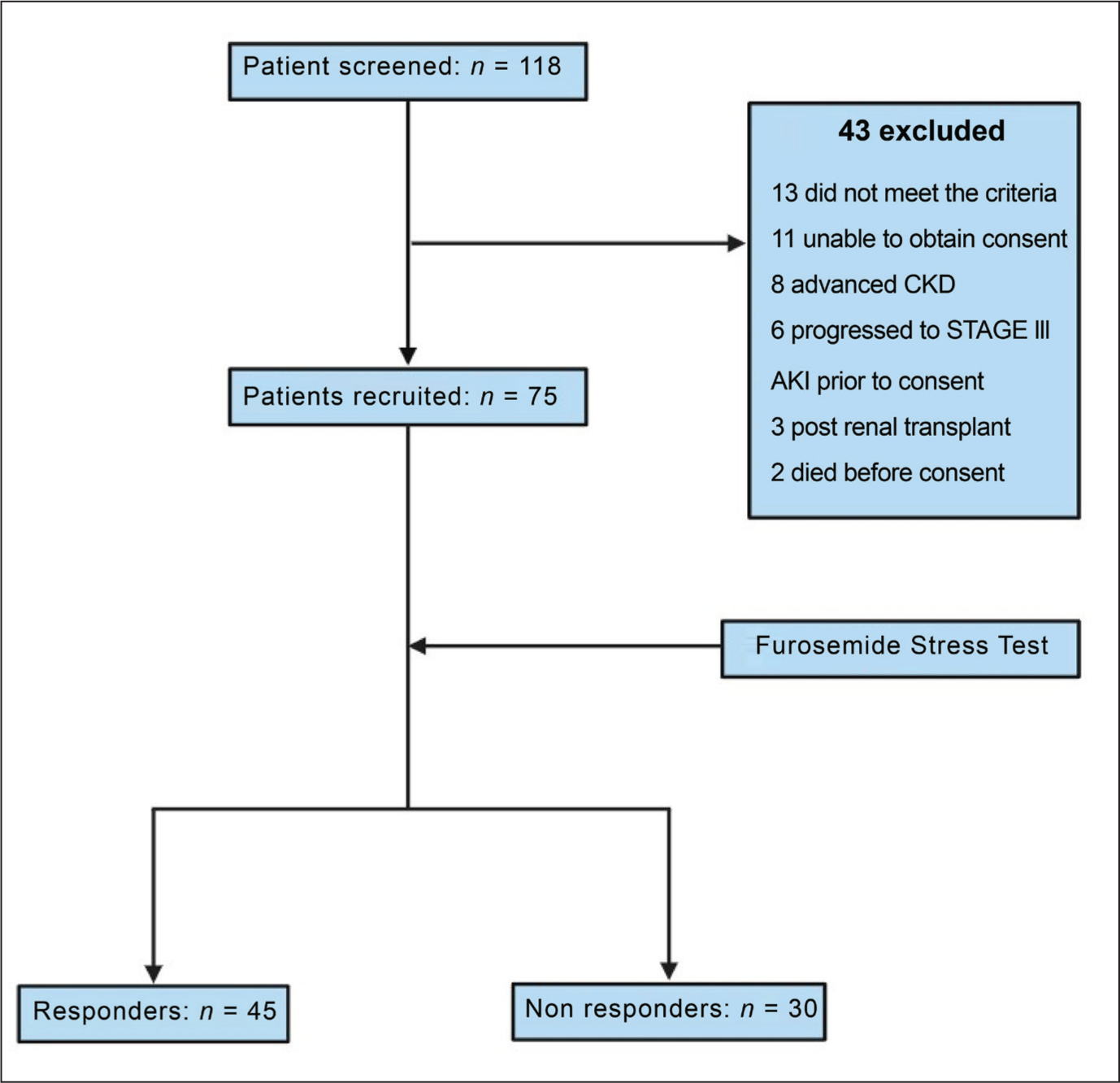
A total of 118 patients were screened, out of which 43 were excluded [Figure 1]. The remaining 75 patients were enrolled on the study and subjected to FST.
Patient enrolment flow sheet
Characteristics of the Patients
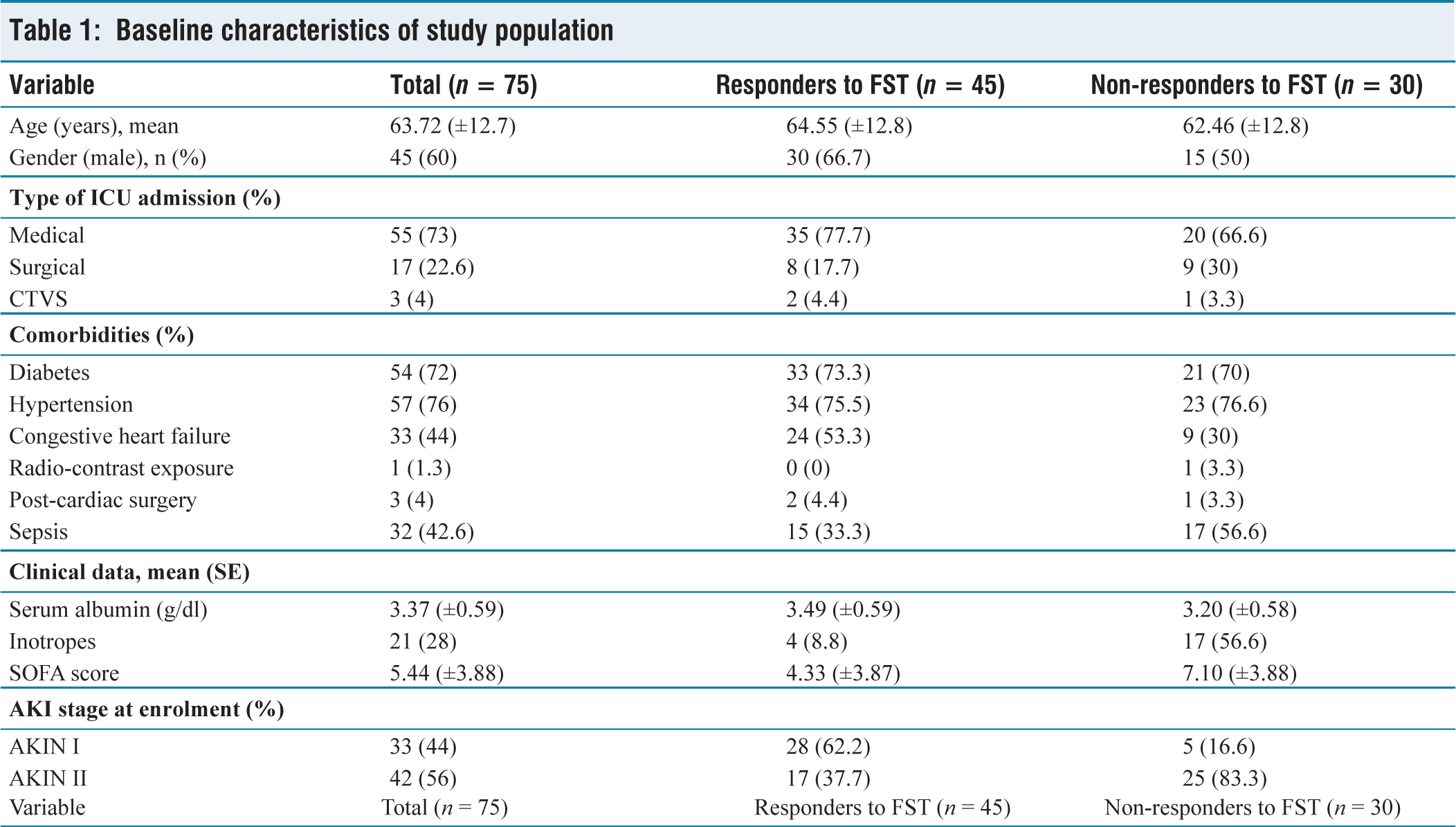
Among the 75 patients, the average age was 63.7 years, with males accounting for 60%. The prevalence of systemic hypertension was 76%, diabetes mellitus was 72% and congestive heart failure was present in 44% of the patients. The study population was mainly critically ill medical patients (73%), while surgical patients contributed 27%. Sepsis was the diagnosis in 42.7% patients, and the mean SOFA score was 5.44, with 28% patients requiring vasopressor support. 29.3% patients had a serum albumin concentration in the range of 2–3 g/dL, the remaining 70.7% had more than 3 g/dL, resulting in a mean serum albumin concentration of 3.37 g/dL. AKI Stage I was seen in 44% of patients on recruitment, while 56% were recruited with AKI Stage II [Table 1].
Baseline characteristics of study population
FST Response and AKI Progression
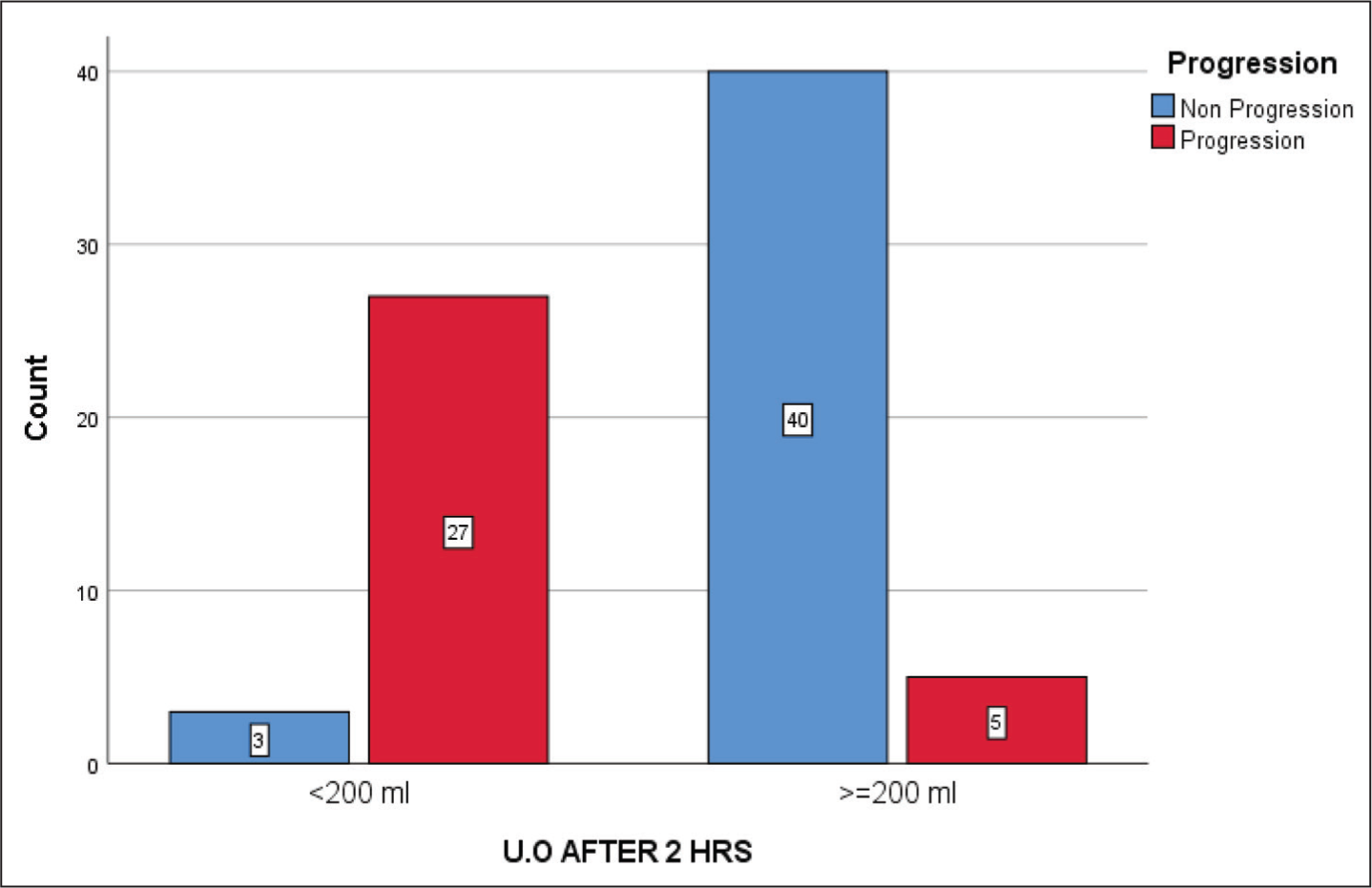
The mean dose of furosemide was 58.7 mg and the mean urine output at the end of two hours was 238.5 ± 166.4 ml. Out of 75 patients who underwent FST, 45 patients (60%) were responders and 30 patients (40%) failed to show adequate response. The mean urine output at two hours was 343.8 ± 131.3 ml in responders and 80.5 ± 49.7 ml in non-responders. By the end of the first week, 27 patients out of the 30 non-responders and five patients out of the 45 responders had progression of AKI. Among the 32 patients who had AKI progression, 27 patients progressed from AKI Stage II to AKI Stage III, three patients progressed from AKI Stage I to AKI Stage III and two patients from AKI Stage I progressed to AKI Stage II [Figure 2].
Response to FST and AKI progression
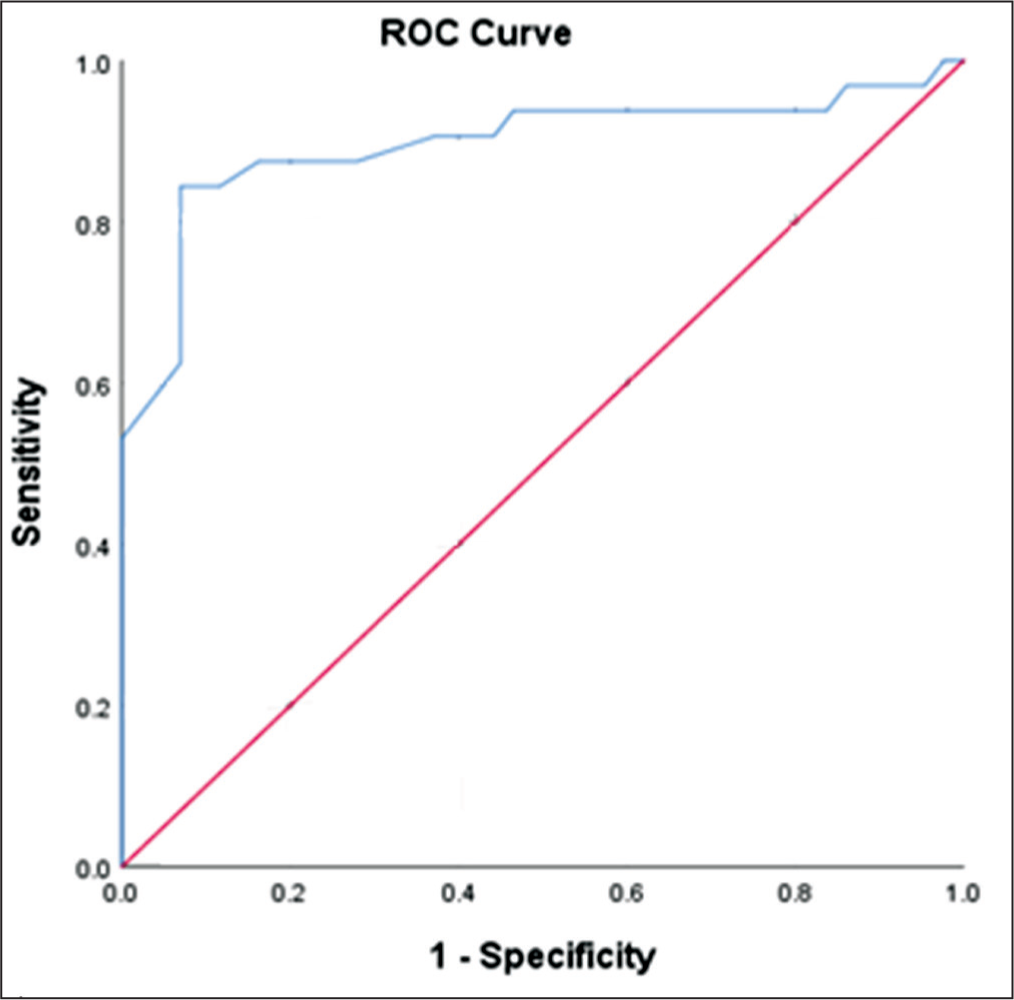
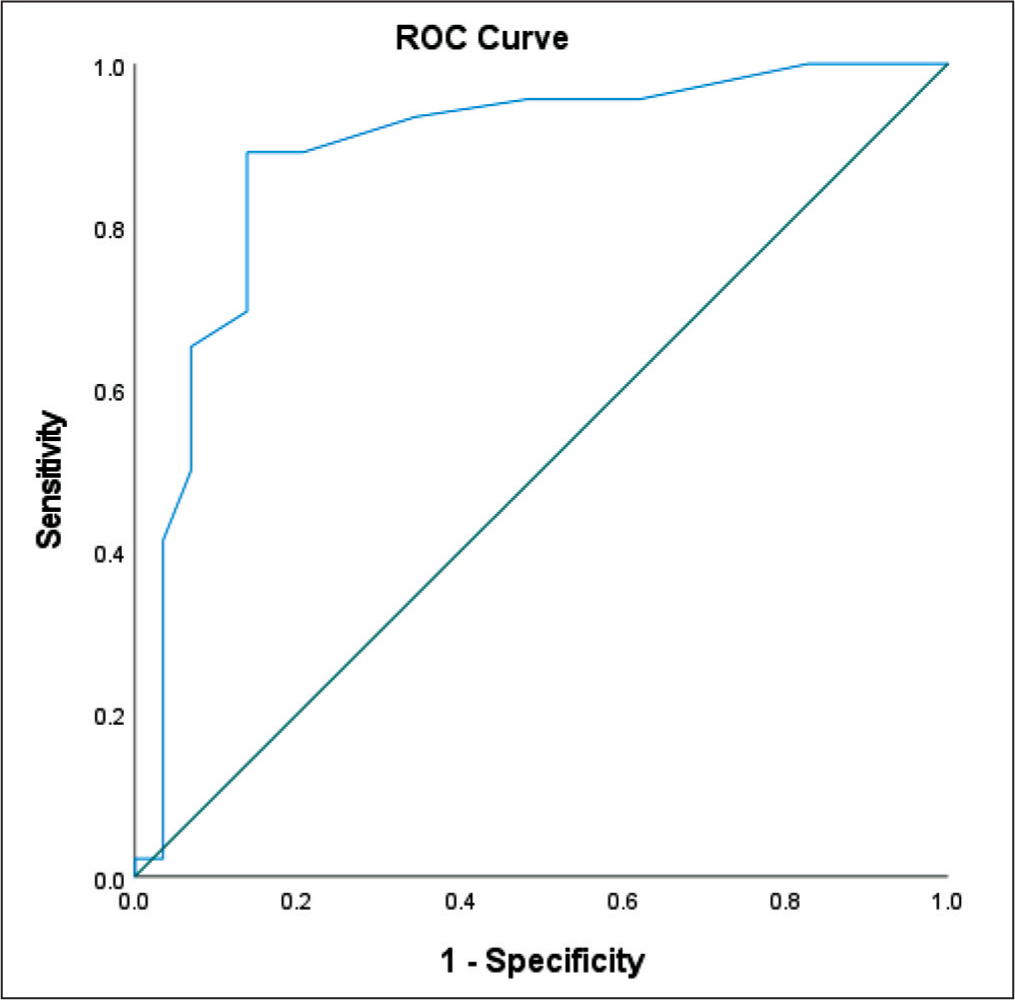
Our analysis showed FST to have 84.4% sensitivity, 93% specificity, positive predictive value (PPV) of 90% and negative predictive value (NPV) of 88.9% with a significant P value (<.01) in predicting progression of AKI. The receiver operator characteristic (ROC) curve showed an area under the curve of 0.896 [Figure 3].
The area under the ROC curve for the total urine output of less than 200 ml over the first two hours following FST to predict AKI progression
At the end of seven days, 25 patients among the 30 non-responders required RRT. In comparison, only four patients out of the 45 FST responders ended up requiring RRT. Analysis of the above data showed FST to have 86.2% sensitivity, 89.1% specificity, 83.3% PPV and 89.1% NPV with a significant P value (<.01) in predicting the requirement of RRT. The ROC curve showed an area under the curve of 0.888 [Figure 4].
The area under the ROC curve for the total urine output of less than 200 ml over the first two hours following FST to predict the requirement of RRT
By the end of 14 days, 12 patients among the 30 non-responders required RRT. In comparison, only three patients out of the 45 FST responders ended up requiring RRT. Analysis of the above data showed FST to have 80% sensitivity, 70% specificity, 40% PPV and 90% NPV.
ICU Length of Stay and Hospital Mortality
The mean ICU length of stay of 75 patients included was 10.23 days with a standard deviation of 9.13 days. Patients who failed FST had a mean ICU stay of 12.5 days, which was not statistically significant. FST was unable to predict mortality in our study, as 11 patients out of the 21 patients who contributed to the mortality failed the FST.
Discussion
In our prospective single-centre study, we explored the role of FST in predicting AKI progression of 75 critically ill patients admitted to our medical, surgical and cardiothoracic ICUs. The mean age in our study population was 63.72 ± 12.7 years, which was comparable to the previous studies by Chawla et al.[6] and Rewa et al.[7]
Similar to Rewa et al.,[7] we noted that AKI incidence was higher in the medical ICU compared to the surgical ICU. Multiple comorbidities, multiple organ involvement, prolonged ICU stay and severity of illness could be the factors contributing to this. Our study had a higher proportion of septic patients (42.6%), similar to Venugopal et al.[8] compared to the other studies.
Unlike the Chawla et al.[6] study who calculated the eGFR, we obtained the baseline serum creatinine at the time of FST administration to capture real-world practices. The mean serum creatinine in our study was 0.91 mg/dl, which was considerably lower than the 1.23 mg/dl of the Rewa et al. 7 study.
Our study population’s mean Sequential Organ Failure Assessment (SOFA) score of 5.44 (±3.88) was significantly higher than the previous studies, probably due to a higher number of sepsis cases. On analysis, non-responders had a higher SOFA score (7.10 ± 3.88), most likely due to the contribution of AKI, hemodynamic instability and organ dysfunction.
Unlike previous studies like Venugopal et al.,[8] we noted the baseline serum albumin levels as albumin binding is an essential step in furosemide pharmacokinetics. Patients with serum albumin <2 g/dL and CLD were excluded from our study, as this would affect the performance of FST. However, almost 30% of our study patients had a serum albumin of 2–3 g/dl, which could have affected our study results. Whether patients with albumin <3 g/dl need a higher dose of furosemide or a different cut-off needs to be evaluated.
A 28% of our study population needed at least single vasopressor support (Noradrenaline <0.1 mcg/kg/min) at the time of FST. A significant percentage of these patients (81%) did not respond to FST. This could possibly be due to septic aetiology and hypotension contributing to the AKI. We did not capture hemodynamic data after furosemide administration, and whether transient hypotension related to furosemide-induced venodilatation contributed to a negative FST is not known. Such an analysis was not performed in the previous studies.
Our mean SOFA score (5.40 ± 3.88) was higher than the previous studies, probably due to a higher number of sepsis cases. On analysis, non-responders had a higher SOFA score (7.1 ± 3.88), most likely due to the contribution of AKI, hemodynamic instability and other organ dysfunction.
The dosage requirement of diuretics was less compared to the previous studies, as most of our patients (98.6%) were not exposed to diuretics earlier.
Chawla et al.[6] and Rewa et al.[7] evaluated the progression of AKI and requirement of RRT at day 14 after FST, but we evaluated after seven days of FST due to the possibility of occurrence of multiple confounding factors, such as new onset sepsis, hypotension over 14 days. Among the 29 patients who required RRT within seven days, 25 patients (86.2%) were non-responders, indicating that FST can predict RRT requirement within seven days.
The AKI progression in our study (42.7%) was higher than what was observed by Chawla et al.[6] (32.4%) and significantly higher than the 25% observed by Rewa et al.[7] The majority (84.3%) of those whose AKI progressed were in AKIN Stage II during FST. Similar findings were noted by Chawla et al.[6] This could probably indicate that the higher the grade of AKI, the higher the risk of progression. This is also supported by the fact that 84.8% of AKIN I patients were responders, whereas 59.5% of AKIN II patients were non-responders. The more severe the AKI, the less response to FST, the more probable progression of AKI.
Although statistically insignificant, FST non-responders had a longer ICU stay with a higher SOFA score, hemodynamic instability, and AKI itself per se contributing to the increased ICU stay. In contrast to Venugopal et al.,[8] we were unable to find any mortality difference between FST responders and non-responders. This result was in agreement with Chawla et al.[6] and Rewa et al.[7]
Post FST urine output of less than 200 ml in two hours was able to predict AKI progression in our critically ill patients with an area under the curve (AUC) of 0.896, similar to what Chawla et al.[6] (0.87) and Rewa et al.[7] (0.87) observed. The sensitivity (84.45%) and specificity (93%) were also similar to the results obtained previously.
Our study is one of the very few prospective studies that have tried validating the FST in the critically ill Indian population. We included baseline characteristics like serum albumin and inotrope requirement, which were not done in the previous studies. We analysed the performance of FST within seven days to detect early progression of AKI.
Our study had a few limitations. First, since we excluded patients with CLD and hypoalbuminemia, these results may not be applicable to that group of patients. Hypoalbuminemia is common in the critically ill and this reduces the generalizability of our results. Second, FST may also have utility in predicting the progression of AKIN Stage III, which we did not evaluate. Third, the decision to initiate RRT was left to the clinician’s discretion; no objective criteria were used and ours was a single-centre study.
Conclusion
We conclude that FST is an excellent clinical tool that accurately predicts the progression of AKI in a critical care setting. FST non-responsiveness has a good ability to predict the progress of AKI and RRT requirement within seven days. Hence, this test can be used in select critically ill patients with early AKI to stratify their risk of progression and to decide about the need for RRT.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Ethical approval obtained prior to the research as mentioned in the manuscript. Institutional ethical committee approval number: AMH-DNB-027/08-20.
Informed consent
Yes.
Patient consent
No patient consent required for publication.
Credit author statement
Dr Kishor Kumar Rajasekaran: Data curation; Formal analysis.
Dr R Bharatram: Formal analysis; Writing - original draft; Writing - review & editing.
Dr Balaji Rajaram: Supervision; Writing - review & editing.
Dr Vivek Vadamalai: Data curation; Methodology; Supervision.
Dr Ramesh Venkataraman: Conceptualisation; Methodology; Supervision, Writing - review & editing.
Data availability
Available.
Use of artificial intelligence
No.