
Abstract
Background
The choice of kidney replacement therapy (KRT) modality for treatment of dialysis requiring acute kidney injury (AKI-D) is underappreciated as a modifiable factor that can impact outcomes. Peritoneal dialysis (PD) and extracorporeal dialysis are both established modalities for treatment of kidney failure; their comparative effectiveness in AKI remains controversial. We conducted a systematic review and meta-analysis to compare clinical outcomes between PD and extracorporeal dialysis in patients with AKI.
Methods
We systematically searched Medline, Embase, and Cochrane Central Register of Controlled Trials from inception through November 2024 for randomized controlled trials comparing PD with extracorporeal dialysis in adult patients with AKI requiring KRT. The primary outcome was mortality. Secondary outcomes included kidney function recovery, time to kidney function recovery, and infectious complications. We conducted meta-analyses using random-effects models and assessed risk of bias using the Cochrane Risk of Bias tool 2.0.
Results
About 358 records were identified, of which 7 were included in quantitative meta-analysis. We found no significant difference in mortality between PD and extracorporeal dialysis (odds ratio [OR] 1.05; 95% confidence interval [CI], 0.62–1.76; p = 0.87). Event rates were similar between groups (PD: 56.1%, extracorporeal: 56.5%). Kidney function recovery rates were comparable (OR 1.26; 95% CI, 0.81–1.95; p = 0.30), though time to kidney function recovery was significantly shorter with PD (mean difference −3.34 days, 95% CI −3.95 to −2.73, p < 0.00001). Infection rates were similar between modalities (OR 1.02, 95% CI 0.47–2.22, p = 0.96).
Conclusion
This meta-analysis demonstrates comparable clinical outcomes between PD and extracorporeal dialysis for AKI management across key metrics including mortality, kidney function recovery, and infectious complications. PD was associated with faster time to kidney function recovery. These findings support the use of PD as an equally effective treatment for AKI-D. Further research is needed to evaluate patient-reported outcomes and patient modality preference.
Introduction
Acute kidney injury (AKI) affects approximately 5–7% of hospitalized patients, with higher rates of up to 50–57% in critically ill patients.1–4 This common complication is associated with substantial morbidity and mortality, with in-hospital mortality rates ranging from 5–13% in general hospitalized patients to as high as 34–43% in intensive care settings.4–8 In AKI requiring dialysis (AKI-D) hospital mortality rate are range 20–30%, increasing to 45–50% in critically ill subgroups.9,10 While extracorporeal dialysis methods, particularly continuous kidney replacement therapy (CKRT) and intermittent hemodialysis (IHD), have become the standard of care in many high resource nations, peritoneal dialysis (PD) continues to play a vital role, especially in resource-limited settings.11–19
Historically, PD was the primary modality for managing AKI since its first successful use in 1946. 20 PD offers several advantages including technical simplicity, hemodynamic stability, and lower cost.11,21,22 However, with technological advances in extracorporeal techniques, the use of PD has declined in many centers.11,23,24 In the United States, with the exception of during the COVID-19 pandemic, PD is rarely used in the setting of AKI due to historical Medicare payment policies that reimbursed AKI-D treatments in outpatient dialysis units but not if performed in the home.25–29 However, recent changes implementing site-neutral payments may influence future practice patterns.
The comparative effectiveness of PD versus extracorporeal dialysis in AKI remains controversial. Previous meta-analyses have shown conflicting results, with some suggesting comparable outcomes between the two modalities and others indicating potential advantages or disadvantages for specific patient populations.30,31 The most recent Cochrane review, published in 2017, concluded that based on moderate-quality evidence, there appears to be little or no difference in mortality or recovery of kidney function between PD and extracorporeal therapies. 31 Since then, additional randomized trials have been published, and equipoise remains.
This systematic review and meta-analysis aim to compare the clinical outcomes of PD versus extracorporeal dialysis in patients with AKI. Our primary objective is to evaluate mortality differences between the two modalities. Secondary objectives include comparing rates of kidney function recovery, time to kidney function recovery, and infectious complications. By synthesizing the available evidence, we seek to provide clinicians with data-driven insights to inform the selection of RRT modality for patients with AKI, considering both clinical effectiveness and resource utilization, particularly in the context of new policies bringing site neutrality to outpatient AKI-D management in the US.
Methods
Study design
We conducted a systematic review and meta-analysis following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Supplementary Table 3). The review protocol was prospectively registered with Open Science Framework Registries (10.17605/OSF.IO/CNW2X).
Literature search
We systematically searched Medline, Embase, and Cochrane Central Register of Controlled Trials from inception through November 2024. The search strategy combined terms related to acute kidney injury, peritoneal dialysis, and extracorporeal dialysis modalities, including their variations and synonyms (Supplemental Table 1). Additional studies were identified through manual review of reference lists from relevant articles and previous systematic reviews.
Eligibility criteria
Studies were eligible for inclusion if they were randomized controlled trials comparing peritoneal dialysis with extracorporeal dialysis modalities in adult patients with acute kidney injury requiring KRT. We included English-language, full-text articles that reported at least one of our outcomes of interest: mortality, kidney function recovery, time to kidney function recovery, or infection rates. Studies were excluded if they were case reports or case series, lacked a comparison group, or did not report our outcomes of interest.
Data extraction
The study selection process involved three independent reviewers who screened titles and abstracts of identified articles. Full texts of potentially eligible studies were then assessed for inclusion, with disagreements resolved through consensus. Two reviewers independently extracted data using a standardized form. The extracted information encompassed study characteristics including author, year, country, design, and setting; patient demographics and baseline characteristics; intervention details regarding the type of peritoneal dialysis and extracorporeal modality; outcome measures including mortality, kidney function recovery, time to recovery, and complications; follow-up duration; and quality assessment criteria.
Quality assessment
We evaluated risk of bias using the Cochrane Risk of Bias tool 2.0 for randomized controlled trials. The assessment examined the randomization process, allocation concealment, blinding, incomplete outcome data, selective reporting, and other potential sources of bias.
Data analysis
Data from eligible studies were extracted and analyzed using Review Manager (RevMan) Web version (The Cochrane Collaboration, Copenhagen, Denmark). For dichotomous outcomes (mortality, kidney function recovery, and infectious complications), we calculated odds ratios (ORs) with 95% confidence intervals (CIs) using the Mantel-Haenszel random-effects model. For continuous outcomes (time to kidney function recovery), we computed mean differences with 95% CIs using the inverse variance method with random effects.
Statistical heterogeneity was quantified using the I2 statistic, with values of 25%, 50%, and 75% indicating low, moderate, and high heterogeneity, respectively. We also calculated the chi-square test for heterogeneity, with p < 0.05 indicating significant heterogeneity. To explore potential sources of heterogeneity, we planned subgroup analyses based on the type of extracorporeal modality. Publication bias was assessed through visual inspection of funnel plots and Egger's test. We considered p < 0.05 as statistically significant for all analyses. A sensitivity analysis excluding abstracts without full text was performed.
Results
Study selection
Three hundred fifty-eight (358) records were identified, with 318 screened after removing duplicates. Two hundred ninety-nine (299) of which did not meet the inclusion criteria and were hence excluded. A total of 19 full articles were assessed for eligibility, 10 were included in systematic review and 7 in quantitative meta-analysis. Study characteristics are summarized in Supplementary Table 2. Included trials spanned from 1993 to 2021 across Asia, South America, and the Middle East, with sample sizes ranging from 50 to 157 participants. Across studies, PD prescriptions were predominantly high-volume regimens (30–70 L/day) with frequent exchanges, while extracorporeal modalities included both intermittent hemodialysis and continuous therapies (Figures 1 and 2).

PRISMA diagram.

Mortality.
Primary outcome
Seven studies including 781 patients reported on mortality. In the primary analysis comparing mortality between peritoneal dialysis (PD) and extracorporeal KRT, we found no statistically significant difference between modalities [pooled odds ratio (OR) 1.05; 95% confidence interval [CI], 0.62–1.76; p = 0.87]. Moderate statistical heterogeneity was present (I2 = 63%, p = 0.01). Event rates were 215/383 (56.1%) in the peritoneal dialysis group and 225/398 (56.5%) in the extracorporeal dialysis group. Findings were consistent amongst different forms of extracorporeal dialysis (Supplemental Figure 3) and were also similar when stratified by PD catheter type (Supplemental Figure 4) and study era (Supplemental Figure 5). Individual studies show mixed results, with some favoring PD and others favoring ECD, but the overall data do not demonstrate a clear advantage for either approach.
Secondary outcomes
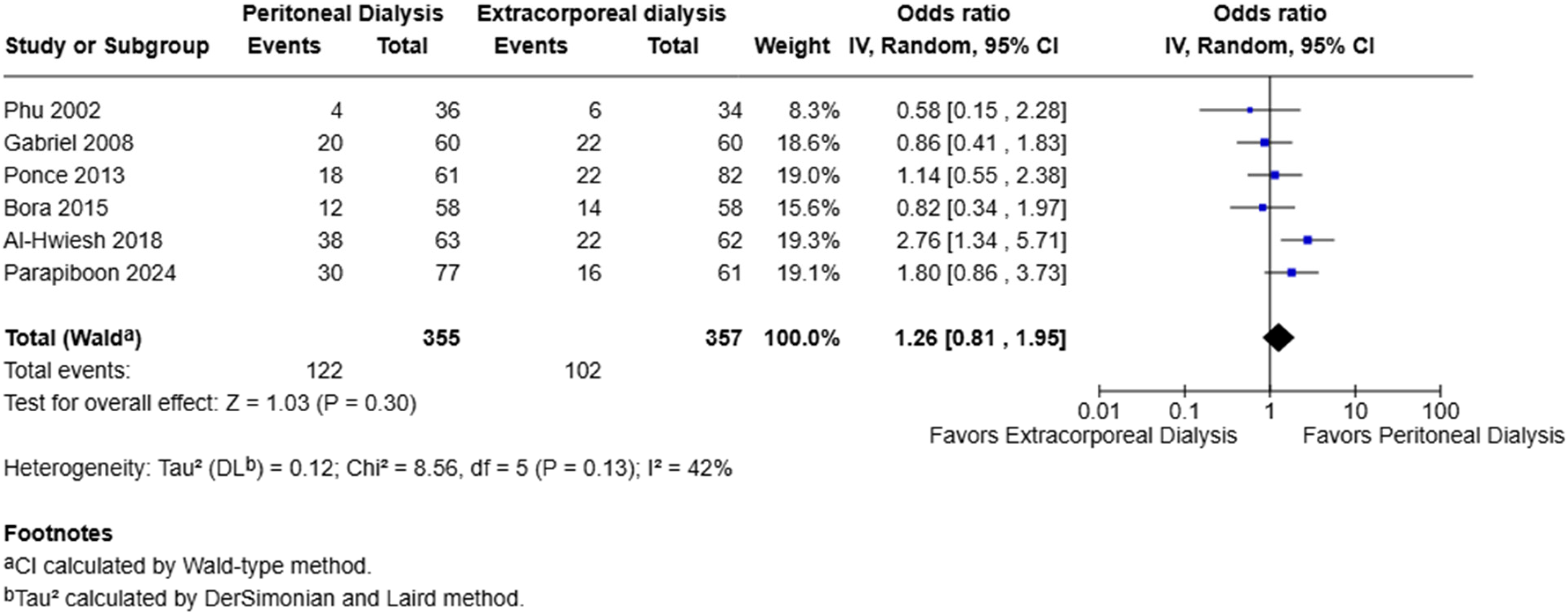
The analysis of kidney function recovery included seven studies with 781 patients (383 receiving peritoneal dialysis and 398 receiving extracorporeal dialysis). The overall pooled analysis showed no significant difference in kidney function recovery rates between peritoneal and extracorporeal dialysis (OR 1.26; 95% CI, 0.81–1.95; p = 0.30). Event rates were similar between groups, with recovery occurring in 215/383 (56.1%) peritoneal dialysis patients and 225/398 (56.5%) extracorporeal dialysis patients. Substantial heterogeneity was observed across studies (I2=63%, p = 0.01). Exclusion of the study by Bora et al. (2015) which was only published as an abstract did not materially alter pooled effect estimates for any outcome (Supplemental Figures 6–7).
Time to kidney function recovery was evaluated across three studies comprising 388 patients. Peritoneal dialysis was associated with significantly shorter time to recovery compared to extracorporeal dialysis (mean difference −3.30 days, 95% CI −3.90 to −2.70, p < 0.00001). This effect was consistent across all studies without any significant between-study variation (Figures 3 and 4).
Kidney function recovery.

Time to kidney function recovery.
Analysis of infectious complications included 4 studies with a total of 458 patients (220 receiving peritoneal dialysis and 238 receiving extracorporeal dialysis). The incidence of infections was 28/220 (12.7%) in the peritoneal dialysis group compared to 32/238 (13.4%) in the extracorporeal dialysis group. The meta-analysis showed no significant difference in infection risk between modalities (OR 1.02, 95% CI 0.47–2.22, p = 0.96), with moderate heterogeneity across studies (I2=38%, p = 0.18) (Figure 5).

Infections.
Analysis of hypotensive episodes (Supplemental Figure 8) included 3 studies with a total of 332 patients (168 receiving peritoneal dialysis and 164 receiving extracorporeal dialysis). The incidence of hypotension was lower in the peritoneal dialysis group at 14/168 (8.3%) compared to 42/164 (25.6%) in the extracorporeal dialysis group. This difference was statistically significant favoring peritoneal dialysis (OR 3.98 95% CI 1.61–9.84, p = 0.003) with low heterogeneity was observed across studies (I2=27%, p = 0.25).
Risk of bias
Risk of bias evaluation revealed varying methodological quality across the included studies (Supplemental Figures 1 and 2). While most studies demonstrated adequate random sequence generation, allocation concealment, and blinding of participants and personnel were universally challenging due to the nature of the interventions. Blinding of outcome assessment was largely accomplished, with the majority of studies showing low risk. Performance bias was therefore assessed as high risk across studies. Selective reporting bias was predominantly low risk, with pre-specified outcomes reported as planned in most studies.
Discussion
In this systematic review and meta-analysis comparing PD to extracorporeal dialysis modalities in AKI, we found no significant difference in mortality between the two approaches. This finding has important implications for clinical practice, bringing further evidence that PD is equally efficacious to extracorporeal therapies and supports greater adoption of its use. Our analysis, which includes the most recent randomized trials, provides robust evidence that while extracorporeal therapies have become the default choice in many high-resource nations, this preference may reflect historical practice patterns and resource availability rather than clinical superiority.
Our secondary analyses revealed several noteworthy findings. While overall AKI recovery rates were comparable between PD and extracorporeal modalities, we observed time to recovery was shorter in the PD group, with a mean difference of −3.34 days (95% CI: −3.95 to −2.73). Infection rates were no different amongst the groups, contradicting traditional assumptions about higher infection risk with PD. These findings suggest that PD may actually be preferable in certain clinical scenarios, particularly in patients with hemodynamic instability or those at high risk for catheter-related bloodstream infections.
These results must be contextualized within the existing literature on patient choice and modality education in KRT. Studies in chronic kidney disease have consistently demonstrated that when patients receive comprehensive education about dialysis options, up to 50% choose PD and there is a lack of evidence on patient modality selection in AKI. 32 This discrepancy between patient preference and clinical practice in CKD stems from systemic factors rather than medical contraindications and these factors are even more prominent in AKI.33,34 In many high resource nations, the shift away from PD was driven partly by technological advances in extracorporeal techniques and historical reimbursement policies.35,36 For instance, in the United States, Medicare payment policies historically favored outpatient hemodialysis over PD for AKI patients. Recent changes implementing site-neutral payments may alter this landscape, potentially leading to renewed interest in PD for AKI management. 37 Geographical and resource considerations significantly impact modality selection. In resource-limited settings, PD often remains the primary modality due to its lower technical requirements and cost-effectiveness.11,21 Our analysis suggests this practice is supported by evidence, as outcomes are comparable to more resource-intensive extracorporeal methods.
Our study has several strengths. First, we included the most recent randomized trials, providing an up-to-date synthesis of available evidence. Second, our comprehensive search strategy and rigorous methodology minimized potential selection bias. Third, we limited our study to only include randomized controlled trials, offering the highest level of evidence available to inform clinical decision-making in AKI management. Additionally, our analysis included trials from diverse healthcare settings across multiple continents, enhancing the generalizability of our findings to both resource-rich and resource-limited environments.
Several limitations warrant discussion. First, the included studies showed considerable heterogeneity in their definitions of AKI, timing of RRT initiation, and outcome measures. Second, many studies were conducted in single centers with varying levels of expertise in different modalities, potentially affecting the generalizability of results. Third, data on important patient-centered outcomes such as quality of life and long-term functional status were limited. Furthermore, not all RCTs reported fluid balance, hemodynamic parameters, or catheter-related complications, limiting comparative analysis of these clinically relevant outcomes. Another limitation of the study is the grouping of extracorporeal dialysis modalities together for the main analysis, which may obscure important modality-specific differences. Additionally, the finding of earlier kidney recovery may be an ascertainment bias, as hemodialysis is typically dosed thrice weekly and peritoneal dialysis daily. Finally, cost-effectiveness analyses were not possible due to insufficient reporting of economic outcomes in the primary studies.
Looking forward, several key questions remain unanswered. Future research should focus on patient perspectives on modality for RRT for AKI-D. Large-scale multicenter trials incorporating standardized definitions and outcomes are needed. Additionally, studies examining the impact of new automated PD technologies and varied prescription approaches could provide insights into optimizing PD delivery in AKI.
The practical implications of our findings are substantial. For clinicians, our results support a more flexible approach to modality selection, considering local resources, expertise, and patient-specific factors rather than assuming superiority of one modality. For healthcare systems, particularly in resource-limited settings, our findings validate the continued use of PD as a modality for AKI management. For policymakers, these results suggest that reimbursement policies should support access to both modalities, allowing for individualized patient care decisions.
Supplemental Material
sj-docx-1-ptd-10.1177_08968608261448781 - Supplemental material for Peritoneal dialysis results in similar outcomes to extracorporeal dialysis in acute kidney injury: A systematic review and meta-analysis
Supplemental material, sj-docx-1-ptd-10.1177_08968608261448781 for Peritoneal dialysis results in similar outcomes to extracorporeal dialysis in acute kidney injury: A systematic review and meta-analysis by Rajiv Hans Menghrajani, Mirtha C Almanzar, Maria Angela Matabang, Saifudheen Faroog, Siena Placino, Anika Sinha, John Paul Aparece and Ankur D Shah in Peritoneal Dialysis International
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: ADS is partially supported by Institutional Development Award Number U54GM115677 from the National Institute of General Medical Sciences of the National Institutes of Health, which funds Advance Clinical and Translational Research (Advance-CTR).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.