
Abstract
Background:
The study aims to evaluate the MRI patterns and severity scores of adult patients with acute global hypoxic-ischaemic encephalopathy (HIE). It also evaluates the predictive value of advanced MRI sequences, such as arterial spin labelling (ASL), susceptibility-weighted imaging (SWI), MR angiography (MRA), and MR venography (MRV).
Methods:
A prospective observational study was conducted at a tertiary care facility between December 2023 and December 2024. Forty-three adult individuals with clinical suspicions of HIE were studied. MRI sequences such as DWI, FLAIR, ASL, SWI, MRA, and MRV were examined to identify specific hypoxic injury patterns and also to generate an imaging severity score. Clinical outcomes were assessed using the cerebral performance category (CPC) scale.
Results:
The majority of cases (97.7%) showed diffuse cortical involvement with deep grey matter and perirolandic areas. Patterns of bilateral medial occipital lobes, perirolandic region, diffuse cortical, diffuse cortical with deep grey matter, deep white matter, brain stem, cerebellum, and hippocampus involvement were strongly related to poor outcomes (CPC-5). On ASL, diffuse hypoperfusion and bilateral medial occipital hyperperfusion, medullary vein prominence on SWI, were associated with poor outcomes. The imaging severity score from all sequences significantly correlated with prognosis (P < .05).
Conclusion:
This prospective study found that MRI, when standard sequences like DWI and FLAIR are paired with advanced sequences like ASL, SWI, MRA, and MRV, is an excellent approach for evaluating the quantity and pattern of acute global hypoxic-ischaemic brain injury (HIBI) in adults. The imaging severity score is a structured approach to stratifying patients by prognosis and guiding management.
Keywords
Introduction
Hypoxic-ischaemic brain injury (HIBI) is a critical condition caused by decreased cerebral oxygenation as a result of cardiac arrest, drowning, or severe hypotension.[1–3] Identifying patients at an early stage who are likely to have positive or negative neurological outcomes is critical for prognosis, treatment decisions, and family therapy. Early prediction of neurological outcomes is critical but difficult, especially as therapeutic hypothermia limits the reliability of clinical indicators.[4–7] MRI, particularly diffusion-weighted imaging (DWI), outperforms CT for early diagnosis and severity assessment in HIBI.[8–10] Furthermore, DWI has been shown to be effective in patients who are in therapeutic hypothermia or sedated. Advanced sequences such as arterial spin labelling (ASL), susceptibility-weighted imaging (SWI), MR angiography (MRA), and MR venography (MRV) provide additional prognostic information but are underutilised in standardised evaluation models.[11–14] Previous studies have highlighted the regional vulnerability of brain tissues and the possibility of imaging-based outcome prediction.[15–19] Still, no complete MRI severity assessment system incorporating these sequences has been devised, particularly in Indian clinical settings.
Materials and Methods
This was prospective observational research that lasted one year, from December 2023 to December 2024, in a multifunctional tertiary care centre. Based on consecutive sampling methods, a total of 43 individuals with clinical suspicion of hypoxic-ischaemic encephalopathy (HIE) were included. Adult patients over the age of 18 who had clinical or imaging symptoms suggesting acute global hypoxic-ischaemic brain damage were included. Exclusion criteria involved age less than 18 years, patients with motion artefacts, metallic implants such as pacemakers or cochlear implants, and intracranial clips that rendered MRI technically infeasible. The major goals were to assess MRI patterns and link imaging severity levels to clinical outcomes. The secondary goal was to evaluate the prognostic significance of various MRI sequences, including ASL, SWI, MRA, and MRV.
The Institutional Ethics Committee accepted the study (Approval Number: AMH-DNB-076/12–23). Prior to participation, patient attendants provided written informed consent. Patients had their MRI performed on a 3.0 Tesla scanner employing DWI, FLAIR, ASL, SWI, MRA, and MRV sequences. For DWI, a typically high b value of 1000 is used and the threshold value of <650 × 10–6 mm2/s is applied. Areas with low ADC below this threshold are considered hypoxic injured areas. For ASL hyperperfusion in adults, CBF ranges from >80 to 100 ml/100 gm/min in grey matter. For normal perfusion, the CBF ranges from 50 to 80 ml/100 gm/min in grey matter. For hypo perfusion, CBF falls <30 to 40 ml/100 gm/min in grey matter.[20] For SWI Deep Medullary Vein Grading (1–7 is used)[21]:G1: Absent veins, G2: Faint, equivocal signal, G3: Minimal, fine grey veins in deep white matter, G4: Mildly prominent, dark veins not reaching superficial layers, G5: Moderately prominent, dark, wide veins into superficial white matter, G6: Severely prominent, very dark veins near cortex, G7: Extremely prominent, thick, irregular veins reaching cortex. MRA finding[22] is scored based on normal visualisation of the intracranial artery and diffuse narrowing/non-visualisation of the intracranial artery. MRV finding[22] is scored based on normal visualisation of cerebral veins and diffuse narrowing/non-visualisation of cerebral veins. Based on the duration of the hypoxic event, patients exposed were categorised into three groups: mild (<5 mins), moderate (5–20 mins), and severe (>20 mins). Based on ejection fraction (EF) analysis, patients were categorised into four groups: EF > 55 normal, 45–54 mild left ventricular dysfunction, 35–44 moderate LV dysfunction, and <35 severe LV dysfunction. Clinical cerebral performance score[23] is categorised as normal living as cerebral performance category (CPC)-1, moderate disability with consciousness as CPC-2, severe disability with consciousness as CPC-3, coma patient as CPC-4, and dead as CPC-5. CPC-1 and -2 have favourable outcomes. CPC-3, -4, and -5 unfavourable outcomes. Identifying areas of the brain involved with DWI and FLAIR, as well as changes in ASL, SWI, MRA, and MRV sequences and assigning a score of 1 to each, with the exception of ASL hypoperfusion and bilateral medial occipital lobe hyperperfusion, which will be given a maximum score of 2. Finally, a total imaging severity score out of 18 will be determined. At the end of three months, clinical results were analysed using the CPC scale, which classified them as favourable (CPC-1 and -2) or unfavourable (CPC-3 and -5).
Statistical Analysis
The statistical analysis was performed with SPSS v28.0. Descriptive statistics were represented as frequencies and percentages. Associations were determined using the chi-square or Fisher’s exact test, with a P value of <.05 considered significant.
Results
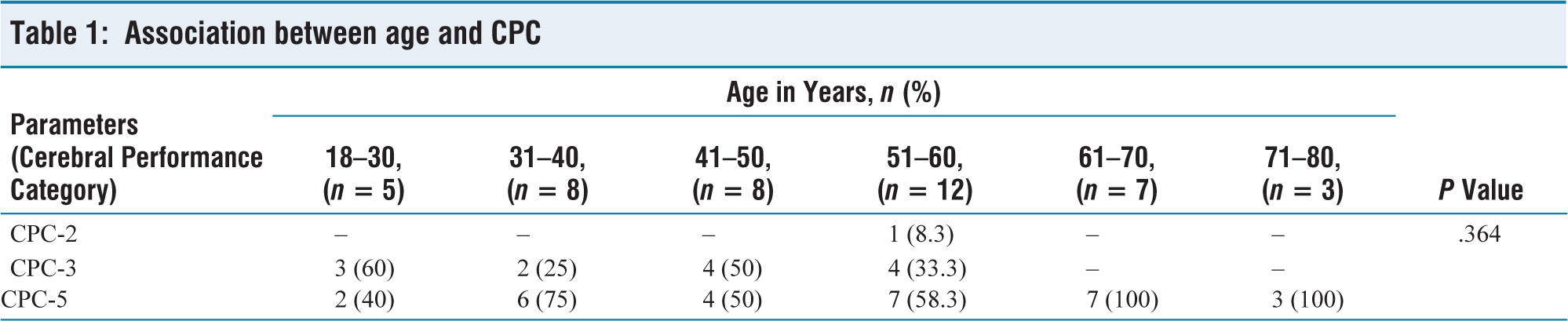
The study included 43 adult patients who had sustained acute global hypoxic-ischaemic brain damage. The prevalence was highest in the 51–60 age group (27.9%), followed by the 31–50 years. Clinical outcomes were measured using the CPC scale. Among patients above the age of 60, all got CPC-5 (death). Younger patients (18–30 years old) had a combination of CPC-3 (severe disability) and CPC-5 results. However, no statistically significant relationship was found between age and outcome (P = .364) [Table 1]. Similarly, there was no significant difference in outcomes by gender (P = .698), with 69% of males and 64.3% of females expressing CPC-5 [Table 2]. The duration of the hypoxic incident was significantly associated with patient outcome (P < .001) [Table 3]. All patients who experienced acute hypoxia for more than 20 minutes developed CPC-5. Patients with brief hypoxia (<5 minutes) had better outcomes, with 91.7% having CPC-3 and one patient reaching CPC-2 (mild impairment).
Association between age and CPC
Association between gender and CPC

Association between duration of hypoxic event and CPC

Patients with normal EF experienced mixed outcomes (CPC-2: 4.2%, CPC-3: 33.3%, CPC-5: 62.5%), while those with moderate or severe left ventricular dysfunction (EF <45%) had 100% CPC-5 results. However, the connection was not statistically significant (P = .565). Similarly, patients with severe Glasgow Coma Scale (GCS) scores had poorer outcomes, but this was not statistically significant (P = .122). Diabetes, hypertension, renal failure, sepsis, and cardiac impairment were among the most common comorbidities, but none had a statistically significant connection with outcome. Comorbidities, such as renal failure and sepsis, were more frequently linked to CPC-5.
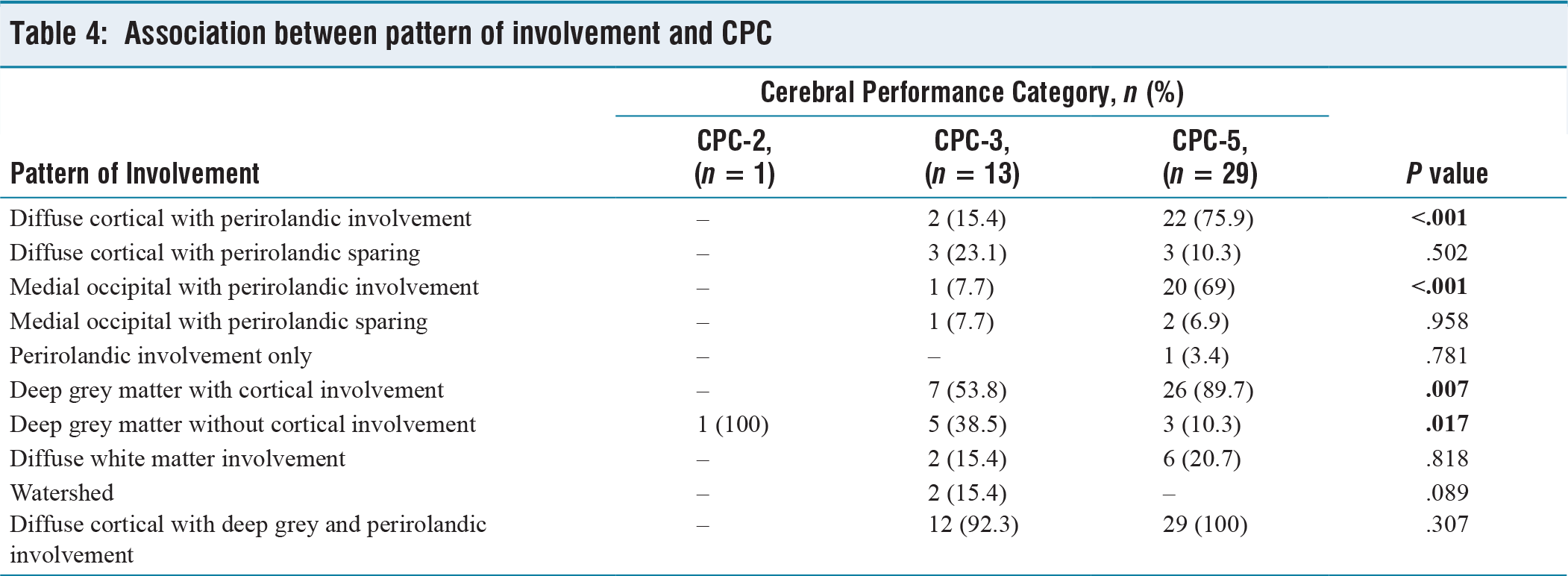
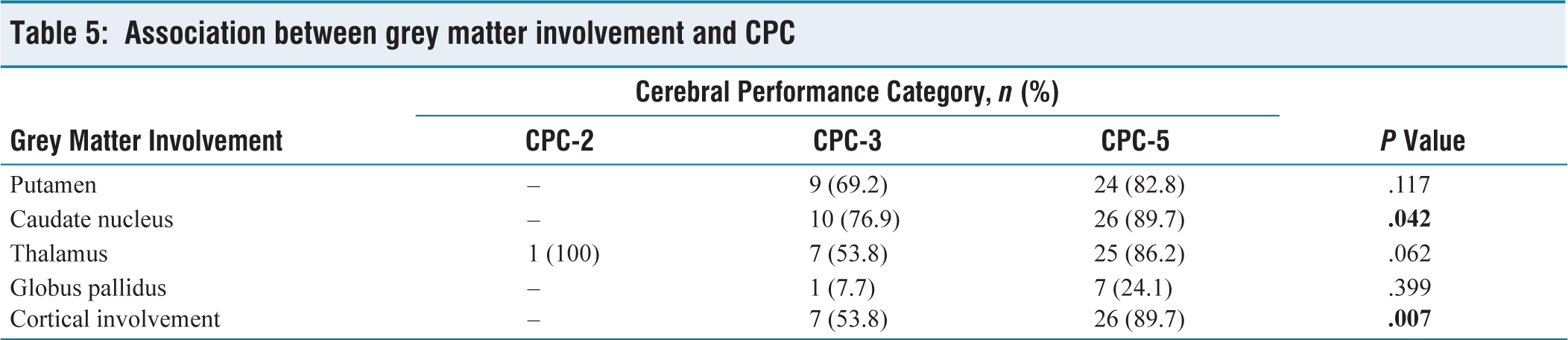
The most common pattern on MRI was widespread cortical involvement with deep grey matter and perirolandic region, which was observed in 97.7% of patients [Table 4]. This pattern demonstrated a substantial trend towards bad outcomes. Significant P value was found with cortical with perirolandic involvement (P = .001), medial occipital with perirolandic involvement (P < .001) and deep grey matter with cortical involvement (P = .007), only deep grey matter involvement (P = .017). Only peri-rolandic involvement, watershed pattern and diffuse white matter involvement were less commonly seen and are linked with unfavourable outcomes (CPC-3 and -5). In grey matter involvement, the caudate nucleus (P = .042) and cortical structures (P = .007) were substantially related to poor clinical outcomes [Table 5]. The involvement of the hippocampus, brainstem, and cerebellum demonstrated a trend towards worse outcomes, with cerebellar involvement reaching statistical significance (P = .018) [Table 6].
Association between pattern of involvement and CPC
Association between grey matter involvement and CPC
Association between parts of brain involvement and CPC

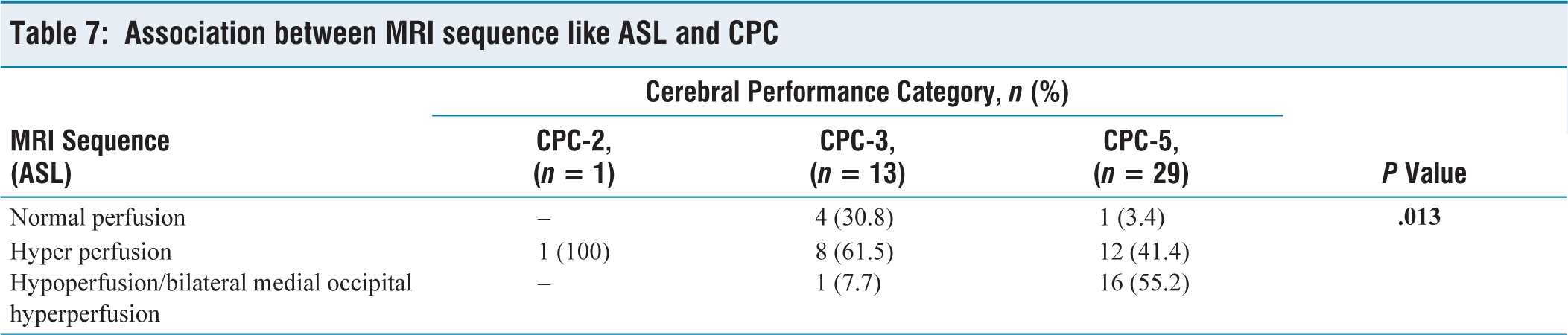
ASL is one of the most revealing advanced MRI sequences. Patients with diffuse hypoperfusion or bilateral medial occipital lobe hyperperfusion had significantly higher rates of CPC-5 outcomes (P = .013) [Table 7]. Similarly, SWI data revealed that patients with prominent deep medullary veins (Grades 5–7) had a significantly greater risk of CPC-5 outcomes (P = .043) [Table 8]. MRA and MRV revealed vascular constriction or non-visualisation of intracranial vessels in a small number of individuals, all of whom had CPC-5. However, these findings were not statistically significant (P = .255).
Association between MRI sequence like ASL and CPC
Association between MRI sequence like SWI and CPC
Finally, the MRI severity score, which was determined based on pattern, region involvement, and advanced sequence in MRI, revealed a clear trend that higher scores were associated with worse clinical outcomes [Table 9].
Association between imaging severity score and CPC
Discussion
This prospective observational study investigated the prognostic efficacy of MRI patterns and imaging severity scores in individuals with acute global HIE. These findings demonstrate the importance of neuroimaging in predicting clinical outcomes. Our study found that the majority of patients had poor neurological outcomes (CPC-5), particularly those who had been exposed to hypoxia for more than 20 minutes. This is consistent with the findings of Shuai Yang et al.,[19] who found unfavourable outcomes in individuals with severe hypoxic injury.
In our sample, the most common and prognostically unfavourable pattern was widespread cortical involvement with deep grey matter and perirolandic region, which was seen in 97.7% of patients. This complements Muttikkal et al.’s[16] findings, which found that broad cortical and deep grey matter involvement in DWI is frequently associated with poor clinical outcomes. However, unlike their findings, which showed that watershed patterns and isolated basal ganglia involvement had significantly better outcomes, our investigation found mixed results with similar patterns, most likely because of differences in sample size and patient profile.
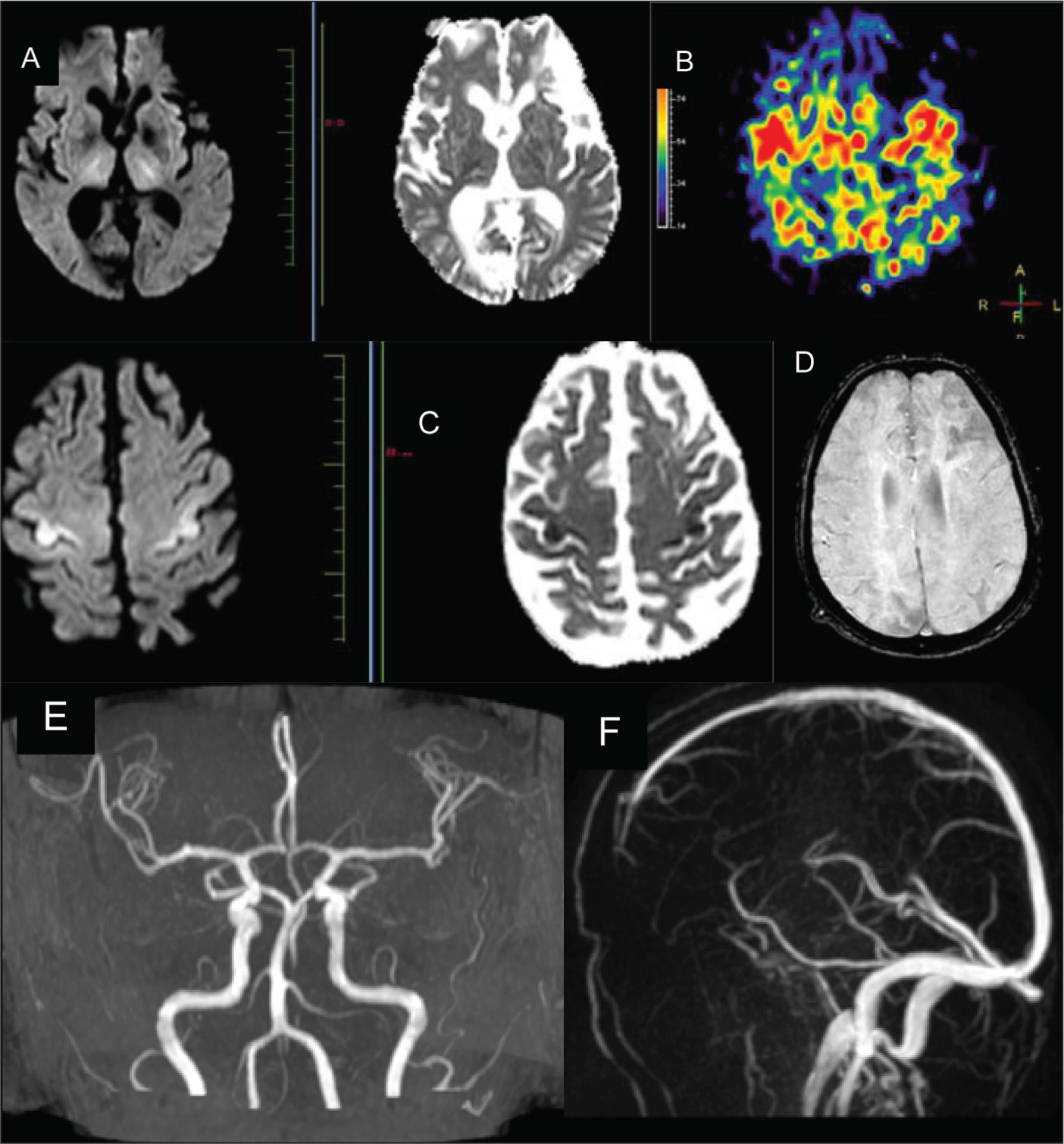
Our findings emphasised the significance of grey matter fragility. The involvement of the caudate nucleus and cortex was strongly related to a bad prognosis, which is consistent with Howard et al.,[24] who emphasised that the amount of cortical and deep grey matter injury has a significant impact on patient recovery capacity [Figure 1].
72/M had a moderate hypoxic episode with comorbidities DM, HT, CAD and CVA. (A and C) shows diffusion restriction in bilateral thalamus and perirolandic region; (B) Arterial spin labelling shows hyper perfusion in bilateral peri Rolandic region; (D) Susceptibility-weighted imaging shows no abnormal prominence of deep medullary veins; (E and F) shows normal MR angiography and venogram. The imaging severity score was 3. CPC was 5
Finally, Sandroni et al.[25] and Keijzer et al.[26] confirmed our observation that cortical and basal ganglia involvement correlates with poor recovery. Still, as seen in our study, isolated thalamic injury may indicate a better prognosis. While Barth et al.[27] claimed that the cortex was more frequently involved than the basal ganglia, we observed that the caudate nucleus was the most commonly affected. Nonetheless, both studies agree that significant structural involvement predicts poor results.
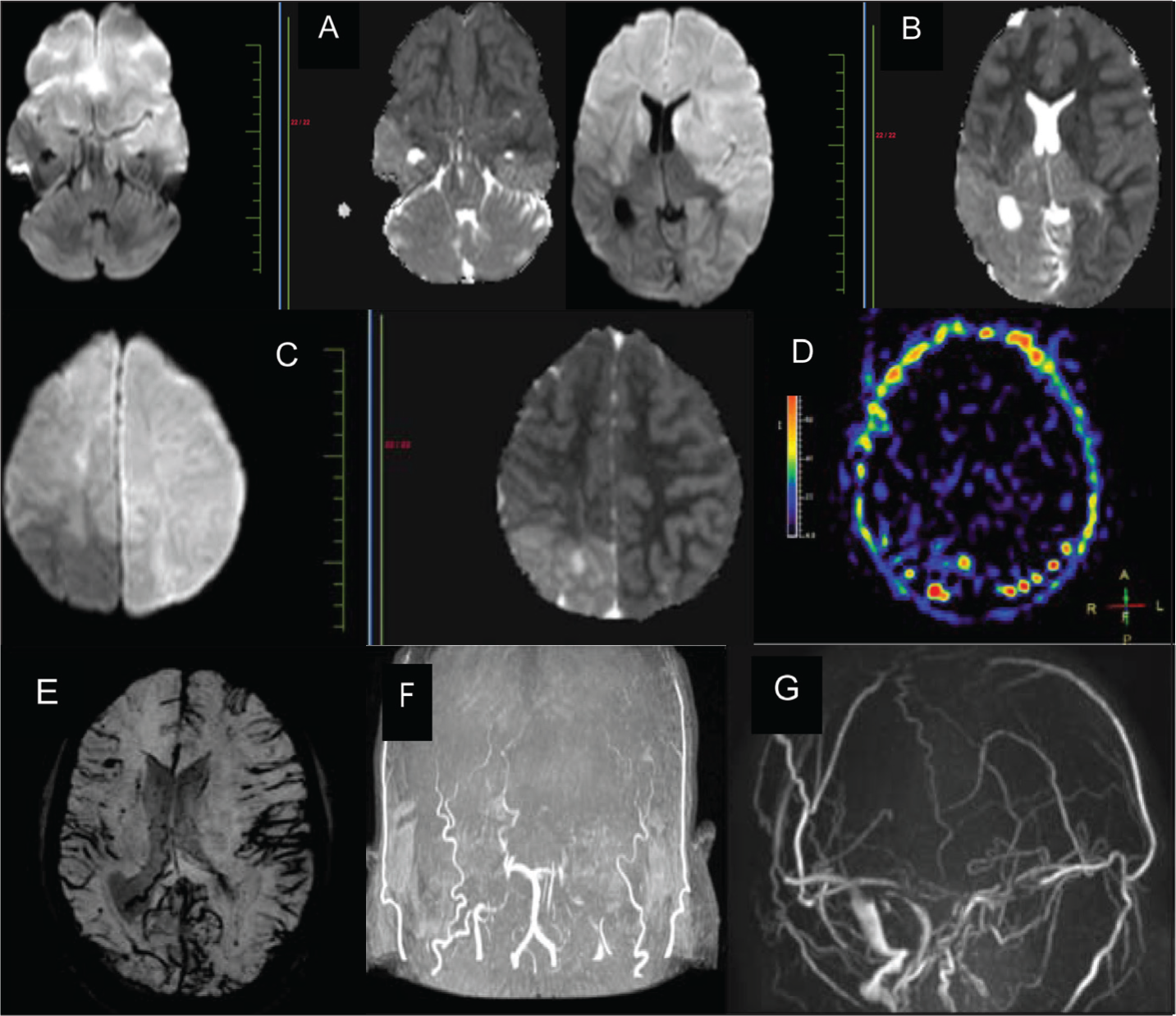
Our findings are comparable with those of Iten et al.,[28] who found that hippocampal, brainstem, and basal ganglia involvement predicts poor outcomes. However, their finding that pure cortical involvement predicts better outcomes contradicts our investigation, which found that even isolated cortical injuries were associated with a poor prognosis. Oren et al.[29] and An et al.[30] demonstrated that cortical and deep grey matter involvement, particularly when paired with white matter, brainstem, or cerebellum, is associated with a poor prognosis, which is consistent with our cohort [Figure 2]. This study makes an important addition by incorporating sophisticated MRI sequences to create an imaging severity ranking system.
39/M old male patient had a severe hypoxic episode with comorbidity of infective endocarditis. (A-C) shows diffusion restriction in bilateral caudate, putamen, globus pallidus, hippocampus, diffuse white matter, diffuse cortical, perirolandic region, left medial occipital lobe, Corpus callosum, right mid brain involvement; (D) diffuse hypo perfusion on arterial spin labelling; (E) Grade 5–7 prominent deep medullary vein on susceptibility-weighted imaging; (F) Non-visualisation of bilateral ICA, MCA, ACA on MR angiography; (G) Diffuse narrowing of Dural venous sinuses more predominantly seen on superior sagittal sinus seen on MR venogram. The imaging severity score was 15. CPC was 5
ASL perfusion imaging, particularly bilateral medial occipital hyperperfusion, was substantially linked with CPC-5 outcomes, consistent with the findings of De Havenon et al.,[31] who identified this pattern as a hallmark of permanent injury. Meng et al.[32] and Li et al.[33] discovered that areas with restricted diffusion on ADC frequently exhibit hyperperfusion on ASL, which we observed in 76.7% of patients, supporting the hypothesis of disrupted autoregulation in severely wounded regions. Similarly, SWI grading of deep medullary vein prominence has predictive value, as reported by Kitamura et al.,[21] in neonatal populations and is now validated in our adult group. Verma et al.[34] and Wagner et al.[35] observed pseudo-diminished cortical veins in diffusion restriction locations, which is consistent with our SWI findings, which show that higher medullary vein prominence is related to unfavourable outcomes. Oztoprak et al.[36] found a direct link between cerebral vein prominence and hypoxia severity.
Higher severity scores were strongly associated with poor outcomes, providing quantitative information for prognostication. This method addresses a gap in the literature, as previous research rarely incorporated numerous sequences into a single prognostic model. Unlike many previous retrospective studies that had heterogeneous populations or relied exclusively on DWI and ADC, our prospective strategy, which includes well-defined imaging and clinical characteristics, provides a more clinically useful tool. While several limitations remain, such as a small sample size (n = 43) and a lack of long-term follow-up beyond three months, multiple confounding factors taken into consideration and a lack of EEG and biochemical indicators (e.g., NSE, SSEP) in all patients hampered multi-modality prognostication. However, this study represents a new step towards standardised imaging-based prognostication in adult HIE.
Recommendations
Larger multi-centric trials with longer follow-up times are recommended to validate the suggested MRI severity assessment method. Further research should look at the role of automated AI-based picture analysis in determining the severity of a hypoxic injury.
Conclusion
This prospective study indicated that MRI, particularly when traditional sequences such as DWI and FLAIR are combined with advanced sequences such as ASL, SWI, MRA, and MRV, is an effective technique for determining the amount and pattern of acute global HIBI in adults. The most common pattern was widespread cortical involvement with deep grey matter and perirolandic areas, which was substantially related to poor clinical outcomes. A substantial connection was identified between higher MRI severity scores and unfavourable neurological outcomes (CPC-3 and -5), emphasising the usefulness of a composite scoring method. Diffuse cortical, diffuse cortical with deep grey matter, bilateral medial occipital lobe, peri-rolandic, diffuse white matter, brain stem, cerebellum and hippocampus involvement were predictors of poor outcome. Specific MRI findings, such as ASL diffuse hypoperfusion and bilateral medial lobe hyperperfusion, SWI Grade 5–7 medullary vein prominence, and non-visualisation of intracranial vessels in MRA and MRV, were strong predictors of poor prognosis. Thus, MRI severity rating may be a viable, non-invasive predictive tool for adult HIE patients in early decision-making.
Footnotes
Acknowledgements
I sincerely thank our chief, Dr Chidambaranathan N., Senior Consultant Radiologist. I am also very thankful to Dr Sunder K., Dr Vishaka Mazumdar, Dr Yvette Kirubha J., Dr Sudhakar, and Dr Amaresh for their valuable help and to all my colleagues and juniors for their continued support and encouragement.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Ethical approval was obtained from the Institutional Ethics Committee, Apollo Hospitals, Chennai. Approval number: AMH-DNB-076/12–23.
Informed consent
Informed consent has been obtained from all the patients who met the eligibility criteria.
Patient consent
Not obtained.
Credit author statement
Dr Mohamed Arief L. (MAL): Conceptualisation: Formulated the research goals and aims. Data Curation: Collected and organised clinical data. Investigation: Conducted investigations and data acquisition. Formal Analysis: Analysed data using relevant statistical and imaging methods. Methodology: Contributed to design of the study methodology. Visualisation: Prepared figures, MRI pattern illustrations, and data presentation. Writing – Original Draft: Drafted the initial manuscript.
Dr Meera Krishnakumar (MK): Conceptualisation: Contributed to development of study concept and design. Supervision: Provided guidance and oversight throughout the project. Methodology: Reviewed and refined imaging and scoring protocol. Validation: Verified reproducibility and quality of data. Writing – Review & Editing: Critically reviewed and edited the manuscript.
Dr Aishwarya B. (AB): Supervision: Supported and monitored all stages of research. Investigation: Participated in patient selection and MRI assessments. Validation: Cross-verified scoring and imaging patterns. Project Administration: Coordinated departmental approvals and resources. Writing – Review & Editing: Reviewed and edited the manuscript for clarity.
All authors have read and approved the final version of the manuscript.
Data availability
Data presenting the study’s findings are available from the corresponding author.
Use of artificial intelligence
No generative artificial intelligence or AI-assisted tools were used in the writing, analysis, or figure generation for this manuscript.