
Abstract
Background:
Subclinical left ventricular diastolic dysfunction (LVDD) is an early cardiac manifestation in individuals with prediabetes, often preceding symptomatic heart failure with preserved ejection fraction (HFpEF). Despite preserved ejection fraction and absence of hypertension, insulin resistance in prediabetes may contribute to myocardial remodelling and impaired relaxation.
Objective:
The aim of this study was to assess the prevalence of subclinical LVDD in normotensive prediabetic individuals and evaluate the association between diastolic dysfunction and insulin resistance measured by homeostasis model assessment of insulin resistance (HOMA-IR).
Methods:
This prospective observational study enrolled 53 normotensive adults (aged 18–60 years) with prediabetes, defined according to American Diabetes Association 2019 criteria. All participants underwent two-dimensional echocardiography with tissue Doppler imaging to assess LVDD. Insulin resistance was quantified using the HOMA-IR. LVDD was diagnosed based on abnormal Early-to-late mitral inflow velocity ratio (E/A) ratio and deceleration time (DT) per modified Tschope criteria.
Results:
LVDD was identified in 11 of 53 patients (20.8%). Patients with LVDD had significantly higher HOMA-IR values (4.78 ± 1.1) compared to those without LVDD (2.9 ± 0.85, P < .001). All individuals with LVDD were insulin resistant (HOMA-IR ≥ 2.5), whereas only 33.3% of those without LVDD showed insulin resistance. Pearson correlation analysis revealed a strong positive correlation between HOMA-IR and E/A ratio (r = 0.65, P < .01) and a moderate inverse correlation with DT (r = –0.58, P < .05).
Conclusion:
A considerable proportion of normotensive prediabetic individuals exhibits subclinical LVDD, which is strongly associated with insulin resistance. The HOMA-IR may serve as a valuable non-invasive marker for early myocardial dysfunction in prediabetes, potentially enabling risk stratification and early preventive strategies before the onset of overt heart failure.
Keywords
Introduction
Cardiovascular disease remains the leading cause of morbidity and mortality globally, with metabolic disorders such as type 2 diabetes mellitus (T2DM) playing a central role in its pathogenesis. However, it is now well recognised that adverse cardiovascular changes begin much earlier, during the prediabetic phase, even in the absence of overt hyperglycaemia or hypertension.[1,2] Prediabetes—defined by impaired fasting glucose (IFG), impaired glucose tolerance (IGT), or elevated haemoglobin A1c (HbA1c) (5.7–6.4%)—affects nearly 25–38% of the adult population worldwide and is associated with a markedly increased risk of cardiovascular events.[3,4]
One of the earliest cardiac manifestations in this metabolic continuum is left ventricular diastolic dysfunction (LVDD)—characterised by impaired myocardial relaxation and increased ventricular stiffness despite preserved ejection fraction. LVDD may remain clinically silent for years, but it contributes significantly to the later development of heart failure with preserved ejection fraction (HFpEF).[5,6] Studies using advanced imaging techniques such as tissue Doppler imaging (TDI) and speckle-tracking echocardiography (STE) have demonstrated subclinical myocardial abnormalities even in normotensive individuals with prediabetes.[7,8]
A central mechanism implicated in the pathogenesis of LVDD is insulin resistance, a hallmark of prediabetes. Insulin resistance promotes myocardial fibrosis, endothelial dysfunction, altered calcium homeostasis and oxidative stress—all of which impair myocardial compliance and relaxation.[9,10] The homeostasis model assessment of insulin resistance (HOMA-IR) is a validated and widely used surrogate marker to quantify insulin resistance in clinical and epidemiological studies.[11]
While prior studies have examined the association between hyperglycaemia and LV function in diabetes, limited data are available specifically focusing on normotensive individuals in the prediabetic state, especially with regard to the predictive utility of the HOMA-IR. Furthermore, most existing studies have not adequately excluded confounding factors such as hypertension, renal dysfunction or overt cardiac disease, nor have they incorporated structured echocardiographic criteria for early LVDD detection.[12,13]
In this context, our study aims to investigate the prevalence of subclinical LVDD in normotensive prediabetic individuals and to evaluate the predictive role of insulin resistance (HOMA-IR) in identifying those at risk. By focusing on a younger, asymptomatic cohort without comorbidities, we aim to provide insight into early myocardial changes driven primarily by metabolic dysfunction, thereby informing future screening and prevention strategies.
Aims and Objectives
Aim
The aim of this study was to evaluate the prevalence of subclinical LVDD in normotensive prediabetic individuals and examine the predictive role of insulin resistance, assessed by the HOMA-IR.
Objectives
Following are the objectives of this study:
To determine the incidence of subclinical LV diastolic dysfunction in normotensive prediabetic individuals using 2D echocardiography and TDI. To evaluate insulin resistance using the HOMA-IR in this population. To examine the association between HOMA-IR and echocardiographic indicators of diastolic dysfunction. To assess the relationship between glycaemic control (HbA1c) and the presence of LVDD. To identify insulin resistance (HOMA-IR) as an early predictor of myocardial diastolic dysfunction in asymptomatic normotensive prediabetic adults.
Materials and Methods
Study Design and Setting
This was a prospective observational study conducted from September 2019 to December 2020 in the Departments of Endocrinology and Cardiology at Indraprastha Apollo Hospital, New Delhi, a tertiary care referral centre.
Ethical Approval
The study protocol was reviewed and approved by the Institutional Ethics Committee (Approval No.: IAEC/2020/12; Date: September 1, 2019). Written informed consent was obtained from all participants in accordance with the principles outlined in the Declaration of Helsinki. Trial registration was not applicable for this prospective observational study, as no interventions were administered, and the study did not fall under mandatory registration criteria.
Study Population
Inclusion Criteria
Age between 18 and 60 years
Diagnosis of prediabetes, based on American Diabetes Association (ADA) 2019 criteria:
Fasting plasma glucose: 100–125 mg/dL 2-hour post-glucose load (OGTT): 140–199 mg/dL HbA1c: 5.7–6.4%
Normotensive individuals: Systolic blood pressure (BP) <130 mmHg and diastolic BP <85 mm Hg
No prior history of structural heart disease
Exclusion Criteria
Known hypertension, coronary artery disease, valvular heart disease or arrhythmia
Chronic kidney disease (estimated glomerular filtration [eGFR] <60 mL/min/1.73 m²)
Chronic obstructive pulmonary disease (COPD), pregnancy or acute systemic illness
Incomplete data or refusal to provide informed consent
Sample Size Calculation
Assuming an expected prevalence of LVDD in prediabetic individuals of 16.7%, as per the study by Tschope et al.,[3] with a 95% confidence interval and a 10% margin of error, the required sample size was calculated using the formula:
Formula for calculating the sample size -
n = z2 x p(1-p)/e2 Where, n is sample size, z is the z score, e is the margin of error, p is the population proportion n = (1.96*1.96) x (0.167*(1–0.167))/(0.1*0.1) = 53
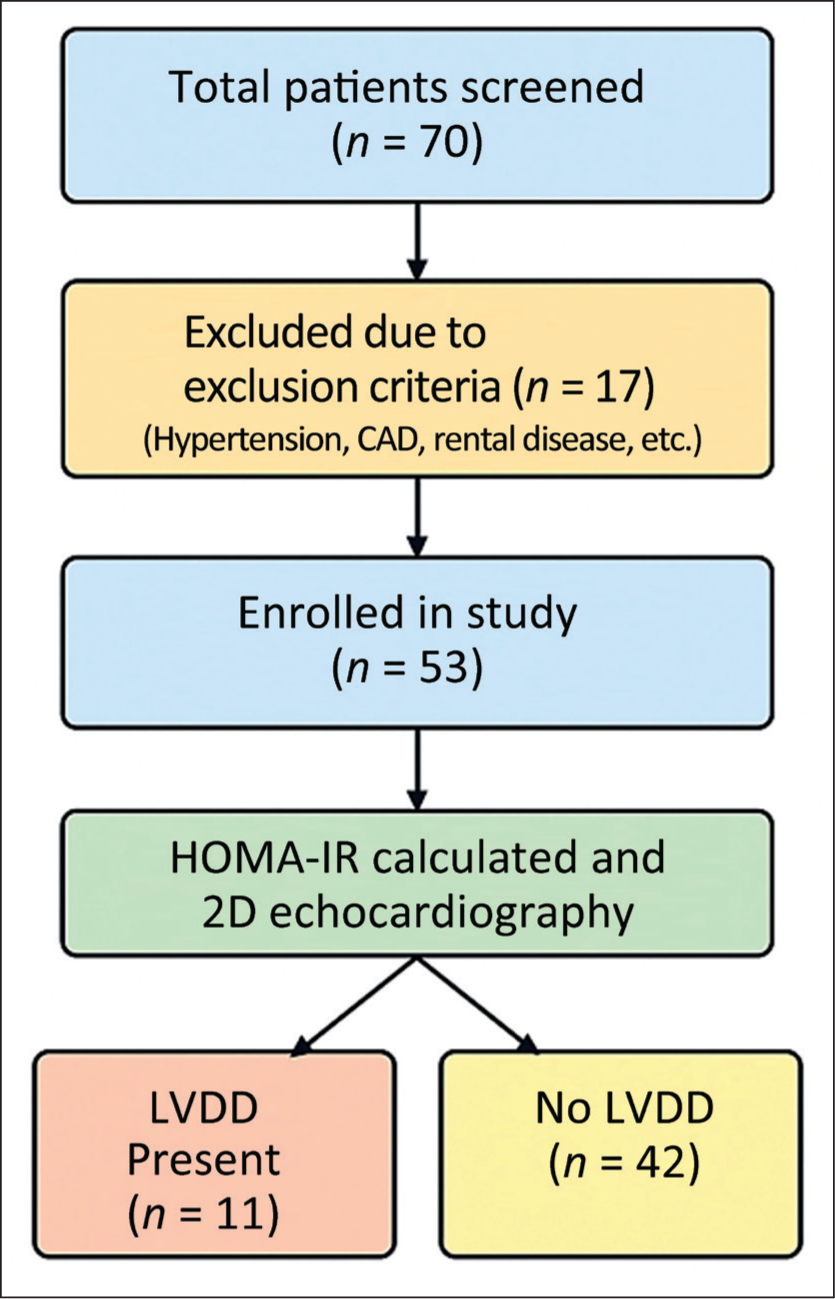
The minimum required sample size was 53 participants, which was achieved. The flow of participant screening and inclusion is shown in Figure 1.
Flow diagram showing screening and inclusion of prediabetic participants. LVDD: Left ventricular diastolic dysfunction; HOMA-IR: Homeostatic model assessment of insulin resistance
Data Collection and Investigations
Clinical and Anthropometric Parameters
Height, weight, body mass index (BMI) and waist circumference
Blood pressure was measured using a validated digital sphygmomanometer after 5 minutes of rest
Biochemical Parameters
Fasting plasma glucose (FPG)
Two-hour plasma glucose (post-OGTT)
HbA1c, measured by high-performance liquid chromatography (HPLC)
Fasting serum insulin, measured by chemiluminescence immunoassay (CLIA)
Insulin resistance was assessed using the HOMA-IR, calculated as:
HOMA IR = (fasting insulin mU/mL X fasting glucose mmol/L) / 22.5 A HOMA-IR > 2.5 was considered indicative of insulin resistance.
Echocardiographic Assessment
All participants underwent 2D transthoracic echocardiography and TDI performed by an experienced cardiologist blinded to laboratory data. The following parameters were recorded:
Mitral inflow velocities (E and A waves) Early-to-late mitral inflow velocity ratio (E/A) ratio Deceleration time (DT) of early mitral inflow Left atrial (LA) volume Systolic pulmonary artery pressure (sPAP) E/e′ ratio (early mitral inflow velocity to mitral annular early diastolic velocity)
Definition of LV Diastolic Dysfunction (LVDD):
LVDD was diagnosed based on either an abnormal E/A ratio (<0.75 or >1.5) or a DT <150 ms or >220 ms, in accordance with the criteria established by Tschope et al.
Participants meeting either of the above thresholds were classified as having LVDD.
Statistical Analysis
All data were analysed using IBM SPSS Statistics for Windows, Version 19.0.
Continuous variables: presented as mean ± standard deviation (SD)
Categorical variables: expressed as frequencies and percentages
Between-group comparisons:
Independent t-test for continuous variables Chi-squared test for categorical variables
Correlation analysis between HOMA-IR and echocardiographic parameters was performed using Pearson correlation coefficient
A P value < .05 was considered statistically significant
Results
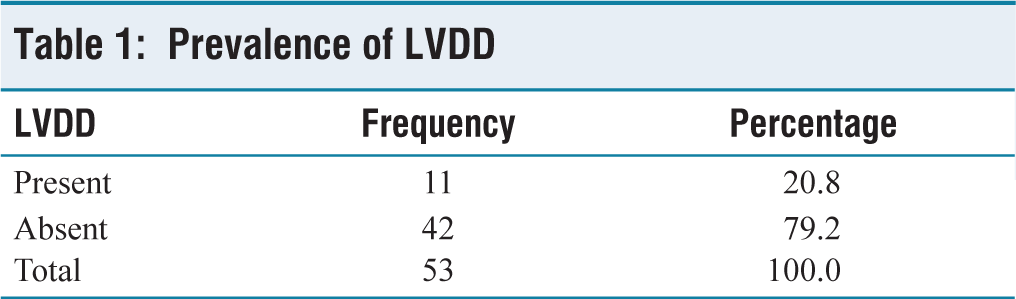
A total of 53 normotensive prediabetic individuals were included in the study. The mean age of the participants was 45.7 ± 9.8 years, and 56.6% were male. Based on echocardiographic criteria, 11 individuals (20.8%) were diagnosed with LVDD, while the remaining 42 (79.2%) did not exhibit evidence of LVDD [Table 1 and Figure 2].
Prevalence of LVDD
Bar graph illustrating the distribution of study participants with and without LVDD
A total of 53 patients with prediabetes were enrolled in the present study. Out of 53 cases of prediabetes, LVDD was present among 11 (20.8%) cases.
Demographic and Biochemical Characteristics
The mean age in the LVDD group was significantly higher (53.18 ± 6.40 years) compared to the non-LVDD group (43.76 ± 10.34 years, P = .035). There was no statistically significant difference in gender distribution between the two groups.
HbA1c levels, reflecting chronic glycaemic exposure, were significantly elevated in the LVDD group (6.21 ± 0.23%) compared to the non-LVDD group (5.84 ± 0.33%, P = .01).
Insulin Resistance (HOMA-IR) Findings
HOMA-IR values were significantly higher among individuals with LVDD compared to those without:
LVDD group: 4.78 ± 1.1 Non-LVDD group: 2.9 ± 0.85 (P <.001)
Moreover, 100% (11/11) of participants with LVDD were insulin resistant (HOMA-IR > 2.5), whereas only 33.3% (14/42) of those without LVDD met this criterion (P < .0001).
These results underscore the strong association between insulin resistance and the presence of subclinical LVDD [Table 2 and Figure 3].
The prevalence of insulin resistance among prediabetic patients with and without LVDD
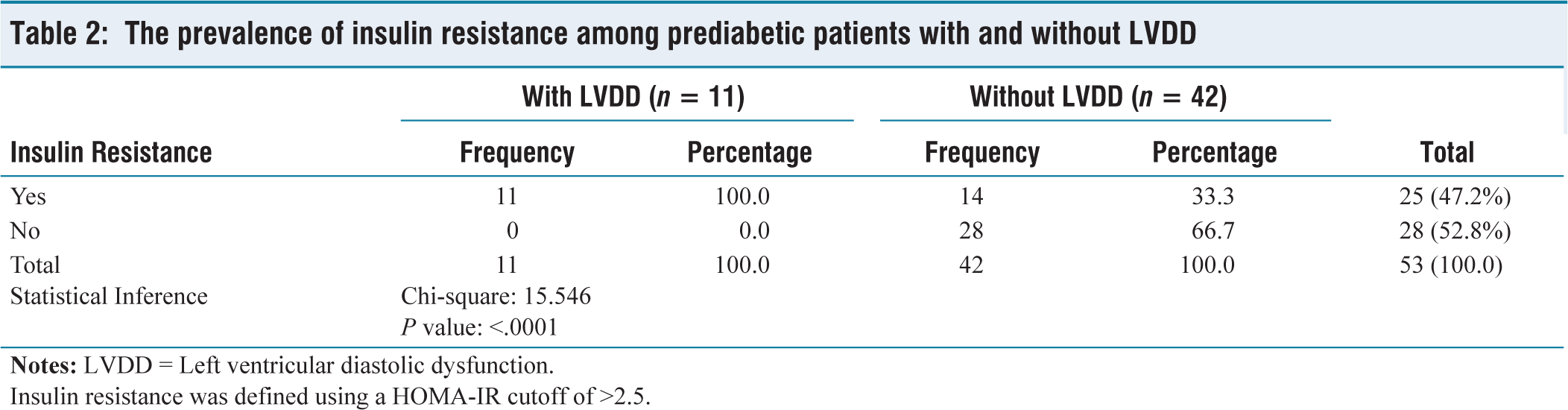
Insulin resistance was defined using a HOMA-IR cutoff of >2.5.
Bar chart showing the prevalence of insulin resistance (HOMA-IR >2.5) among normotensive prediabetic individuals.
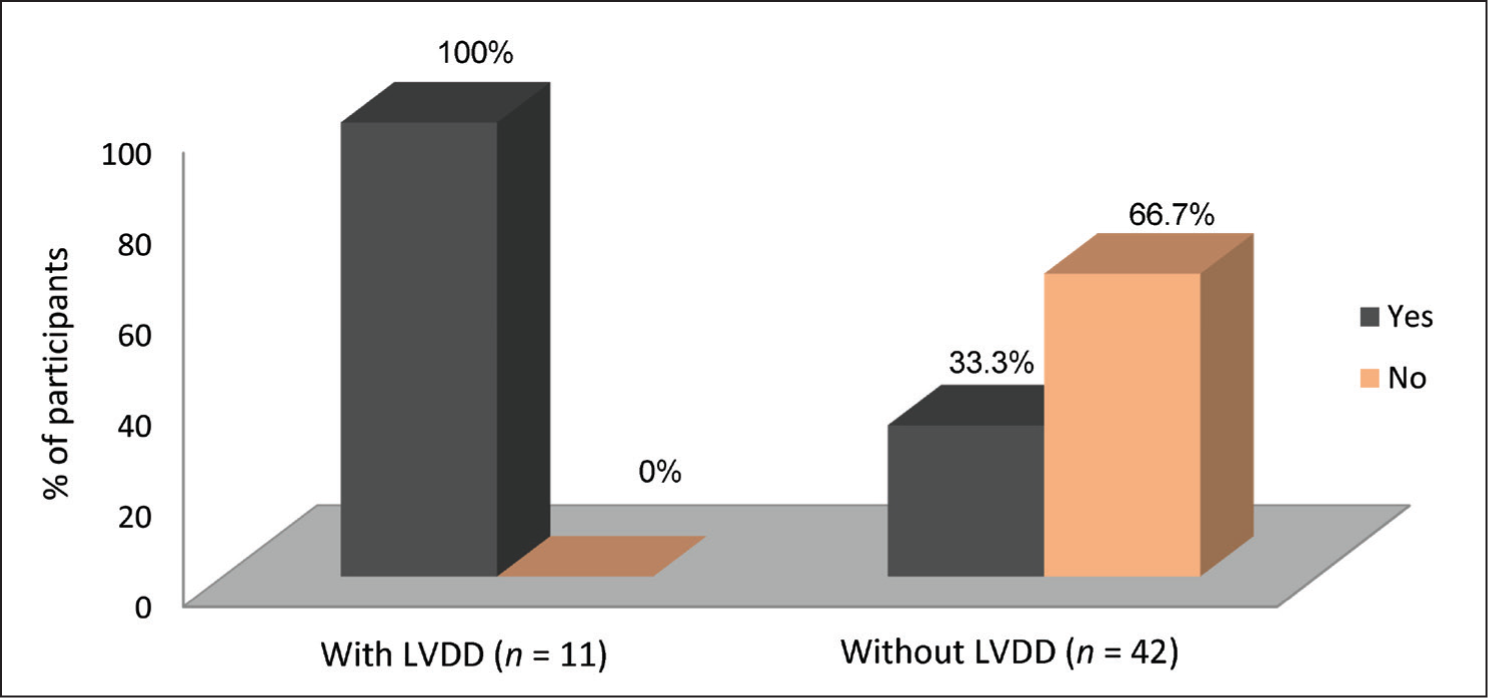
Table 2 presents the prevalence of insulin resistance among prediabetic patients with and without LVDD. Insulin resistance, defined using a HOMA-IR threshold >2.5 (see Table 2 footnote), was present in 100% of patients with LVDD, compared to only 33.3% of those without LVDD (P value = <.0001). This reinforces the potential role of insulin resistance in early myocardial remodelling.
Echocardiographic Parameters
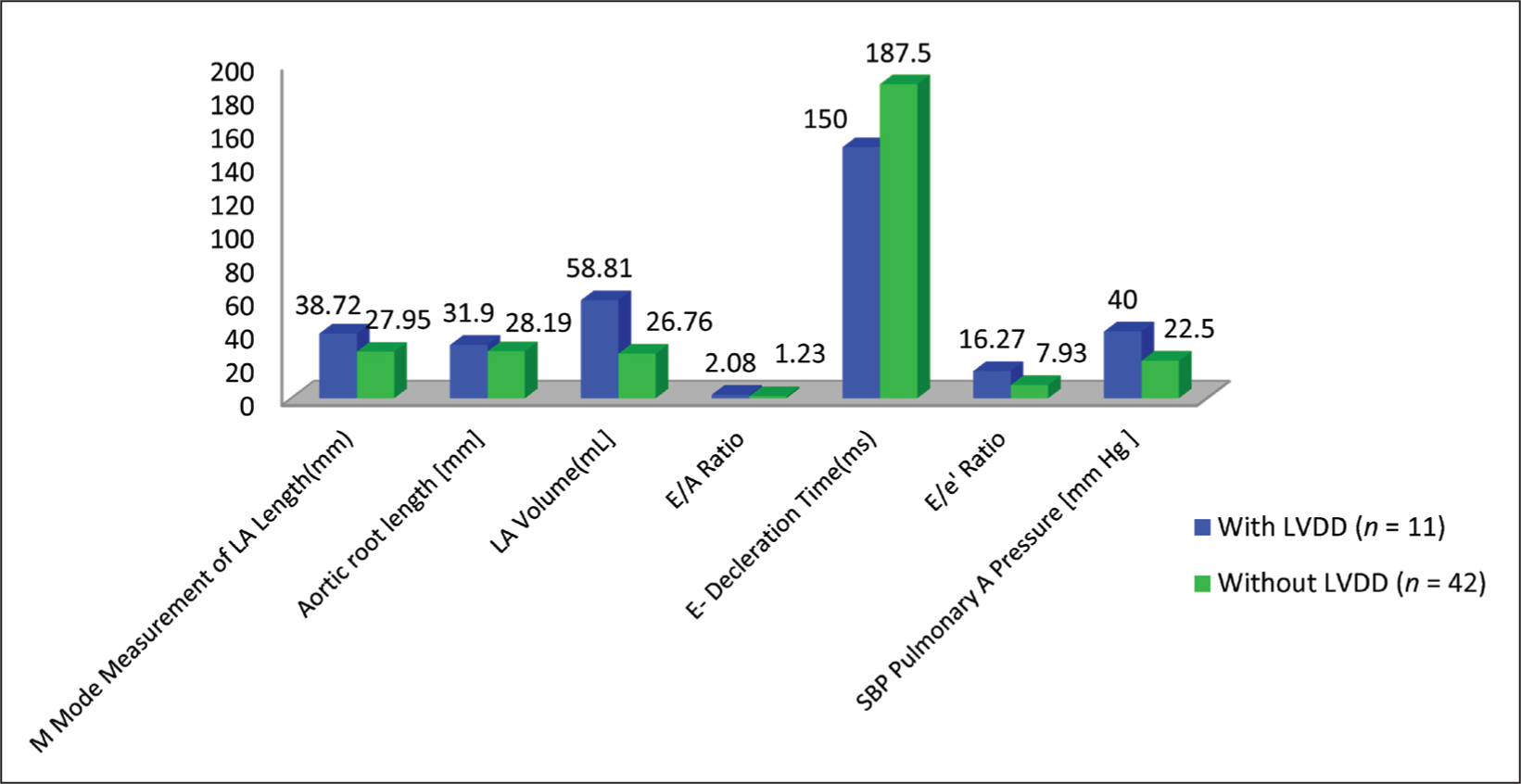
Echocardiographic findings showed significant diastolic abnormalities among the LVDD group:
E/A ratio:
LVDD group: 2.08 ± 0.43 Non-LVDD group: 1.23 ± 0.18 (P < .001) DT:
LVDD group: 150 ± 21.4 ms Non-LVDD group: 187 ± 5.3 ms (P <.001) LA volume:
LVDD group: 58.8 ± 5.5 mL Non-LVDD group: 26.7 ± 3.4 mL (P = .006) sPAP:
LVDD group: 40.0 ± 5.2 mmHg Non-LVDD group: 22.5 ± 2.5 mmHg (P <.001)
Other echocardiographic measures (e.g. E/e′ ratio, aortic root diameter, LA length) were not significantly different between the groups [Table 3 and Figure 4].
The comparison of echocardiographic parameters between patients with and without LVDD
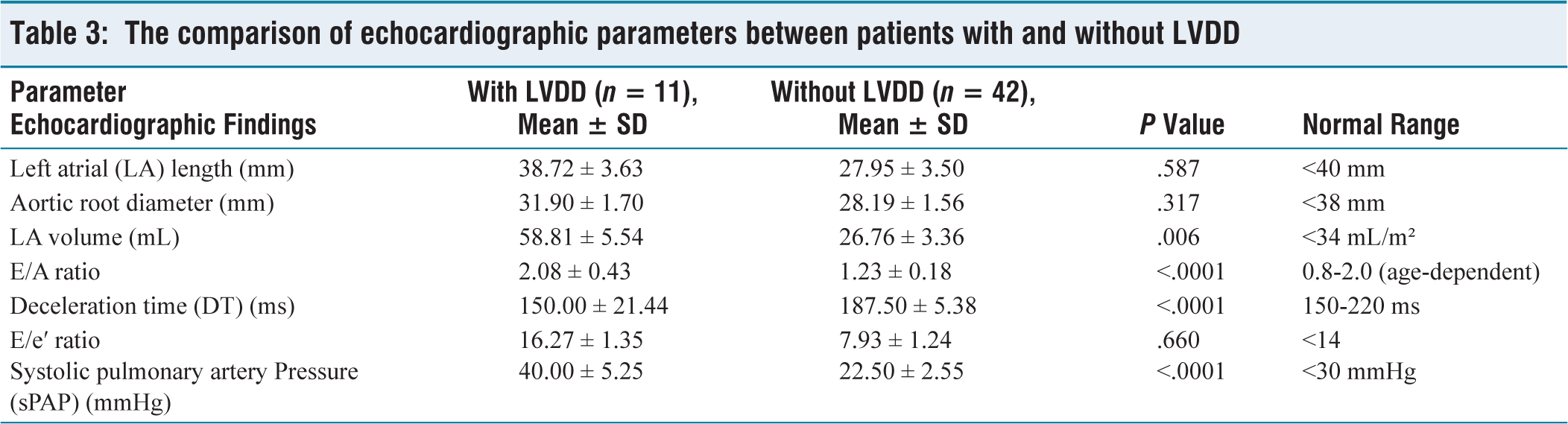
LA: Left atrium; DT: Deceleration time; sPAP: Systolic pulmonary artery pressure; LVDD: Left ventricular diastolic dysfunction
Patients with LVDD had significantly higher LA volumes (mean 58.8 ± 5 vs. 26.7 ± 3.4 mL), exceeding the normal reference range of <34 mL/m², which reflects elevated left-sided filling pressures. Similarly, sPAP in the LVDD group averaged 40.0 ± 5.2 mmHg, markedly above the normal threshold of <30 mmHg, suggesting early pulmonary hypertension, as also noted in Table 3.
Notes: LVDD = Left ventricular diastolic dysfunction, LA = Left atrium, DT = Deceleration time, sPAP = Systolic pulmonary artery pressure, E/A = Early-to-late mitral inflow velocity ratio, E/e′ = Mitral inflow to annular early diastolic velocity ratio normal ranges adapted from American Society of Echocardiography (ASE) 2023 guidelines and standard echocardiographic references. LVDD was defined as either E/A ratio <0.75 or >1.5, or DT <150 ms or >220 ms, per modified Tschope criteria.
Correlation Analysis
Pearson correlation analysis revealed:
Scatter plot demonstrating a significant positive correlation between insulin resistance (measured by HOMA-IR) and E/A ratio among normotensive prediabetic individuals (r = 0.65, P < .01). Each point represents an individual subject. The dashed line indicates the line of best fit
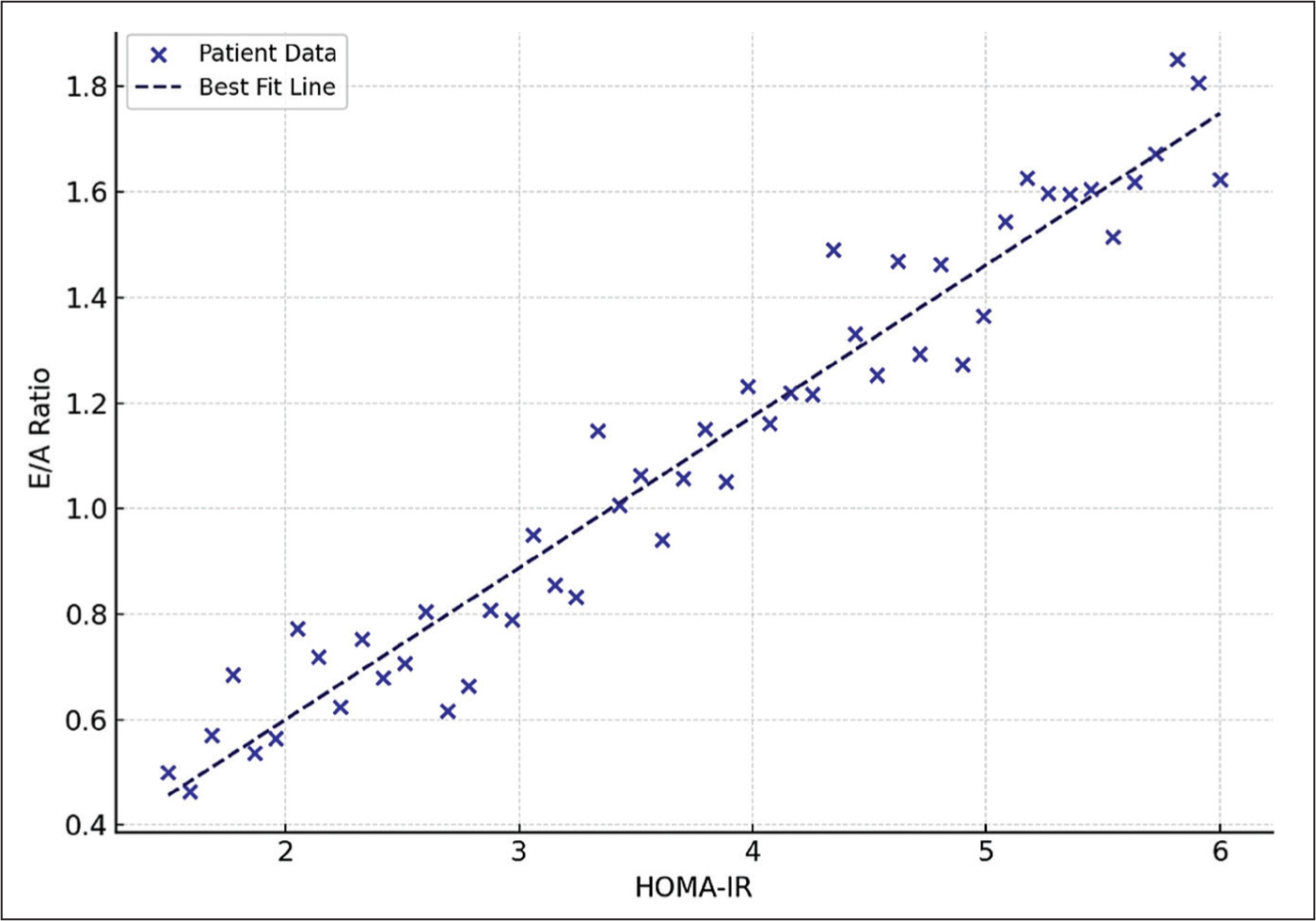
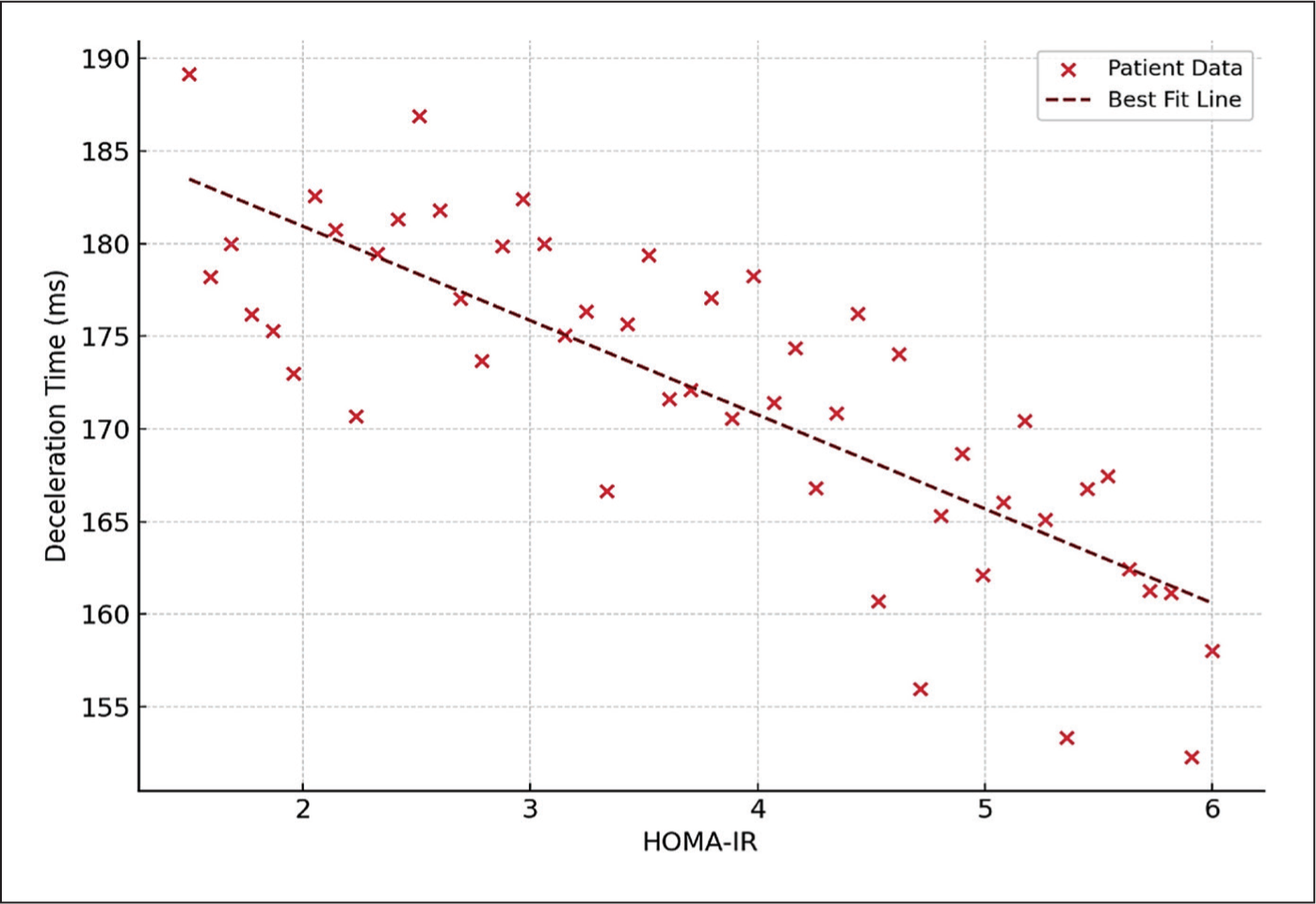
These findings confirm that increased insulin resistance is significantly associated with worsening diastolic function in this population.
Discussion
This prospective observational study demonstrates that a significant proportion (20.8%) of normotensive prediabetic individuals exhibit subclinical LVDD. Crucially, our findings identify insulin resistance—measured by the HOMA-IR—as a strong and independent predictor of LVDD, even in the absence of overt diabetes, hypertension or clinically apparent cardiovascular disease.
Our observed prevalence aligns with previous reports, including those by Sirkeci et al. and Albertini et al., who noted early echocardiographic signs of diastolic dysfunction in prediabetic populations.[14,15] However, our study adds to the literature by explicitly focusing on HOMA-IR as a primary metabolic predictor and correlating it robustly with echocardiographic parameters of LVDD.
In our cohort, 100% of participants with LVDD were insulin resistant, while only 33.3% of those without LVDD showed elevated HOMA-IR, suggesting a compelling link between metabolic dysregulation and early myocardial dysfunction. This finding supports mechanistic models proposed by Buglioni and Burnett[10] and later expanded by Tschope and Van Linthout, who proposed that insulin resistance mediates myocardial remodelling via microvascular inflammation, myocardial fibrosis, impaired nitric oxide signalling and oxidative stress.[16,17]
Recent studies have reinforced this pathophysiological link. For example, Mita et al. showed that higher HOMA-IR values were independently associated with diastolic dysfunction among Japanese patients with T2DM.[12] More recently, Zhang et al. used STE to detect subclinical myocardial strain abnormalities in prediabetic individuals and reported a significant correlation with insulin resistance indices.[13] Similarly, Rodrigues et al. employed three-dimensional echocardiography and found early diastolic abnormalities linked to HOMA-IR in asymptomatic prediabetics.[18]
Recent studies support this preventive perspective. For instance, Singh et al. demonstrated that lifestyle interventions in Indian prediabetic adults improved both insulin sensitivity and early echocardiographic markers of cardiac dysfunction.[19] Furthermore, Lorenzo-Almorós et al. proposed that metabolic markers, including HOMA-IR and adiponectin, may be integrated into predictive models for HFpEF in high-risk individuals.[9]
In our study, individuals with elevated HOMA-IR exhibited classical diastolic changes—reduced E/A ratio, shortened DT, increased LA volume and elevated sPAP—all indicative of increased LV filling pressure and impaired ventricular compliance. These findings are consistent with previous observations by Diamant et al., who demonstrated that insulin resistance alters myocardial metabolism and sympathetic tone, contributing to functional impairments.[20]
Importantly, we also found a significant positive correlation between HOMA-IR and E/A ratio (r = 0.65, P < .01) and a negative correlation with DT (r = –0.58, P < 0.05). These correlations suggest that HOMA-IR could serve as a surrogate marker for subclinical myocardial dysfunction. Comparable findings were reported in a study by Hayashi et al., which linked elevated fasting insulin levels with decreased LV compliance and worsening diastolic indices in prediabetic adults.[21]
From a clinical perspective, our results advocate for a paradigm shift in how prediabetes is managed. Rather than being viewed solely as a risk factor for future diabetes, prediabetes should be considered a metabolically active state with immediate cardiovascular implications.[22] Given that LVDD is a precursor to HFpEF, early identification of at-risk patients using HOMA-IR may enable timely intervention through lifestyle modification and pharmacotherapy, potentially altering the trajectory toward overt heart failure.[23]
The strengths of our study include a well-characterised normotensive cohort, exclusion of known cardiovascular disease and use of TDI, which enhance sensitivity for detecting early diastolic abnormalities. Unlike N-terminal pro–B-type natriuretic peptide (NT-proBNP), which is subject to variation with age, BMI and renal function, HOMA-IR offers a metabolically specific index of insulin resistance, better suited for early detection in prediabetic individuals.
our study provides strong evidence for incorporating HOMA-IR into routine cardiovascular risk screening for prediabetic patients, particularly those without overt cardiac symptoms.
Conclusion
This study underscores that insulin resistance, assessed through HOMA-IR, is a potent early marker of subclinical LVDD in normotensive prediabetic individuals. The strong correlation between elevated HOMA-IR and echocardiographic markers of LVDD supports the integration of metabolic risk screening into early cardiovascular risk stratification.
We advocate for the routine assessment of HOMA-IR in prediabetic patients to identify those at heightened risk of early cardiac dysfunction, even before overt diabetes or hypertension develops. Targeted metabolic interventions in this window may reduce long-term cardiovascular complications.
Clinical Implications
The findings of this study reinforce the concept that prediabetes is not merely a metabolic transition stage but an early cardiovascular risk state, particularly when accompanied by insulin resistance. The detection of subclinical LVDD in this asymptomatic population—independent of hypertension or overt cardiac disease—has important clinical consequences:
HOMA-IR should be considered a routine screening tool in prediabetic individuals to identify those at risk of early myocardial dysfunction. Echocardiographic evaluation, particularly with TDI, can detect subtle diastolic changes that may be missed by conventional clinical assessments. Early identification of LVDD through HOMA-IR and echocardiography offers an opportunity for preventive strategies—such as structured lifestyle interventions and insulin-sensitising therapies—to potentially reverse or halt progression toward HFpEF. By integrating metabolic and cardiac evaluation in prediabetic care, clinicians can shift the paradigm from reactive treatment to proactive cardiovascular risk mitigation.
These results advocate for a multidisciplinary approach—involving endocrinologists, cardiologists and primary care providers—to implement early surveillance and intervention strategies in normotensive prediabetic individuals with elevated insulin resistance.
Limitations
While this study provides novel insights into the role of insulin resistance in early cardiac dysfunction among prediabetics, several limitations should be acknowledged:
Single-centre study and sample size: This study was conducted at a single tertiary-care centre with a relatively small sample size (n = 53), which may limit generalisability. While powered for prevalence estimation, the sample may be insufficient for subgroup or multivariable analysis. Cross-sectional design: The observational design limits causal inference between insulin resistance (HOMA-IR) and LV diastolic dysfunction. Longitudinal studies are needed to determine predictive value and clinical progression. Absence of advanced imaging: Diastolic function was assessed using conventional and tissue Doppler echocardiography. More sensitive modalities like speckle-tracking or cardiac MRI could have offered deeper insight into subclinical myocardial changes. Unmeasured confounders: Factors such as physical activity, visceral adiposity, sleep apnoea and inflammatory markers were not assessed and may have influenced outcomes. No intervention or outcome data: The study did not assess the effect of improving insulin resistance on diastolic function or track long-term outcomes like HFpEF or progression to diabetes. Biomarker considerations: Although NT-proBNP was excluded from the current version of the analysis, prior observations and literature indicate that its diagnostic utility can be confounded by renal function, age and BMI. In contrast, HOMA-IR may offer more metabolically relevant and stable associations in the prediabetic setting, but still requires standardisation across populations and assay platform
Future research should involve multicentre, longitudinal studies incorporating metabolic, structural and functional cardiac parameters to validate and expand on these findings
Footnotes
Acknowledgements
I would like to express my deep gratitude to Dr. V. K. Aneja and Dr. S. K. Wangnoo, my research supervisors, for their patient guidance, enthusiastic encouragement and useful critiques of this research work. I also extend my thanks to Dr. P. K. Gosh for her advice and assistance. Special thanks to the statistician for help with data analysis and to the technicians in the internal medicine, cardiology and endocrinology departments for their support.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Approval No: IAEC/2020/12, dated September 1, 2019. Approval was obtained from the Institutional Ethics Committee of Indraprastha Apollo Hospital, New Delhi.
Informed consent
Informed consent was obtained from all participants before enrolment in the study.
Credit author statement
Ramesh Krishnan helped in conceptualisation, study design and manuscript writing.
Vijay Kumar Aneja was involved in data collection, statistical analysis and review.
Subhash Kumar Wangnoo helped in supervision, critical review and final approval.
Data availability
Data supporting the findings of this study are available upon reasonable request from the corresponding author.
Use of artificial intelligence
No AI tools were used in the preparation of this manuscript.