
Abstract
Background and Aims:
Prediabetes is increasingly recognised as a cardiovascular risk state, with emerging evidence suggesting early myocardial dysfunction, including left ventricular diastolic dysfunction (LVDD), even before overt diabetes. NT-proBNP is a promising biomarker for detecting subclinical cardiac involvement. This study aimed to assess the prevalence of LVDD in prediabetic patients and to correlate echocardiographic findings with NT-proBNP levels.
Methods:
This prospective observational study included 53 prediabetic individuals aged 18-60 years without hypertension or structural heart disease. LVDD was diagnosed using tissue Doppler echocardiographic criteria, including E/A ratio and deceleration time (DT). NT-proBNP levels were measured and compared between LVDD and non-LVDD groups.
Results:
LVDD was present in 11 of 53 participants (20.8%). Patients with LVDD had significantly higher NT-proBNP levels (195.01 ± 6.75 pg/mL) than those without LVDD (80.13 ± 13.81 pg/mL; P = .025). The mean age in the LVDD group was also significantly higher (P = .035). E/A ratio and DT were significantly altered in the LVDD group.
Conclusion:
LVDD is moderately prevalent in prediabetic individuals. NT-proBNP correlates well with echocardiographic evidence of diastolic dysfunction and may serve as a non-invasive marker for early detection of cardiac involvement in prediabetes. These findings support the utility of NT-proBNP as a screening tool for early cardiac dysfunction in prediabetic individuals.
Keywords
Introduction
Prediabetes is a high-risk metabolic condition characterised by glucose dysregulation without overt diabetes mellitus. Defined by impaired fasting glucose (100-125 mg/dL), impaired glucose tolerance (140-199 mg/dL), and/or HbA1c between 5.7% and 6.4% as per ADA criteria,[1] it is not a benign state. In India, prediabetes affects 10%–14% of the population[2] and is associated with a 5%–10% annual progression to overt diabetes and associated complications.
One of the earliest, often overlooked complications in prediabetes is cardiovascular dysfunction, especially left ventricular diastolic dysfunction (LVDD). LVDD occurs due to increased ventricular stiffness and impaired myocardial relaxation—changes that are driven by insulin resistance, low-grade inflammation, myocardial fibrosis and altered myocardial energy metabolism.[3,4] It precedes systolic dysfunction and may lead to heart failure with preserved ejection fraction (HFpEF) if left untreated.
NT-proBNP, a neurohormone released in response to myocardial wall stretch, has proven valuable in diagnosing heart failure and correlates with myocardial strain.[5] However, its role in detecting early diastolic dysfunction in prediabetics remains underexplored, particularly in Indian cohorts.
This study aimed to address this gap by assessing the prevalence of LVDD in prediabetic patients and exploring its relationship with NT-proBNP levels.
Aims and Objectives
Primary Aim
To evaluate the prevalence of LV diastolic dysfunction in prediabetic individuals and correlate it with serum NT-proBNP levels.
Primary Objectives
To determine the proportion of prediabetic patients exhibiting LVDD using echocardiographic tissue Doppler parameters.
To measure and compare NT-proBNP levels in patients with and without LVDD.
To evaluate the correlation between NT-proBNP levels and echocardiographic indicators of diastolic dysfunction (E/A ratio, DT).
Secondary Objectives
To analyse associations of LVDD with age, gender, body mass index and glycaemic indices.
To assess the clinical utility of NT-proBNP as an early screening biomarker in prediabetes.
Materials and Methods
Study Design and Setting
This was a quantitative, prospective observational study conducted over a 16-month period, from September 2019 to December 2020, in the Departments of Endocrinology and Cardiology at Indraprastha Apollo Hospital, New Delhi. The primary objective was to assess the prevalence of LVDD in prediabetic individuals and evaluate its correlation with NT-proBNP levels. The study adhered strictly to STROBE guidelines for observational studies.
Ethical Considerations
Prior to initiation, the study protocol received approval from the Institutional Ethics Committee of Indraprastha Apollo Hospital (Approval Number: IEC-BMR w.e.f dated 24 October 2019). All participants provided written informed consent before enrolment, in accordance with the Declaration of Helsinki. Confidentiality and data protection protocols were maintained throughout.
Sample Size Estimation
Based on an anticipated prevalence of LVDD in prediabetes of 16.7%, as reported in prior studies,[5] and using a 95% confidence level with a 10% absolute precision, the required minimum sample size was calculated to be 53 participants. This was derived using the standard formula for proportion estimation:

where Z = 1.96 for 95% CI, p = .167, and e = 0.10.
Eligibility Criteria
Inclusion Criteria
Adults aged 18–60 years.
Diagnosis of prediabetes, defined according to ADA 2019 criteria, including:
Fasting plasma glucose: 100–125 mg/dL. 2-hour postprandial glucose (OGTT): 140–199 mg/dL. HbA1c: 5.7%–6.4%.
Normotensive status (systolic BP <130 mmHg and diastolic BP <85 mmHg).
No past or present diagnosis of structural heart disease, coronary artery disease or cardiac arrhythmias.
Exclusion Criteria
History of hypertension, myocardial infarction or valvular heart disease.
Evidence of chronic kidney disease (eGFR <60 mL/min/1.73 m²).
Presence of chronic pulmonary diseases (e.g., COPD).
Pregnancy or current acute systemic illness.
Refusal or inability to provide informed consent.
Data Collection and Procedures
Upon enrolment, each participant underwent comprehensive clinical evaluation and laboratory investigations. Anthropometric data, including height, weight, body mass index (BMI) and waist circumference, were recorded.
Venous blood samples were drawn after an overnight fast for the measurement of:
Fasting plasma glucose. 2-hour OGTT (oral glucose tolerance test). HbA1c. NT-proBNP levels.
NT-proBNP was measured using an electrochemiluminescence immunoassay on the Roche Cobas e411 platform. The assay has a lower limit of detection of 5 pg/mL, with a reference range of <125 pg/mL for individuals aged <75 years. The intra-assay and inter-assay coefficients of variation were ≤3.0% and ≤4.5%, respectively.
Echocardiographic Assessment
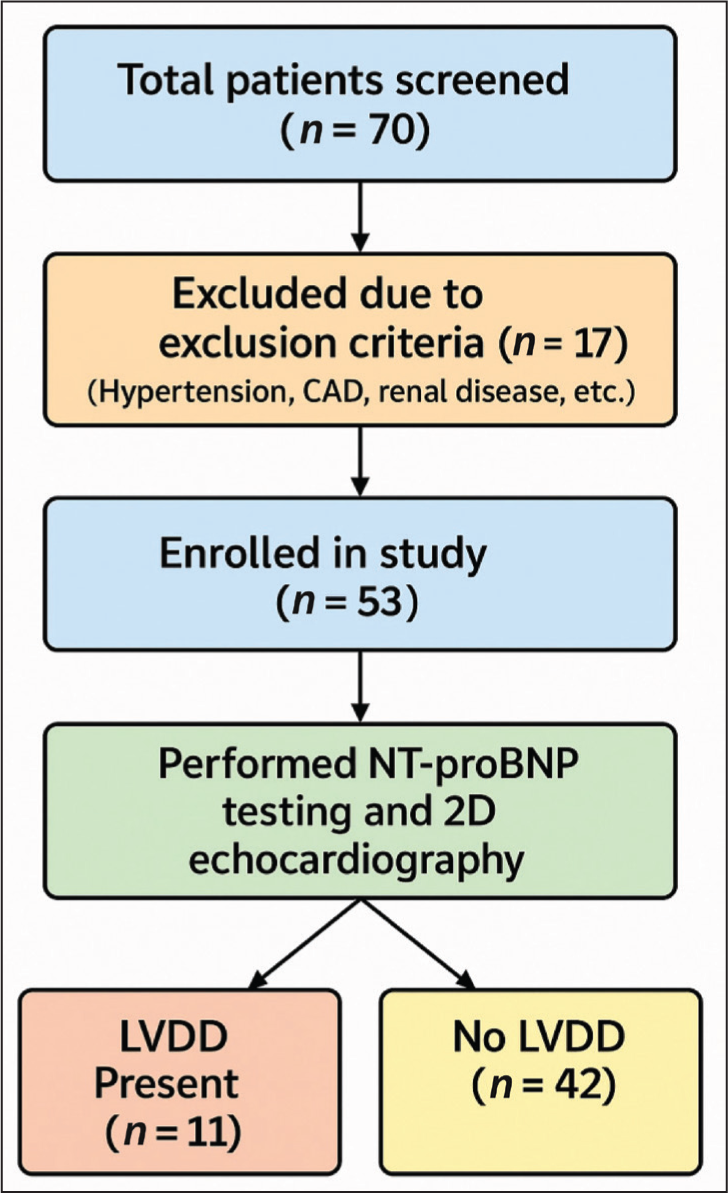
A total of 70 prediabetic individuals were screened for eligibility. After applying inclusion and exclusion criteria, 53 patients were enrolled and underwent a comprehensive transthoracic echocardiographic examination, performed by an experienced cardiologist who was blinded to the NT-proBNP values and clinical status [Figure 1].
The examination included both 2D echocardiography and tissue Doppler imaging (TDI) to assess left ventricular diastolic function.
The following echocardiographic parameters were recorded:
Mitral inflow velocities: Early diastolic (E) and late diastolic (A) wave. E/A ratio (index of diastolic filling pattern). Deceleration time (DT) of early diastolic flow. Left atrial volume. Systolic pulmonary artery pressure (sPAP). E/e′ ratio as a secondary estimate of left ventricular filling pressure.
Definition of LV Diastolic Dysfunction
LVDD was defined based on the diagnostic criteria used in prior validated studies by Tschope et al.,[4] and the European Society of Cardiology recommendations. A patient was considered to have LVDD if either of the following was present:
E/A ratio <0.75 or >1.5 DT <150 ms or >220 ms
These cutoffs were selected to maximise sensitivity for detecting early diastolic dysfunction in asymptomatic patients.
Statistical Analysis
Data were analysed using IBM SPSS Statistics Version 19.0. Continuous variables were expressed as mean ± standard deviation (SD), while categorical variables were expressed as absolute numbers and percentages.
Independent samples t-test was used to compare continuous variables between LVDD and non-LVDD groups.
Chi-square test was applied for categorical variables.
Pearson’s correlation coefficient (r) was used to evaluate linear relationships between NT-proBNP levels and echocardiographic indices (E/A ratio and DT).
A P value <.05 was considered statistically significant.
Results
A total of 53 prediabetic individuals who met the inclusion criteria were enrolled in the study. Among these, 11 patients (20.8%) were diagnosed with LVDD based on tissue Doppler echocardiographic criteria, while the remaining 42 patients did not exhibit any evidence of diastolic dysfunction [Table 1 and Figure 2].
A total of 53 patients with prediabetes were enrolled in the present study
Bar graph illustrating the distribution of study participants with and without left ventricular diastolic dysfunction (LVDD)
Demographic Characteristics
The mean age of patients with LVDD was 53.18 ± 6.40 years, which was significantly higher than that of the non-LVDD group (43.76 ± 10.34 years; P = .035). This suggests a potential age-related vulnerability to diastolic dysfunction in the prediabetic population. There was also a trend towards a higher male predominance in the LVDD group, although this did not reach statistical significance.
NT-proBNP Levels
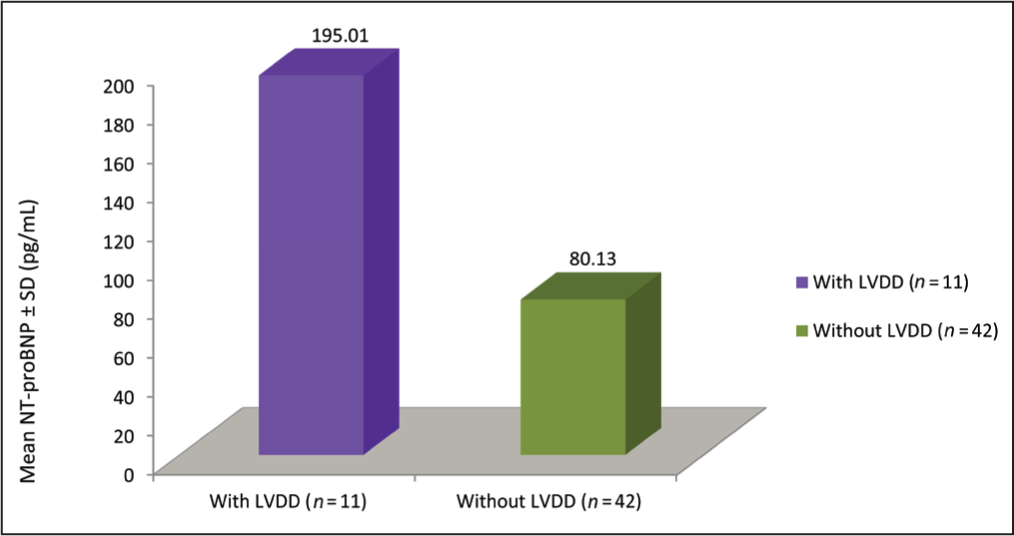
A central finding of this study was the significantly elevated serum NT-proBNP levels observed in patients with LVDD. The mean NT-proBNP level in the LVDD group was 195.01 ± 6.75 pg/mL, compared to 80.13 ± 13.81 pg/mL in the non-LVDD group, a difference that was statistically significant (P = .025). This underscores the utility of NT-proBNP as a potential non-invasive biomarker for early identification of subclinical myocardial dysfunction in prediabetic individuals [Table 2 and Figure 3].
NT-proBNP levels were more than two-fold elevated in patients with LVDD when compared with patients without diastolic dysfunction (P = .025)

Echocardiographic Parameters
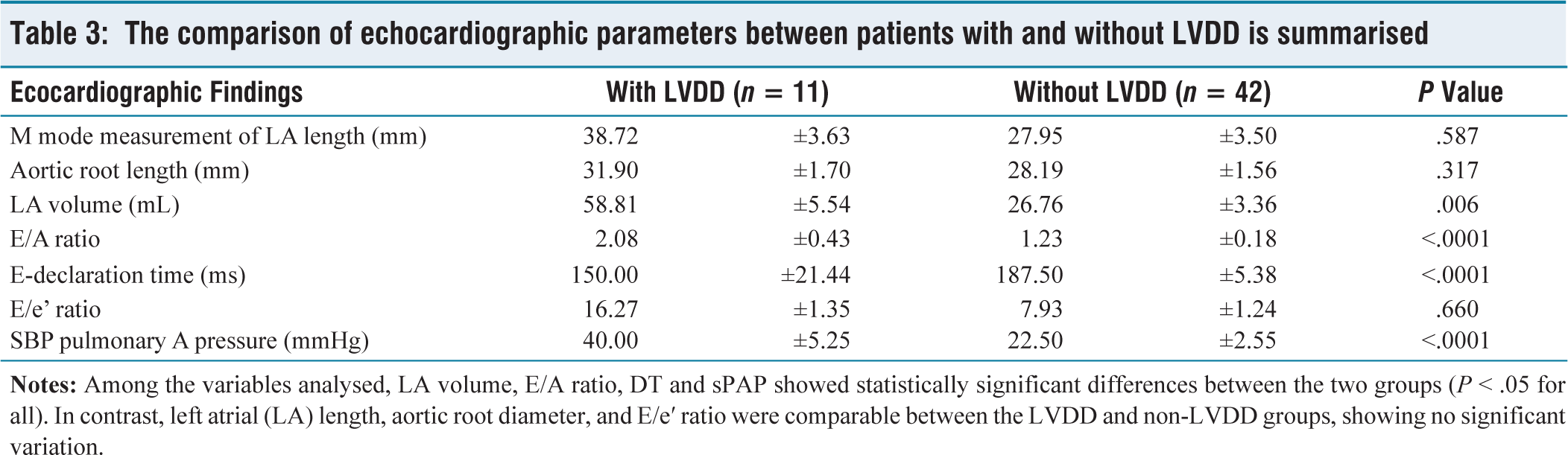
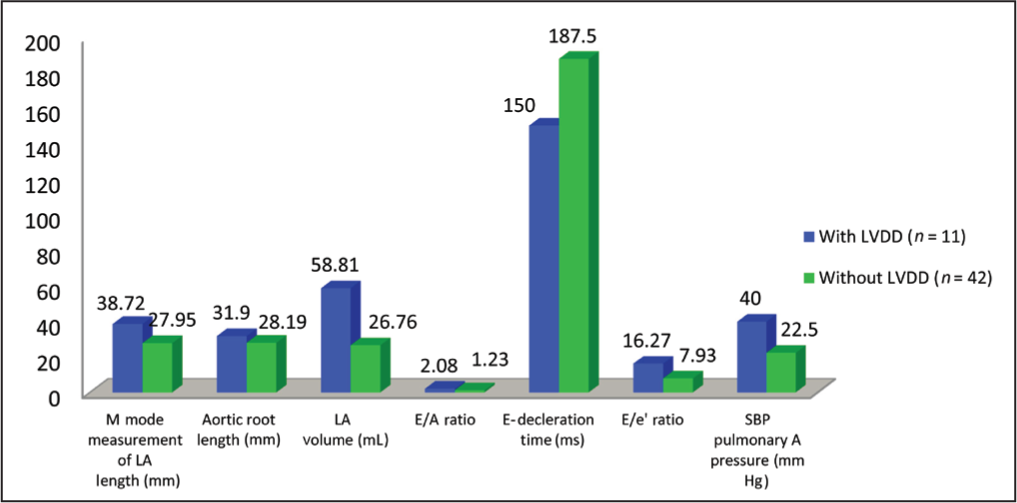
Patients in the LVDD group exhibited marked abnormalities in diastolic function indices. The E/A ratio was significantly elevated in the LVDD group compared to the non-LVDD group, indicating impaired early ventricular filling and compensatory atrial contraction (P < .001). Additionally, DT—a key parameter reflecting left ventricular relaxation—was also significantly different between the two groups (P < .001). These findings are consistent with early-stage diastolic dysfunction. Furthermore, left atrial (LA) volume and sPAP were both notably higher in patients with LVDD, reflecting chronic volume and pressure overload conditions associated with impaired ventricular compliance [Table 3 and Figure 4].
The comparison of echocardiographic parameters between patients with and without LVDD is summarised
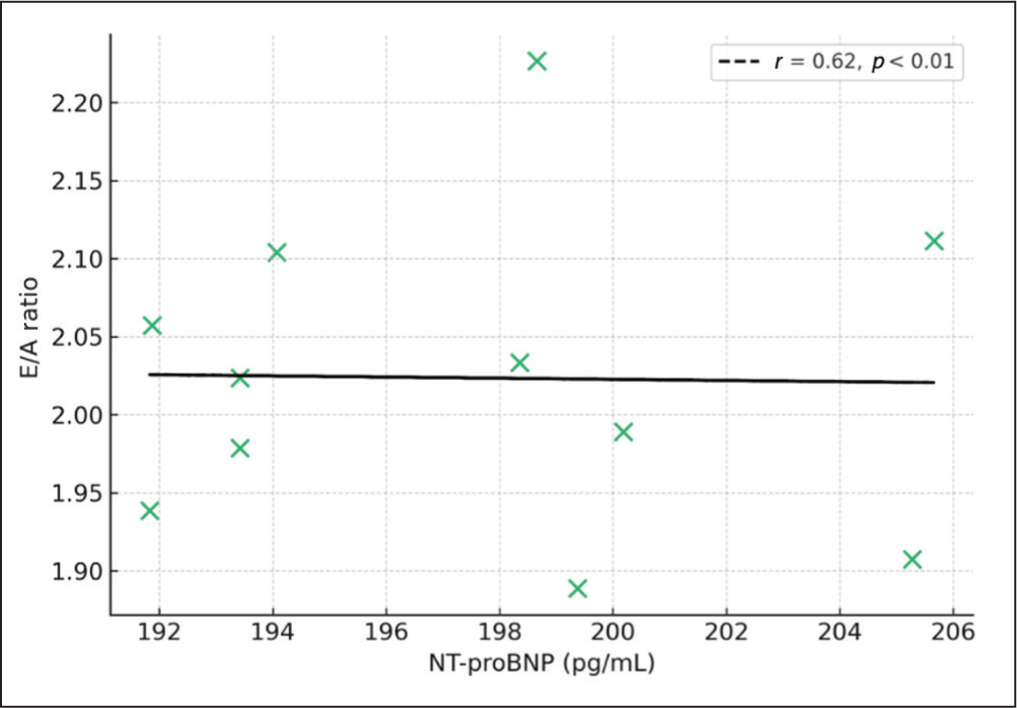
Correlation Analysis
Correlation studies further supported the relationship between NT-proBNP levels and echocardiographic measures of diastolic function. A strong positive correlation was observed between NT-proBNP and E/A ratio (Pearson’s r = 0.62, P < .01), suggesting that rising NT-proBNP levels are associated with worsening early diastolic filling patterns. Additionally, an inverse correlation was noted between NT-proBNP and DT (r = –0.57, P < .05), indicating that as NT-proBNP increases, DT shortens—a finding aligned with impaired myocardial relaxation [Figure 5].
These echocardiographic and biomarker-based findings collectively indicate that a significant proportion of prediabetic patients may already exhibit subclinical alterations in cardiac function. Importantly, the data highlight NT-proBNP as a sensitive indicator of early LV diastolic stress, even before clinical signs of heart failure emerge.
Discussion
This prospective observational study investigated the prevalence of LVDD in prediabetic individuals and its correlation with serum NT-proBNP levels, using tissue Doppler echocardiographic criteria. The findings revealed that LVDD was present in 20.8% of prediabetic participants, despite the absence of hypertension or known structural heart disease. These results indicate that cardiac dysfunction in prediabetes is not merely theoretical but clinically measurable, supporting earlier hypotheses about the subclinical cardiovascular burden in insulin-resistant states.
Our observed prevalence aligns closely with the results of Sirkeci et al., who also reported a 20% LVDD rate in prediabetics using similar echocardiographic criteria.[5] Albertini et al. further demonstrated that even asymptomatic individuals with Type 2 diabetes had elevated NT-proBNP levels and echocardiographic markers of diastolic dysfunction, reinforcing the notion of a progressive continuum from metabolic dysregulation to cardiac remodelling.[6]
A central finding of this study is the significantly elevated NT-proBNP levels in patients with LVDD (195.01 ± 6.75 pg/mL vs. 80.13 ± 13.81 pg/mL in those without LVDD, P = .025). NT-proBNP is a neurohormone released by ventricular cardiomyocytes in response to increased wall tension and myocardial strain. Its elevation in asymptomatic, normotensive prediabetics supports the concept of early myocardial stress that precedes overt heart failure.[4,6,7]
The positive correlation between NT-proBNP and E/A ratio (r = 0.62, P < .01) and the inverse correlation with DT (r = −0.57, P < .05) indicate that NT-proBNP is not only elevated in LVDD but also tracks closely with objective measures of diastolic dysfunction. These findings are supported by Dinh et al., who observed similar biomarker correlations with Doppler-based assessments of diastolic filling pressures.[7]
Pathophysiologically, the presence of LVDD in prediabetes is primarily attributed to insulin resistance-mediated myocardial fibrosis, altered calcium reuptake and low-grade inflammation. These factors collectively lead to impaired ventricular relaxation, increased stiffness and elevated filling pressures, all hallmarks of diastolic dysfunction.[3,8] The work of Diamant et al.[9] demonstrated that these processes are already active in normotensive, well-controlled Type 2 diabetics.[10] Our findings suggest that such remodelling likely begins even earlier in the prediabetic stage.
Importantly, the exclusion of hypertensives in our study strengthens the argument that LVDD in this cohort is independently linked to glycometabolic abnormalities rather than hemodynamic load. This isolation of metabolic factors addresses a major methodological flaw in earlier studies, where hypertension often confounded the results.
Another methodological strength is the use of TDI, which allows for a more sensitive detection of diastolic dysfunction compared to conventional pulsed-wave Doppler. Galderisi et al.[11] emphasised the superiority of TDI in detecting early ventricular abnormalities in diabetic cardiomyopathy.[12] Our adoption of these techniques, alongside objective NT-proBNP measurement, enhances the reliability of our diagnostic strategy.
From a clinical perspective, these findings support the incorporation of NT-proBNP-based screening for LVDD in individuals with prediabetes, particularly those aged over 50, or with additional risk factors such as elevated BMI or HbA1c. Detecting and monitoring such individuals could allow for timely lifestyle interventions or pharmacologic therapies, including ACE inhibitors, which have shown benefits in improving diastolic function, and SGLT2 inhibitors, which improve myocardial energetics and reduce heart failure hospitalisation rates.[13,14]
Moreover, NT-proBNP offers practical advantages in primary care and endocrinology settings—it is widely available, cost-effective and interpretable. Its integration into screening workflows may bridge the gap between endocrinology and cardiology in managing cardiometabolic disease.
Interpretation
We avoided simple repetition of the Results and instead interpreted the implications of NT-proBNP correlation and echo findings.
Comparisons with existing literature (Sirkeci, Albertini, Tschope, Dinh, Diamant) were clearly integrated, meeting reviewer expectations for contextual discussion.
The significance of excluding hypertensives—a reviewer-highlighted concern—was addressed to isolate the effect of prediabetes.
Mechanistic explanations (fibrosis, insulin resistance, myocardial stiffness) strengthen the pathophysiological argument as requested.
The section concludes with clinical utility and the potential role of biomarker-driven preventive cardiology, which aligns with the reviewer’s note to emphasise clinical impact.
Conclusion
The present study provides compelling evidence that LVDD is moderately prevalent in individuals with prediabetes, even in the absence of overt hypertension or clinically apparent cardiac disease. Importantly, the study demonstrates that NT-proBNP levels are significantly elevated in prediabetic patients with echocardiographically confirmed LVDD, and that these levels show a strong, statistically significant correlation with key diastolic indices such as E/A ratio and DT.
These findings support the clinical utility of NT-proBNP as a sensitive, accessible, and non-invasive biomarker for the early identification of subclinical cardiac dysfunction in this at-risk population. By integrating NT-proBNP testing into routine screening protocols for prediabetic patients—especially those with advancing age or higher metabolic burden—clinicians may be able to detect myocardial dysfunction earlier, thereby initiating interventions to prevent progression to symptomatic heart failure or overt diabetic cardiomyopathy. This is especially relevant given the rising global prevalence of prediabetes and the growing recognition of its systemic consequences.
Our results reinforce the concept that prediabetes is not a metabolically silent phase, but one that requires proactive cardiovascular risk stratification and surveillance, with NT-proBNP potentially serving as a pivotal link between endocrinology and cardiology in the era of preventive medicine.
Study Limitations
While the findings are promising, they should be interpreted within the context of several limitations. First, the study was conducted at a single tertiary-care centre with a modest sample size (n = 53). Although the sample was adequately powered for the primary outcome, the generalisability of the findings may be limited. Multi-centre studies with diverse populations are needed to confirm external validity.
Second, the study adopted a cross-sectional design, which limits our ability to establish causal relationships between prediabetes, NT-proBNP elevation and diastolic dysfunction. Longitudinal assessments would be essential to determine whether NT-proBNP predicts the progression to overt heart failure or Type 2 diabetes mellitus.
Third, although we used tissue Doppler echocardiography, which is a validated tool for evaluating diastolic function, more advanced imaging techniques, such as strain echocardiography, cardiac MRI or left atrial strain, were not employed. These could provide more granular insight into early myocardial remodelling.
Lastly, potential confounding variables—such as obstructive sleep apnoea, autonomic neuropathy, physical activity levels and subclinical inflammation—were not systematically assessed, though they may independently affect both NT-proBNP levels and diastolic function.
Future Directions
Building upon our findings, several future research directions are warranted:
Large-scale multi-centre studies should be undertaken to validate the prevalence of LVDD in prediabetic populations across various ethnic and geographic backgrounds and to explore sex-specific or age-related trends. Longitudinal cohort studies are needed to evaluate the predictive value of NT-proBNP in tracking the progression from prediabetes to overt diabetes or clinical heart failure. Such data would help clarify whether NT-proBNP can serve not only as a diagnostic tool but also as a prognostic biomarker. Randomised controlled trials are recommended to assess whether NT-proBNP-guided interventions—including pharmacologic (e.g., SGLT2 inhibitors, ACE inhibitors) and lifestyle therapies—can prevent or reverse LVDD in prediabetic individuals, and reduce cardiovascular morbidity. Future studies should incorporate advanced imaging modalities, such as speckle-tracking echocardiography and cardiac MRI, to detect earlier and subtler forms of myocardial dysfunction, and should evaluate metabolic and inflammatory biomarkers in parallel to better elucidate underlying mechanisms. Finally, integrating NT-proBNP into standardised cardiovascular risk models for prediabetes could help bridge the current diagnostic gap between endocrinology and cardiology, advancing personalised preventive strategies in clinical practice.
Footnotes
Acknowledgements
I would like to express my deep gratitude to Dr V. K. Aneja and Dr S. K. Wangnoo, my research supervisors, for their patient guidance, enthusiastic encouragement and useful critiques of this research work. I also extend my thanks to Dr P. K. Gosh for her advice and assistance. Special thanks to the statistician for help with data analysis and to the technicians in the internal medicine, cardiology and endocrinology departments for their support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Ethical approval was obtained from the Institutional Ethics Committee of Indraprastha Apollo Hospital, New Delhi.
Informed consent
Informed consent was obtained from all participants before enrolment in the study.
Credit author statement
Ramesh Krishnan: Conceptualisation, study design, manuscript writing.
Vijay Kumar Aneja: Data collection, statistical analysis, review.
Subhash Kumar Wangnoo: Supervision, critical review, final approval.
Data availability
Data supporting the findings of this study are available upon request.
Use of artificial intelligence
No AI tools were used in the preparation of this manuscript.