
Abstract
Background:
Pseudomyxoma peritonei (PMP) is a rare clinical syndrome characterised by progressive intraperitoneal accumulation of mucinous ascites, most commonly arising from appendiceal mucinous neoplasms. Once uniformly fatal, the prognosis has been transformed by cytoreductive surgery (CRS) combined with hyperthermic intraperitoneal chemotherapy (HIPEC). Nevertheless, controversies persist regarding diagnostic strategies, surgical thresholds and the true incremental value of HIPEC.
Objective:
This review synthesises contemporary evidence on the pathogenesis, diagnostic pearls, surgical decision-making and HIPEC controversies in PMP, while exploring emerging systemic and targeted therapies and future directions in biomarker-driven and AI-assisted management.
Methods:
A comprehensive literature review of PubMed-indexed studies from 2000 to 2025 was performed, with emphasis on systematic reviews, meta-analyses, randomised controlled trials and multicentre registries. Key themes were integrated under diagnostic evaluation, surgical selection, HIPEC pharmacology, systemic therapy limitations and translational innovations. Seminal historical references were retained selectively for context.
Conclusion:
PMP exemplifies the convergence of rare disease biology and surgical audacity. CRS remains the cornerstone, with peritoneal cancer index (PCI) and completeness of cytoreduction (CC score) guiding operative decision-making. While HIPEC is widely practised, the absence of randomised data in PMP sustains debate over its necessity, optimal regimens and feasibility in low-resource settings. Systemic therapies remain limited, but novel mucinase strategies, immunotherapy and AI-driven imaging prediction herald a future of personalised care. Global collaboration through registries and consensus frameworks will be critical to resolving controversies and ensuring equitable access to curative strategies worldwide.
Keywords
Introduction
Pseudomyxoma peritonei (PMP) is a rare but distinct clinical-pathological entity characterised by the progressive accumulation of mucinous ascites within the peritoneal cavity, most often arising from perforated appendiceal neoplasms. Its natural history is unique: despite frequently indolent histology, untreated disease inexorably leads to debilitating abdominal distension, bowel obstruction and eventual cachexia, marking PMP as a condition where tumour biology and anatomic redistribution dynamics outweigh conventional staging paradigms.[1,2]
Historically, PMP was considered uniformly fatal, with survival rarely extending beyond a few years. The evolution of combined cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) has revolutionised its outlook, offering select patients long-term survival and even potential cure.[3] Yet, the heterogeneity in pathological classification, variability in surgical expertise and ongoing debate surrounding HIPEC’s necessity and regimen continue to generate uncertainty in both practice and policy.[4]
Recent population-level analyses confirm PMP’s rarity, with an estimated incidence of 1–3 cases per million annually.[5] This rarity poses challenges for generating high-level evidence, often relegating decision-making to retrospective series and single-institution experiences. However, advances in registries, multicentre collaborations and refined molecular insights are beginning to bridge these evidence gaps, positioning PMP as a model disease for international cooperation in rare tumour management.[6]
Thus, this review aims to synthesise contemporary evidence on the diagnostic pearls, surgical decision-making frameworks and ongoing HIPEC controversies, with an emphasis on recent literature (2000–2025), meta-analyses and clinical trial data, to guide both surgeons and oncologists in navigating this complex disease.
Diagnostic Pearls: Imaging and Laboratory
The diagnosis of PMP hinges on early recognition of its radiologic and biochemical hallmarks. Unlike peritoneal carcinomatosis from other primaries, PMP exhibits a distinct pattern of peritoneal dissemination, guided by the redistribution phenomenon of mucin within dependent recesses of the peritoneal cavity.
Cross-sectional imaging remains the cornerstone. Contrast-enhanced computed tomography (CT) is widely available and offers robust detection of peritoneal mucinous deposits. The pathognomonic finding is scalloping of visceral surfaces, particularly the liver and spleen, resulting from pressure exerted by extracellular mucin rather than invasive parenchymal infiltration.[7] However, CT has limitations in underestimating disease burden in subtle or loculated disease.
MRI, especially diffusion-weighted sequences, provides superior sensitivity in delineating peritoneal cancer index (PCI) scores compared to CT. Recent prospective studies have demonstrated MRI’s ability to capture mucinous deposits better and predict resectability, particularly in the subdiaphragmatic and pelvic compartments.[8,9] In centres with high PMP volume, MRI is increasingly favoured as the preoperative staging modality of choice.[10]
Serological tumour markers complement imaging by providing prognostic and surveillance value. Elevated carcinoembryonic antigen (CEA), CA19-9 and CA-125 levels correlate with a higher tumour burden and inferior outcomes, although they lack disease specificity.[11] Integration of these biomarkers with imaging findings enhances risk stratification and allows longitudinal monitoring. Recent multi-institutional analyses underscore that normalisation of tumour markers after CRS/HIPEC is associated with improved survival, further reinforcing their utility in postoperative follow-up.[12]
In summary, the triad of CT scalloping, MRI-defined PCI precision and tumour marker profiling constitutes the diagnostic backbone of PMP. Optimal preoperative assessment relies on judicious use of all three, ensuring accurate staging and surgical planning.
The baseline radiologic and laboratory hallmarks of PMP are summarised in Table 1, highlighting the complementary role of CT, MRI, PET/CT and serum tumour markers.
Diagnostic imaging and laboratory pearls in pseudomyxoma peritonei (PMP)
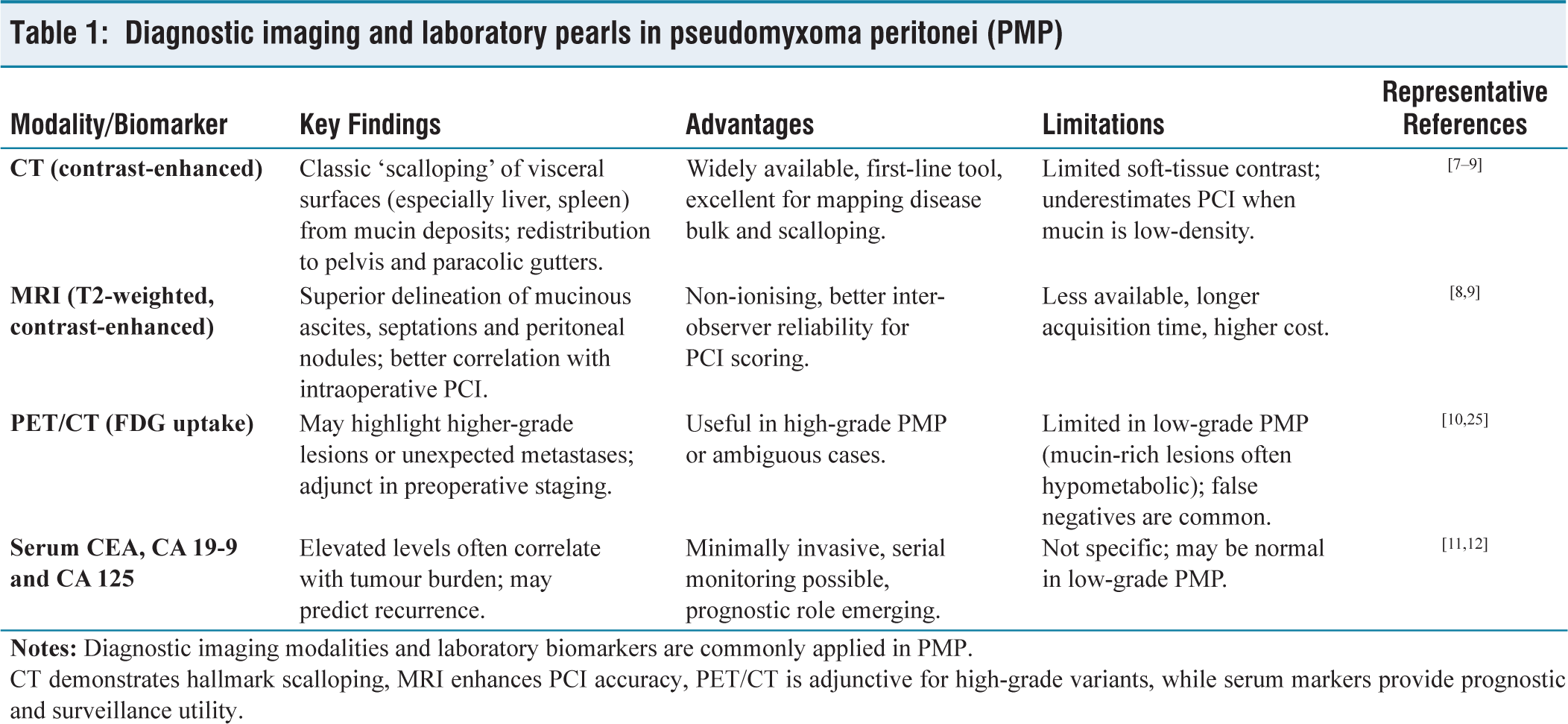
CT demonstrates hallmark scalloping, MRI enhances PCI accuracy, PET/CT is adjunctive for high-grade variants, while serum markers provide prognostic and surveillance utility.
Pathogenesis and Molecular Insights
The pathogenesis of PMP reflects a unique interplay between tumour biology and peritoneal fluid dynamics. Unlike peritoneal spread from high-grade carcinomas, PMP dissemination is largely dictated by the redistribution phenomenon: mucin-secreting epithelial cells shed into the peritoneal cavity, survive in suspension and implant along gravity-dependent surfaces such as the omentum, pelvis and paracolic gutters.[4] This non-invasive mechanical spread explains the predilection for scalloping of visceral organs rather than parenchymal infiltration and underlies the rationale for cytoreductive strategies targeting the peritoneal compartment.
At the molecular level, PMP is no longer regarded as a monolithic entity. High-throughput sequencing studies have consistently demonstrated Guanine Nucleotide Binding Protein, Alpha Stimulating (GNAS) and Kirsten Rat Sarcoma Viral Oncogene Homolog (KRAS) mutations as the dominant drivers, implicating cyclic Adenosine Monophosphate (AMP) and Mitogen-Activated Protein Kinase (MAPK) signalling pathways in mucin hypersecretion.[13] GNAS mutations, in particular, appear nearly pathognomonic for appendiceal mucinous neoplasms and correlate with excessive extracellular mucin accumulation, a hallmark of the disease.
Beyond these canonical alterations, secondary events such as Tumor Protein p53 (TP53) and Mothers Against Decapentaplegic Homolog 4 (SMAD4) mutations are more frequently encountered in high-grade variants, aligning with their aggressive clinical course and poorer outcomes.[14] These molecular distinctions not only provide insight into the biological heterogeneity of PMP but also hold promise for prognostication and therapeutic targeting. For instance, stratifying patients based on mutation profiles may inform adjuvant systemic strategies or identify candidates for novel mucinase or immunotherapeutic trials.
Thus, PMP pathogenesis can be conceptualised as a mucin-driven, mutation-fuelled peritoneal ecosystem, where epithelial cells exploit redistribution dynamics while genetic alterations shape grade, behaviour and eventual outcomes.
The central molecular drivers of PMP are consolidated in Table 2, illustrating how KRAS and GNAS dominate low-grade disease while TP53, SMAD4 and mismatch-repair deficiency mark high-grade biology.
Molecular and pathogenesis insights into pseudomyxoma peritonei (PMP)
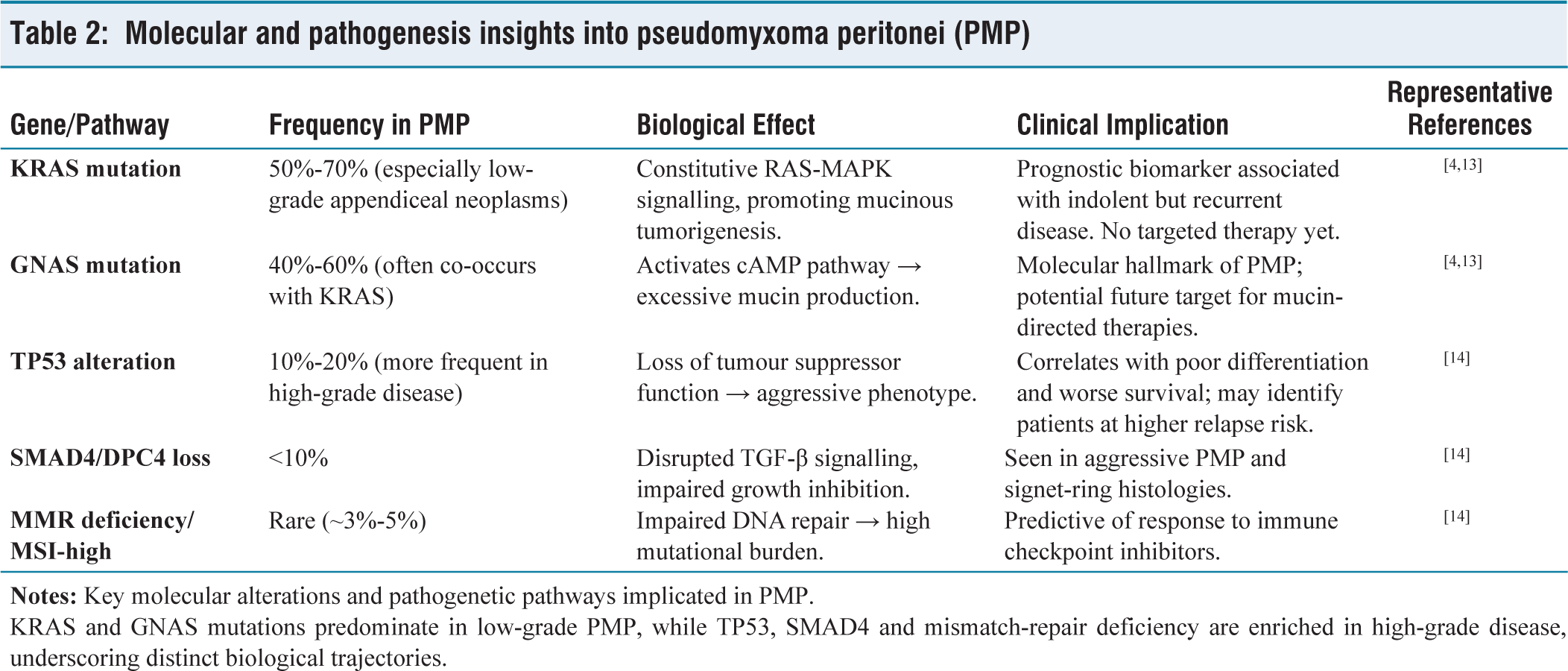
KRAS and GNAS mutations predominate in low-grade PMP, while TP53, SMAD4 and mismatch-repair deficiency are enriched in high-grade disease, underscoring distinct biological trajectories.
Surgical Decision-making
CRS remains the cornerstone of curative treatment for PMP. The guiding principle is complete removal of all visible disease, recognising that residual mucinous implants act as reservoirs for recurrence. Decision-making is therefore governed by three interlinked determinants: disease burden, patient fitness and institutional expertise.
Disease burden assessment is anchored in the PCI, which scores mucin distribution across 13 abdominopelvic regions. Several prospective series confirm PCI as the most reliable predictor of resectability and survival, with outcomes significantly inferior when PCI exceeds 20–24.[15,16] Imaging modalities may underestimate PCI, making intraoperative exploration the gold standard for surgical planning.
Completeness of cytoreduction (CC score) is equally critical. Only patients achieving CC-0 (no residual disease) or CC-1 (residual nodules ≤2.5 mm) derive a survival benefit from CRS.[17] Conversely, incomplete cytoreduction portends poor prognosis and should prompt consideration of palliative approaches rather than futile extensive resections.
Patient selection balances oncologic ambition with perioperative risk. CRS is among the most morbid abdominal operations, with operative times often exceeding 10 hours and complication rates approaching 30%-40% in some registries.[6,18] High-volume centres mitigate these risks through specialised anaesthesia protocols, enhanced recovery pathways and multidisciplinary prehabilitation.[19] Outcomes from experienced units underscore that surgical expertise is as pivotal as disease biology in determining results.
Technical refinements have also shaped surgical paradigms. Peritonectomy procedures and multivisceral resections are frequently required, with the extent of resection tailored to achieve macroscopically complete clearance. Laparoscopic or robotic cytoreduction remains investigational, with early reports suggesting feasibility but not yet equivalence to open approaches.[20]
Ethical considerations loom large in the setting of extreme tumour burden or prohibitive comorbidities. In such cases, debulking may relieve obstructive symptoms, but the survival benefit is minimal. Shared decision-making, incorporating patient values and quality-of-life expectations, is essential to avoid overtreatment.[21]
The key parameters influencing operative selection and outcomes are synthesised in Table 3, underscoring how PCI, CC score, tumour biology, patient resilience and surgical expertise converge to shape prognosis.
Surgical decision-making framework in pseudomyxoma peritonei (PMP)
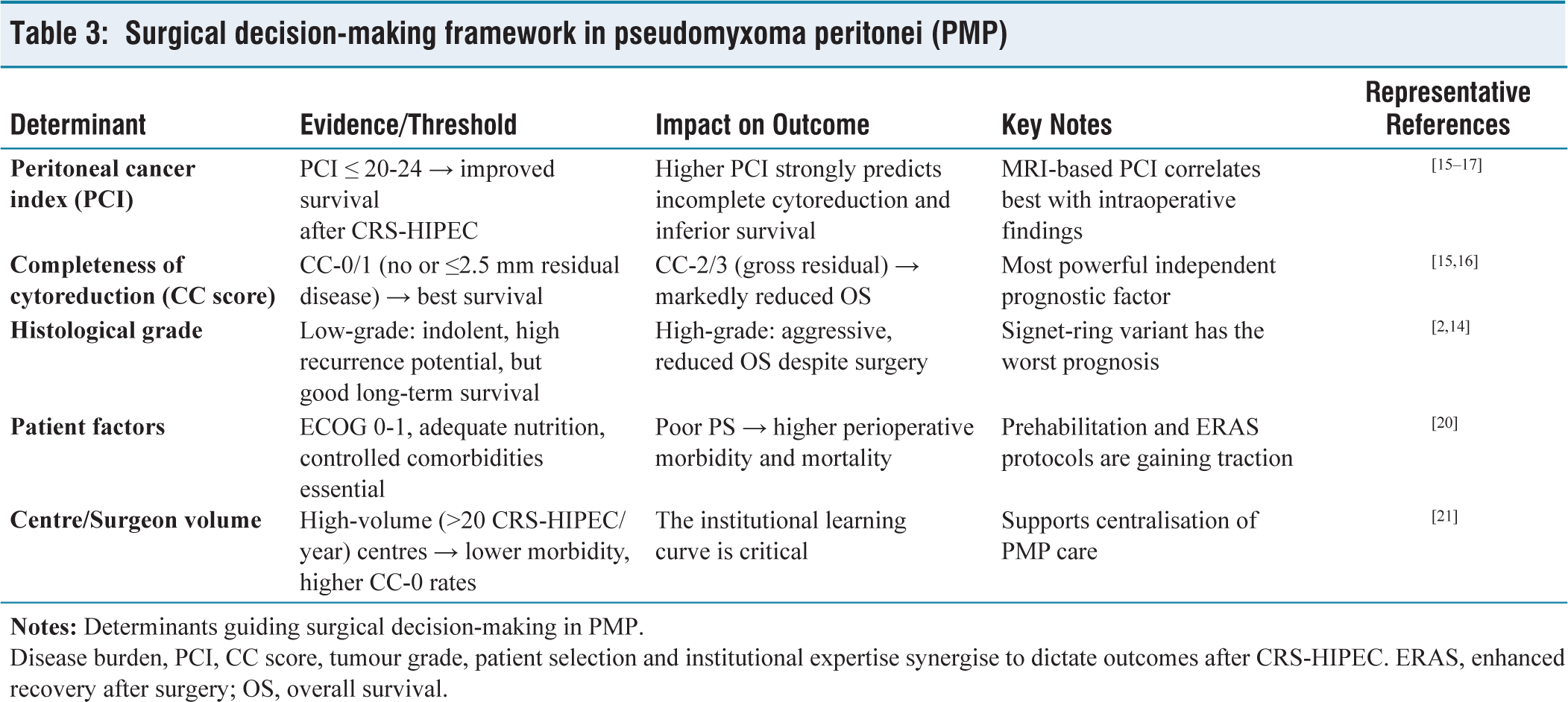
Disease burden, PCI, CC score, tumour grade, patient selection and institutional expertise synergise to dictate outcomes after CRS-HIPEC. ERAS, enhanced recovery after surgery; OS, overall survival.
Hence, surgical decision-making in PMP hinges on a triad: PCI-based burden assessment, CC score feasibility and patient resilience, all contextualised within high-volume expertise and ethical prudence.
HIPEC Controversies (Agent, Parameters and Necessity)
Why HIPEC
HIPEC is intended to eradicate residual microscopic disease after a macroscopically complete cytoreduction, leveraging heat-enhanced cytotoxicity and high intraperitoneal drug concentrations. In contemporary care pathways, many expert algorithms still pair HIPEC with CRS for appropriately selected PMP patients, while acknowledging the paucity of randomised, disease-specific evidence.[15,16]
Is HIPEC Necessary After Complete CRS
The central debate is whether the long-term survival in PMP primarily reflects the CC score or a true incremental benefit from HIPEC. Consensus and pathway documents emphasise that CC-0/CC-1 resection is the dominant driver of outcome and that the additive value of HIPEC, though biologically plausible, remains challenging to quantify definitively in PMP.[15,16] The 2021 Partenariat de Recherche en Oncologie Digestive (French collaborative group for GI oncology trials) (PRODIGE-7) trial in colorectal peritoneal metastases (a different biology) failed to show an overall survival advantage with oxaliplatin-based HIPEC versus CRS alone; while not a PMP study, its null result continues to fuel scepticism and calls for disease-specific trials and should be cited with explicit caution regarding extrapolation.[18]
Which Drug and How to Perfuse
There is marked heterogeneity across centres in agent choice (most commonly mitomycin-C or oxaliplatin), dose, carrier solutions, perfusion duration (≈30–90 minutes), temperature (≈41 °C-43 °C) and technique (open vs closed). Contemporary treatment algorithms and reviews endorse institutional protocolisation rather than a one-size-fits-all regimen, because high-quality head-to-head, PMP-specific data remain limited and outcomes are strongly confounded by surgical completeness and centre expertise.[15,16] Repeat cytoreduction in recurrence may again be coupled with HIPEC at selected units, but durable benefit still appears to hinge on achieving a second CC-0/CC-1 resection rather than the perfusion itself.[17]
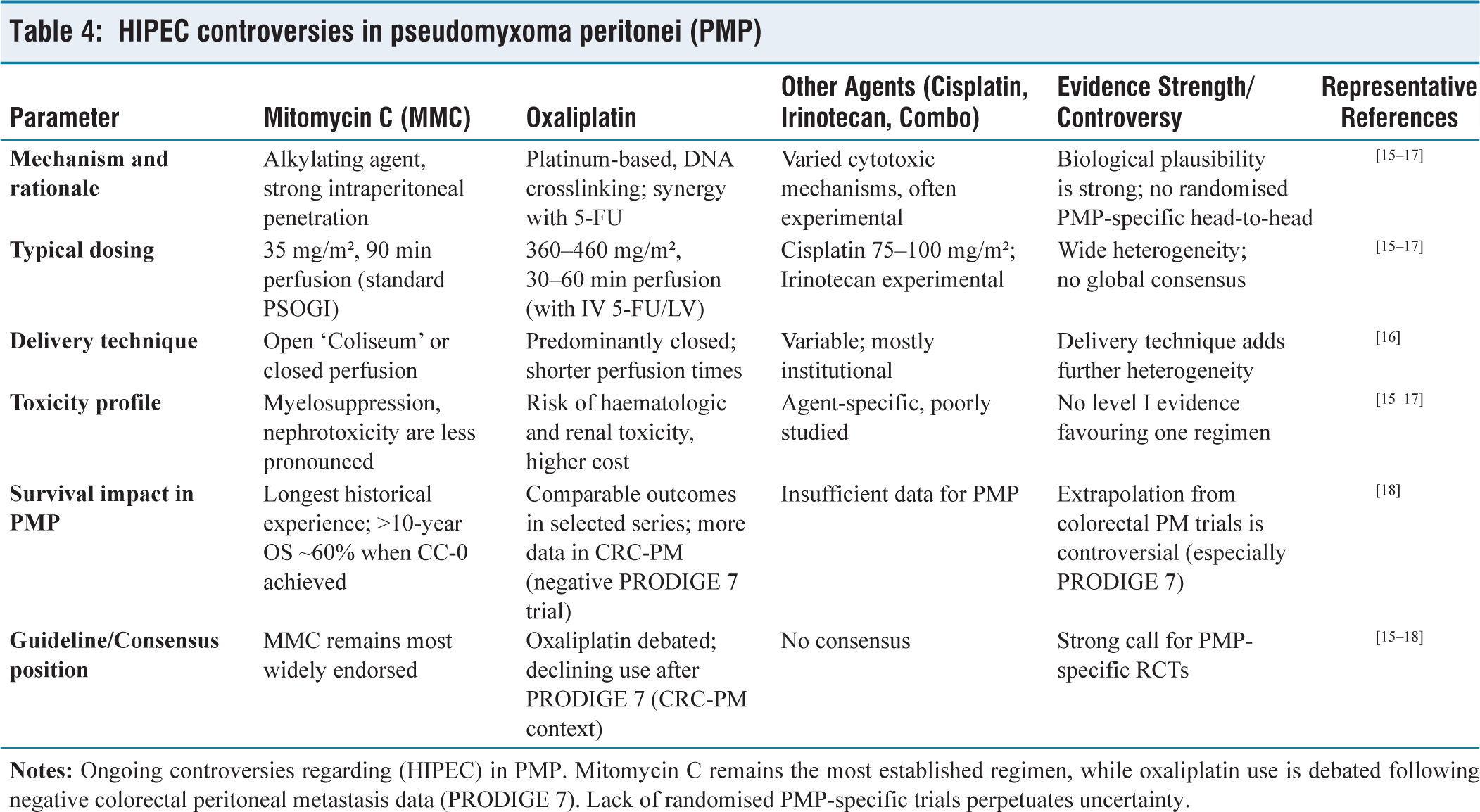
The competing HIPEC regimens and their relative strengths and limitations are summarised in Table 4, highlighting that much of the current debate stems from heterogeneous protocols and extrapolation from colorectal peritoneal metastasis trials.
HIPEC controversies in pseudomyxoma peritonei (PMP)
A pragmatic stance for 2025:
Prioritise complete cytoreduction; reserve HIPEC for settings where equipoise favours potential microscopic control and institutional outcomes are strong.[15,16] Standardise the local HIPEC protocol (agent, dose, duration, temperature and technique) within a multidisciplinary program and audit perioperative results.[15,16] Be explicit about evidence boundaries when counselling patients: PMP data are largely non-randomised; CRC-PM RCT results (PRODIGE-7) inform debate but are not directly generalisable.[18] Capture data prospectively (registries, trials) so centre-level heterogeneity can be translated into comparative effectiveness and, ultimately, standardised recommendations.[15–17]
Systemic and Targeted Therapy
The role of systemic therapy in PMP remains limited, largely because of the disease’s peritoneal-confined biology and mucin-dominant histopathology. Conventional cytotoxic regimens, such as 5-fluorouracil-based chemotherapy, have demonstrated only modest activity, generally reserved for unresectable or relapsed disease after cytoreduction and HIPEC.[22] Response rates remain under 20% and the impact on overall survival is minimal. These data reinforce the paradigm that surgical clearance continues to be the central therapeutic determinant.
Advances in molecular profiling have opened the door to targeted and personalised strategies. Mutations in KRAS and GNAS, present in a large proportion of low-grade appendiceal mucinous neoplasms, have emerged as candidate biomarkers, though currently without actionable therapies.[13] For high-grade PMP, occasional human epidermal growth factor receptor (HER2) amplification or mismatch-repair deficiency has been reported, prompting consideration of trastuzumab or immune checkpoint inhibitors in select, molecularly defined subsets.[14] Early anecdotal experiences suggest that immunotherapy may benefit a fraction of patients, yet prospective trials are lacking. Similarly, anti-vascular endothelial growth factor (VEGF) therapy has theoretical appeal given the angiogenic stroma, but real-world impact remains unproven.
Given the rarity of PMP, collaborative networks are critical for testing systemic agents. Basket trials that include appendiceal primaries, as well as ongoing registry-based studies, may yield future insights. Until robust trial data emerge, systemic therapy should be regarded as adjunctive, reserved for biologically aggressive phenotypes or for palliation where repeat surgery is not feasible.
The current landscape of systemic and targeted options, anchored in randomised data for chemotherapy and molecular logic for selective targeted/immunotherapies, is summarised in Table 5, emphasising that systemic therapy in PMP should be biomarker-guided and trial-focused rather than routine.
Systemic and targeted therapy landscape in pseudomyxoma peritonei (PMP)
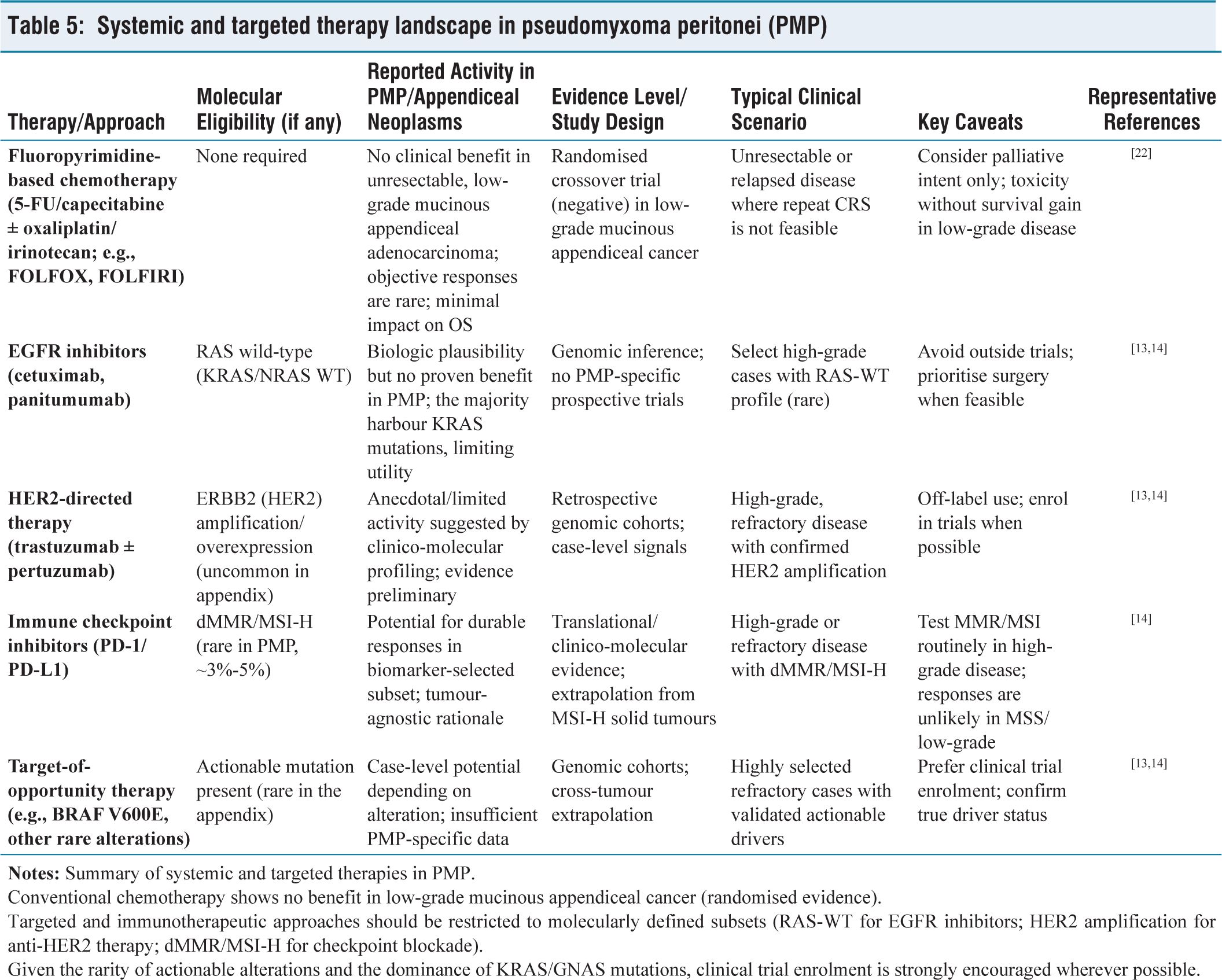
Conventional chemotherapy shows no benefit in low-grade mucinous appendiceal cancer (randomised evidence).
Targeted and immunotherapeutic approaches should be restricted to molecularly defined subsets (RAS-WT for EGFR inhibitors; HER2 amplification for anti-HER2 therapy; dMMR/MSI-H for checkpoint blockade).
Given the rarity of actionable alterations and the dominance of KRAS/GNAS mutations, clinical trial enrolment is strongly encouraged wherever possible.
Future Directions
The management of PMP is entering an era defined less by surgical daring and more by integration of translational science, data harmonisation and novel therapeutics. Molecular stratification will likely reshape patient selection, with KRAS/GNAS status and secondary mutations (e.g., TP53, SMAD4) informing prognosis and systemic therapy eligibility.[23] Precision medicine platforms, including basket and umbrella trials, may help repurpose targeted agents or immunotherapies from colorectal and pancreatic oncology into the PMP domain.
International registries and collaborative trial groups are addressing the evidence void. The Peritoneal Surface Oncology Group International (PSOGI) and other networks are spearheading efforts to pool multicentre data, standardise HIPEC protocols and validate PCI/CC score thresholds. Artificial intelligence and radiomics tools are also being explored to refine PCI estimation preoperatively, improving surgical planning and patient counselling.[24]
From a therapeutic standpoint, future research will test whether HIPEC can be de-escalated, individualised or replaced by alternative intraperitoneal delivery strategies, including pressurised intraperitoneal aerosol chemotherapy (PIPAC). Meanwhile, bioengineering approaches to mucin degradation and stromal targeting hold promise for directly addressing the pathophysiologic driver of PMP.
Emerging innovations in PMP management are summarised in Table 6, which outlines domains ranging from AI-enhanced imaging to registry harmonisation, underscoring both potential and current evidence gaps.
Future directions and innovations in pseudomyxoma peritonei (PMP)
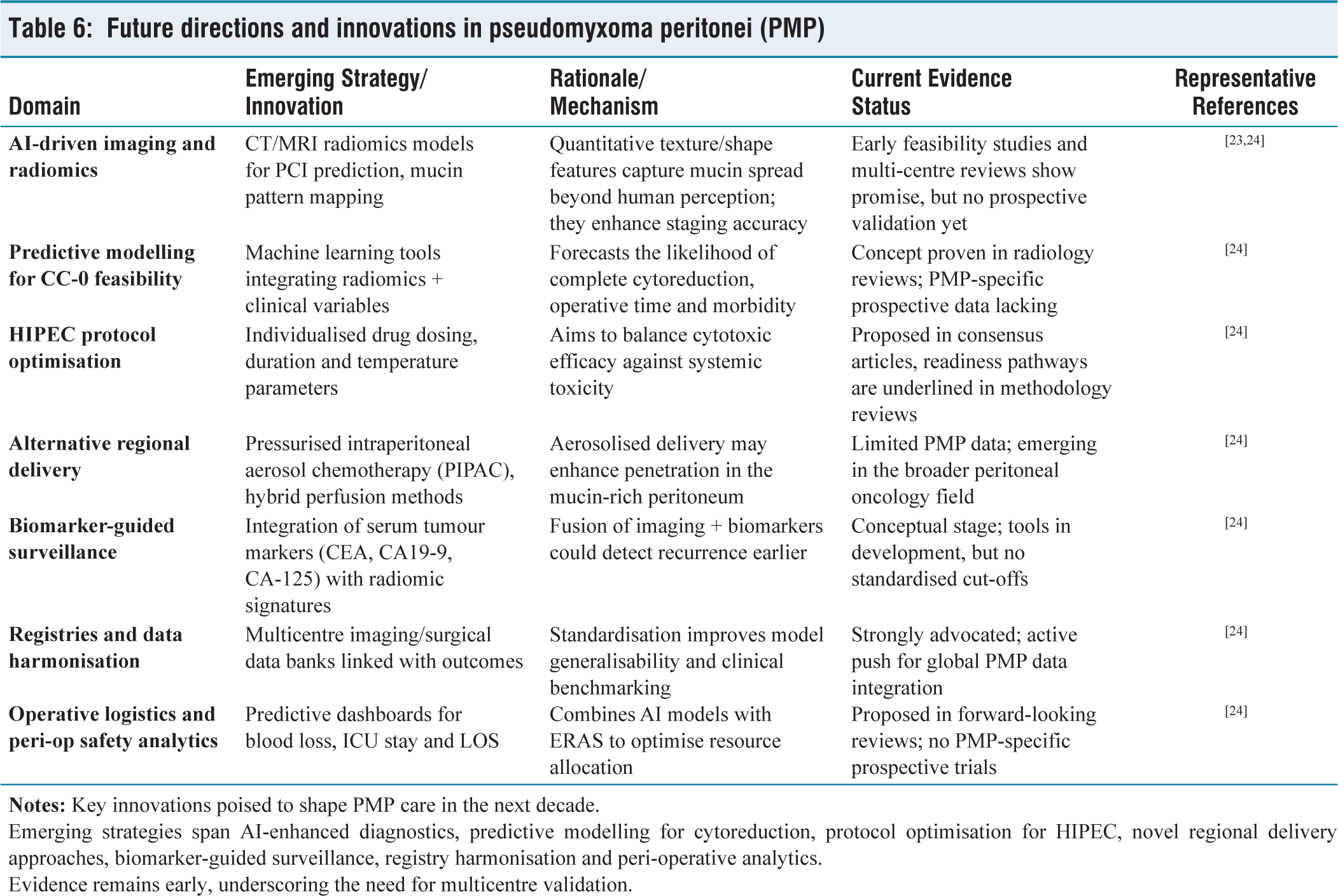
Emerging strategies span AI-enhanced diagnostics, predictive modelling for cytoreduction, protocol optimisation for HIPEC, novel regional delivery approaches, biomarker-guided surveillance, registry harmonisation and peri-operative analytics.
Evidence remains early, underscoring the need for multicentre validation.
The next decade will likely see PMP management transition from a single-modality surgical paradigm to a multimodal, biomarker-driven strategy, where systemic agents, optimised intraperitoneal delivery and precision diagnostics complement cytoreduction. The priority is high-quality, disease-specific clinical trials that can move the field beyond extrapolated evidence.
Conclusion
PMP exemplifies a rare but surgically curable peritoneal malignancy when approached with precision, discipline and multidisciplinary expertise. Over the past decade, the paradigm has shifted from palliative debulking to curative-intent CRS, with HIPEC remaining both a cornerstone and a controversy. Imaging pearls such as hepatic scalloping, MRI-based PCI precision and tumour marker integration have enhanced diagnostic confidence, while molecular insights, particularly KRAS and GNAS mutations, underscore the biological uniqueness of PMP and hint at future therapeutic targets.
Decision-making is anchored in the triad of disease burden, PCI, CC score and patient resilience, contextualised within the experience of high-volume centres. Although HIPEC protocols vary and their necessity is debated, especially in the wake of colorectal peritoneal metastasis trials, consensus remains that its potential benefit must be evaluated within disease-specific frameworks. Systemic chemotherapy offers only modest palliation, yet advances in molecular profiling, immunotherapy and novel intraperitoneal delivery systems are expanding the therapeutic horizon.
The road ahead will be defined by collaboration: harmonised registries, prospective PMP-specific trials and translational science to integrate molecular signatures into clinical care. For now, the optimal strategy remains meticulous patient selection, complete cytoreduction in specialised centres and thoughtful integration of intraperitoneal or systemic adjuncts. This review highlights that PMP is not merely a surgical disease but a model of multidisciplinary oncology, where biology, technology and clinical judgement converge.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Not applicable (narrative review).
Informed consent
Not applicable. No individual patient data, images, or identifiers have been included.
Credit author statement
Supreet Kumar: Concept, design, literature synthesis, drafting and final approval.
Aishwarya Bhalerao: Literature review, drafting sections and table preparation.
Suryalok Pratap Shah: Literature review, drafting sections and reference management.
Vivek Tandon: Critical revision for intellectual content and surgical perspective.
Deepak Govil: Senior oversight, critical revision and approval of final manuscript.
Data availability
Not applicable. This is a review article based on previously published studies; no new datasets were generated or analysed.
Use of artificial intelligence
The authors affirm that no generative artificial intelligence tools were used in the collection, analysis, or interpretation of data. Editorial assistance was limited to language polishing under direct author supervision, and the integrity of the content remains the responsibility of the authors.
Guarantor
Dr. Supreet Kumar accepts full responsibility for the integrity and accuracy of the content.