
Abstract
Cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) are the standard treatment for selected patients with peritoneal malignancy. The optimal means of assessing risk prior to these complex operations is not known. This study explored the associations between preoperative cardiopulmonary exercise testing (CPET) variables and postoperative outcomes following elective CRS and HIPEC. This study included patients who underwent routine preoperative CPET prior to elective CRS and HIPEC at Royal Prince Alfred Hospital in Sydney between July 2017 and July 2020. CPET was performed using a cycle ergometer and measured peak oxygen uptake (V
Keywords
Introduction
Once considered an incurable disease, peritoneal carcinomatosis is now amenable to macroscopic tumour excision combined with intraperitoneal chemotherapy. Pioneered by Sugarbaker in the 1990s, 1 cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) has become increasingly popular worldwide and is now the standard treatment for selected patients with peritoneal surface malignancies originating from the appendix, colon, rectum, ovary or mesothelium. 2
CRS is a complex procedure and presents a number of intraoperative challenges, including long procedure times, often multi-visceral surgical resections, significant blood loss and fluid shifts. HIPEC additionally causes systemic hyperthermia, increased oxygen consumption, raised intra-abdominal pressure, reduced respiratory compliance and cardiovascular stress. 3 Postoperative complications following CRS and HIPEC are common and reported to occur in up to two-thirds of patients, while mortality rates are reportedly between 0% and 9%. 4 The occurrence of postoperative complications following abdominal surgery is known to correlate with length of hospital stay, healthcare utility and cost and, in some patients, failure to reach further intended cancer treatments.5,6 Also of concern is the association between postoperative complications and reduced long-term survival. 7
Functional capacity is an important part of preoperative risk assessment. Cardiopulmonary exercise testing (CPET) is the gold standard assessment of functional capacity 8 and has been used extensively in intra-abdominal surgery to evaluate preoperative cardiopulmonary fitness objectively, predict postoperative outcomes and augment individualised risk assessment. 9 Values derived from CPET have been shown to predict outcomes in a number of intra-abdominal operations, including liver transplantation, liver resection, pancreatic surgery and abdominal aortic aneurysm repair. 10 It is postulated that increased physical fitness enables patients to withstand postoperative systemic stress better, while regular physical activity might also confer beneficial ischaemic preconditioning-type effects. 10
Oxygen consumption measured at the anaerobic threshold (AT) and peak exercise (V
Despite extensive experience of using CPET in intra-abdominal surgery, a recent systematic review of CPET-derived variables prior to cancer surgery found there were no existing studies reporting associations between preoperative CPET performance and outcomes following CRS and HIPEC. 11 Given the significant impact of CRS and HIPEC, including high rates of postoperative complications, reduced quality of life and heavy resource consumption, 15 evaluation of the role of CPET in this patient group is specifically warranted. It is hypothesised that predictive values derived from optimal CPET cut points can be used to prognosticate complications following CRS and HIPEC and therefore improve individualised risk assessment prior to surgery. Moreover, CPET-derived variables might identify modifiable risk and allow implementation of proactive measures to reduce the rate of complications and better deliver value-based healthcare. The primary aim of this study therefore was to evaluate the association between preoperative CPET variables and in-hospital morbidity following CRS and HIPEC.
Methods
This was a prospective observational study conducted at Royal Prince Alfred Hospital (RPAH) in Sydney, Australia, between July 2017 and July 2020. The study was registered in June 2017 and ethics approval was granted by Sydney Local Health District Human Research Ethics Committee (Protocol No. 17-0097 and HREC/17/RPAH/143).
Participants
Patients were included in this study if they were (a) aged ≥18 years, (b) scheduled to undergo CRS and HIPEC at RPAH and (c) underwent preoperative cardiopulmonary exercise testing. Patients were excluded if any of the following applied: (a) underwent non-elective CRS and HIPEC, (b) underwent CRS without HIPEC, (c) underwent a surgical procedure other than CRS and HIPEC, (d) failed to provide consent to undergo CPET, (e) physically unable to perform CPET on a cycle ergometer, (f) failed to achieve an AT or (g) contraindication to CPET as per the American Thoracic Society/American College of Chest Physicians (ATS/ACCP) statement.
All patients with peritoneal malignancy considered for CRS and HIPEC at RPAH were discussed at the Advanced Gastrointestinal Surgical Program multidisciplinary meeting prior to surgery, including evaluation of patient history, physical examination, tumour markers, cross-sectional imaging (contrast-enhanced computed tomography and positron emission tomography) and, where relevant, laparoscopy findings. Patients deemed appropriate surgical candidates for CRS and HIPEC subsequently underwent further preoperative assessment by a specialist anaesthetist at an outpatient clinic, typically two to four weeks prior to planned surgery. All patients had routine bloods collected prior to surgery, namely full blood count, renal and liver function biochemistry, group and hold, and coagulation profile. A 12-lead electrocardiogram (ECG) was also performed. If time permitted (generally at least one week before scheduled surgery), patients were referred for outpatient CPET at the Department of Respiratory Medicine. Referral for CPET was made routinely and was not based on the medical status of the patient or perceived functional capacity. Patients were provided with an information leaflet on the role of CPET with respect to their surgery, and they were given an opportunity to ask questions as well as to decline testing. Other preoperative specialist referrals, and investigations such as echocardiography, were organised at the discretion of the anaesthetist, based on history and examination. CPET results did not singularly alter preoperative management, but detection of very low functional status or suspected cardiac ischaemia was further discussed at a multidisciplinary meeting.
Cardiopulmonary exercise testing
CPET was typically performed within two weeks of planned surgery on a computer-controlled electromagnetically braked cycle ergometer (Ergoline ergoselect5; Ergoline, Bitz, Germany) in accordance with the ATS/ACCP statement. 16 Breath-by-breath analysis of expired gas was measured via metabolic cart (Ultima Cardio2; MGC Diagnostics, St. Paul, MN, USA). A 12-lead ECG and oximetry were measured throughout the test, and non-invasive blood pressure was recorded every two minutes. All tests were supervised by a medical officer, with resuscitation equipment immediately available. Before each CPET, flow and gas calibrations were performed, and patients performed resting spirometry.
Ramped exercise was calculated for each patient based on a modified protocol from Jones et al. 17 to yield a ramped phase intended to last six to ten minutes. Patients were advised to maintain a pedal speed of 60 revolutions per minute, displayed electronically on the cycle ergometer. There were four phases to each CPET: (a) rest lasting two minutes, (b) freewheeling lasting two minutes, (c) ramped exercise lasting six to ten minutes and (d) recovery lasting five minutes. The test was terminated once volitional symptom limitation was reached. Self-perceived exhaustion was recorded using the Borg scale, recorded separately for leg heaviness and shortness of breath.
For this study, oxygen consumption at the AT and V
Surgery
Surgery was performed through an extended midline laparotomy. The burden of disease was calculated based on the peritoneal cancer index (PCI) system. Parietal peritonectomy was performed with or without visceral resections, depending on the origin and extent of disease, and variably included colonic and small bowel resections, splenectomy, cholecystectomy, partial gastrectomy, and hysterectomy with bilateral salpingo-oophorectomy in female patients. HIPEC was performed following cytoreduction and involved delivery of chemotherapy via crystalloid perfusate circulated throughout the abdominal cavity at 42°C using an extracorporeal roller pump (HT2000, ThermoChem; ThermaSolutions, Inc., White Bear Lake, MN, USA). The most commonly used chemotherapy regimen was mitomycin C at a dose of 15 mg/m2 circulated for 60 minutes. A completeness of cytoreduction (CC) score was reported at the time of surgery, and this was used to indicate the volume of residual disease. All patients were routinely admitted to the intensive care unit (ICU) immediately postoperatively.
Outcome measures
Occurrence of any postoperative in-hospital complication in the index admission for surgery was the primary outcome of this study. All postoperative complications were reported according to the Clavien–Dindo classification of surgical complications 18 and recorded at the time of hospital discharge. Clavien–Dindo Grades I and II are classified as minor complications, while Grades III–V are classified as major complications. Based on Clavien–Dindo classes, the comprehensive complication index (CCI) was also reported, calculated as the sum of each patient’s complications weighted for severity. CCI yields a continuous scale of increasing severity from 0 to 100, with 0 representing no complication. 19 Secondary outcomes of this study were length of ICU stay and length of hospital stay. To calculate the total duration of ICU stay, the day of surgery was defined as day 0. The median length of ICU stay for this cohort was four days. Therefore, for the purposes of data analysis, length of ICU stay was divided into short (<5 days) and long (≥5 days). To calculate the total duration of hospital inpatient stay, the day of surgery was defined as day 0. The median length of hospital stay was 16 days. The length of hospital stay was therefore divided into short (<16 days) and long (≥16 days). A number of covariates are additionally reported for each patient, including patient characteristics (age, sex, primary tumour) and intraoperative characteristics (length of surgery, PCI, CC, blood loss, and requirement for any blood transfusion).
Statistical analyses
All statistical analyses were conducted in IBM SPSS Statistics for Windows v25 (IBM Corp., Armonk, NY, USA). Patients’ characteristics and surgical outcomes are presented descriptively. Categorical variables are presented as frequency (percentage), and continuous variables as mean (standard deviation (SD)). Univariate logistic regression was used to investigate the association between preoperative CPET variables and postoperative outcomes. The existing literature has reported optimal discriminatory cut points for patients scheduled to undergo intra-abdominal surgery, with AT of 10 ml/kg/min and 11 ml/kg/min most commonly reported.10,13 We therefore explored the association between postoperative complications and incremental aerobic fitness based on predetermined AT cut points using bivariate logistic regression. A multivariate analysis was also performed for these same cut points, adjusting for age (years), sex (male/female), type of cancer (pseudomyxoma peritoneii/appendix adenocarcinoma/colorectal/ovarian/peritoneal mesothelioma/small bowel adenocarcinoma/other), preoperative chemotherapy (yes/no) and PCI (score). The discriminatory value of CPET variables was assessed using area under the curve (AUC) of the receiver operating characteristic (ROC) curve. A P-value of less than 0.05 was considered statistically significant for all analyses.
Results
Patient characteristics
Between July 2017 and July 2020, 178 patients were scheduled for CRS and HIPEC. A total of 131 patients underwent preoperative CPET, 129 of whom were included in the data analysis (Figure 1). The commonest reason for failure to perform CPET was insufficient time for referral for CPET between multidisciplinary discussion and scheduled surgery. Within the study period, there were no significant differences in the characteristics of patients who performed preoperative CPET and those who did not, except the studied cohort was older (mean (SD) 56 (12.5) years versus 51.5 (16.2) years, P = 0.045.
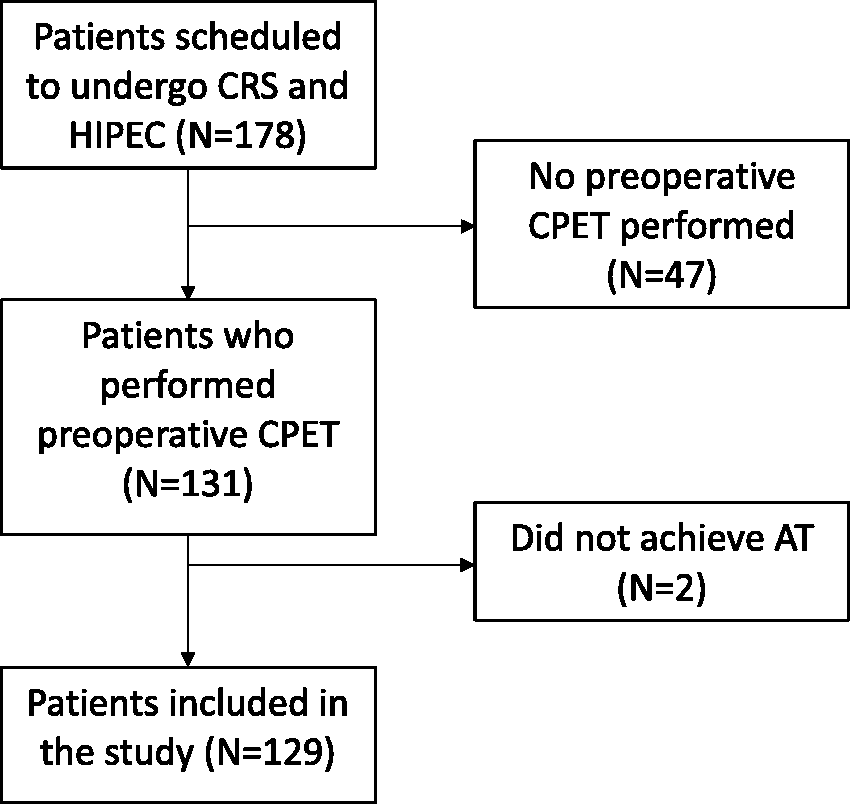
Study flow diagram. CRS: cytoreductive surgery; HIPEC: hyperthermic intraperitoneal chemotherapy; CPET: cardiopulmonary exercise testing; AT: anaerobic threshold.
Patient characteristics are summarised in Table 1. The mean age of included patients was 56 years (SD 12.5 years), and 51.2% of patients were male. The most common tumours were those of colorectal or appendiceal origin, with 41.1% of patients undergoing CRS and HIPEC for colorectal cancer, 20.9% for pseudomyxoma peritoneii and 20.2% for appendiceal adenocarcinoma.
Characteristics of the included patients.
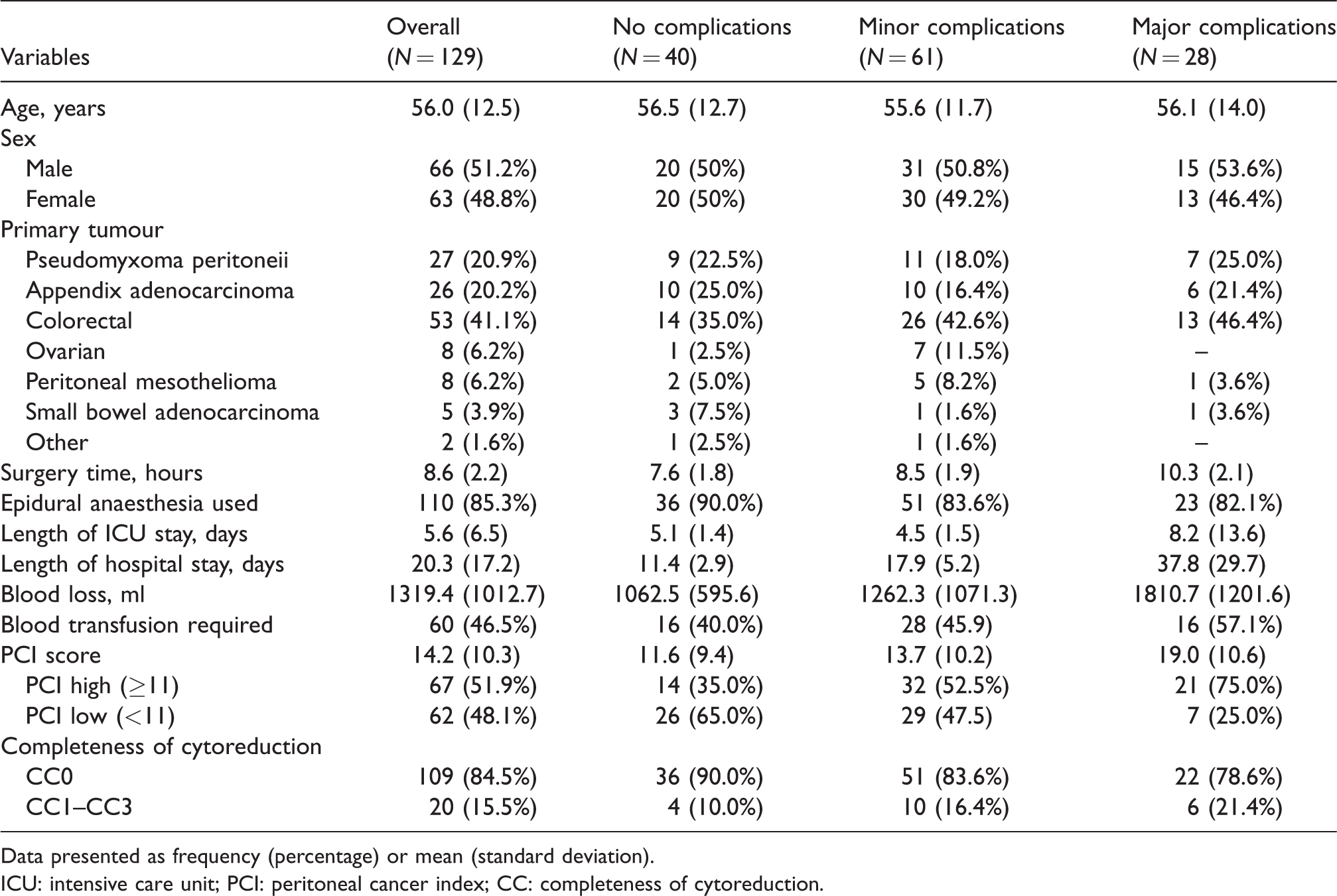
Data presented as frequency (percentage) or mean (standard deviation).
ICU: intensive care unit; PCI: peritoneal cancer index; CC: completeness of cytoreduction.
Intraoperative characteristics
The mean duration of surgery was 8.6 hours (SD 2.2 hours). The mean PCI was 14.2 (SD 10.3), while complete cytoreduction, defined as CC0, was achieved in 84.5% of patients. Mean intraoperative blood loss was 1319 ml (SD 1012 ml), and blood transfusion was required in almost half of patients at the time of surgery.
Length of stay
The mean length of intensive care stay was 5.6 days (SD 6.5 days), and the mean hospital stay was 20.3 days (SD 17.2 days). Of the 129 patients, 41.9% had a short ICU stay, and 46.5% had a short hospital stay.
Postoperative complications
Postoperative complications occurred in 89 (69%) patients. According to Clavien–Dindo classification, 61 (47.3%) patients had a minor (Class I–II) complication, and 28 (21.7%) patients had a major (Class III–V) complication. Two (1.6%) patients died in hospital following surgery: one on the first postoperative day due to overwhelming systemic inflammation and multi-organ failure, and the other on day 61 due to complex intra-abdominal sepsis. The mean CCI for the entire cohort was 20.7 (SD 20.6), and in those with at least one recorded complication, the mean CCI was 29.9 (SD 18.4). Complications by Clavien–Dindo class and CCI are shown in Table 2.
Morbidity as per Clavien–Dindo class and CCI.
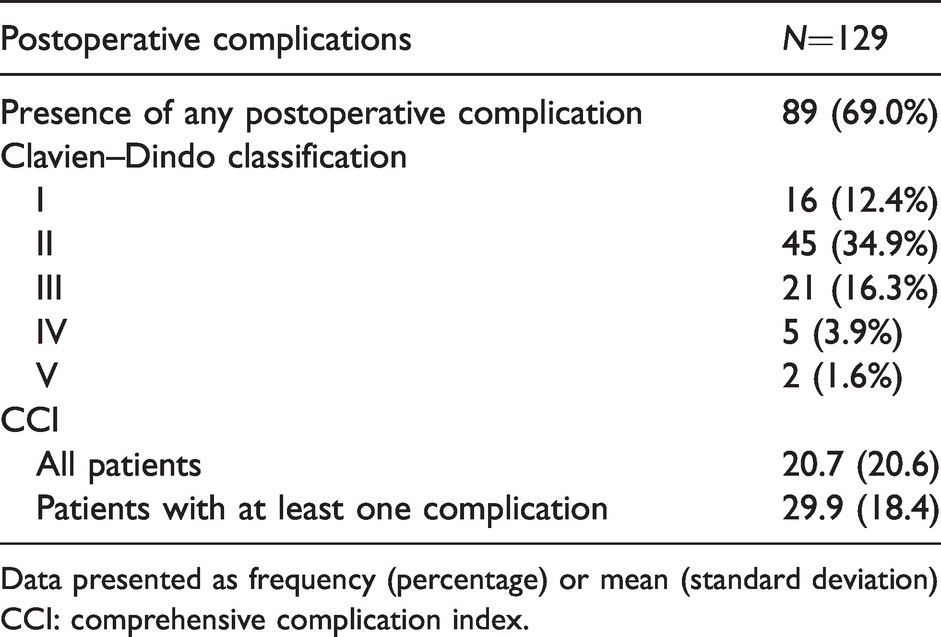
Data presented as frequency (percentage) or mean (standard deviation)
CCI: comprehensive complication index.
Cardiopulmonary exercise testing data
There were no complications recorded during performance of CPET. The mean AT was 14.0 ml/kg/min (SD 4.0 ml/kg/min), and the mean VO2 peak was 21.1 ml/kg/min (SD 5.3 ml/kg/min). Two patients performed insufficient work to achieve an AT and were excluded from data analysis.
Cardiopulmonary exercise testing variables and postoperative outcomes
Complications
The mean (SD) AT in patients with any postoperative complication was 13.5 (3.8) ml/kg/min compared 15.3 (4.2) ml/kg/min in those without complications (P = 0.015; Figure 2). Likewise, the mean mean (SD) V
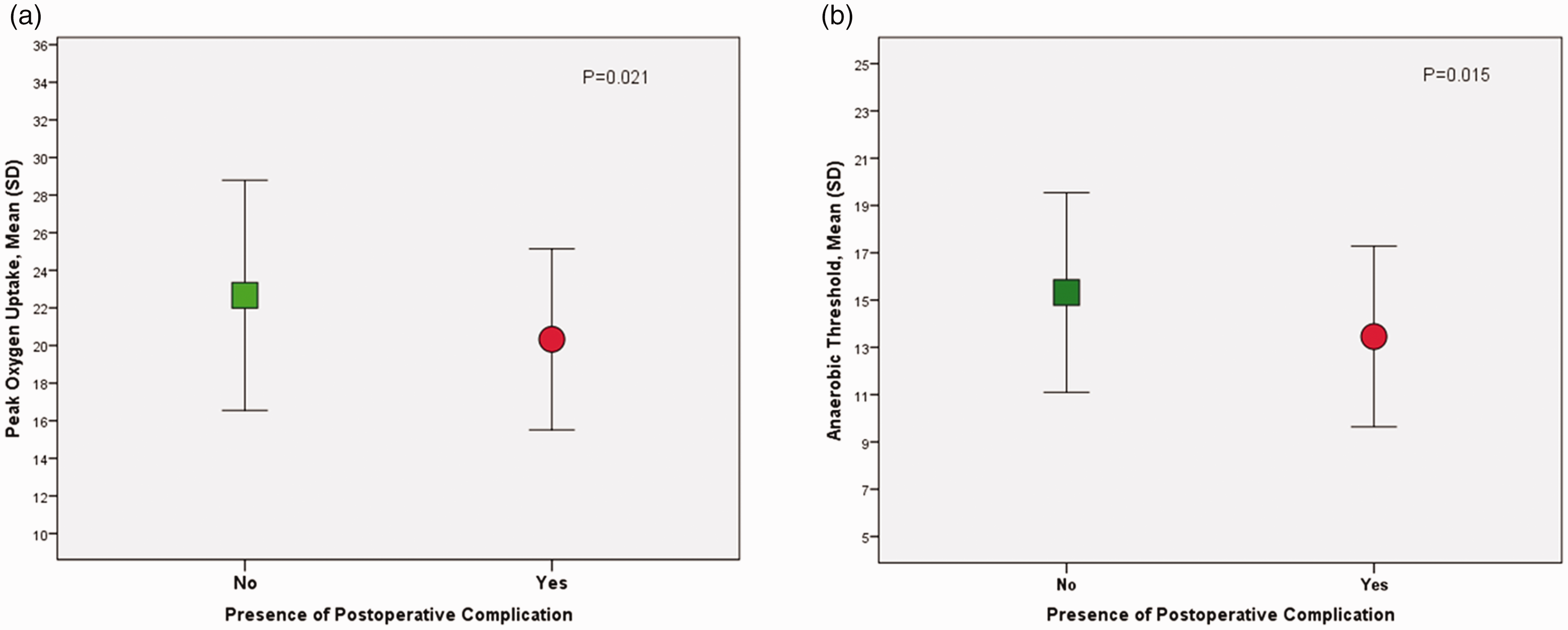
Cardiopulmonary exercise testing variables (ml/kg/min) and presence of any postoperative complication (N=129). SD: standard deviation.
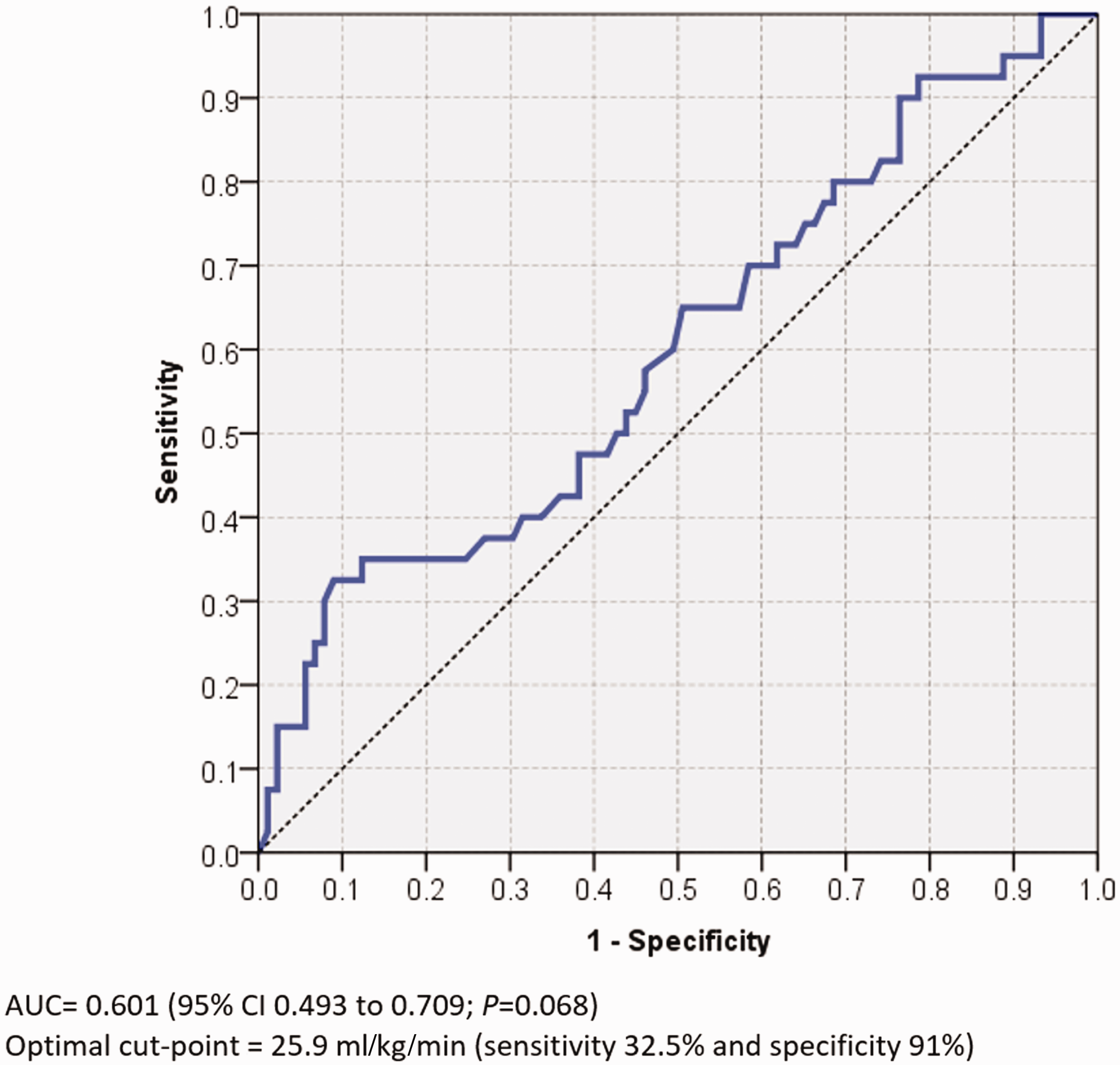
ROC curve for V
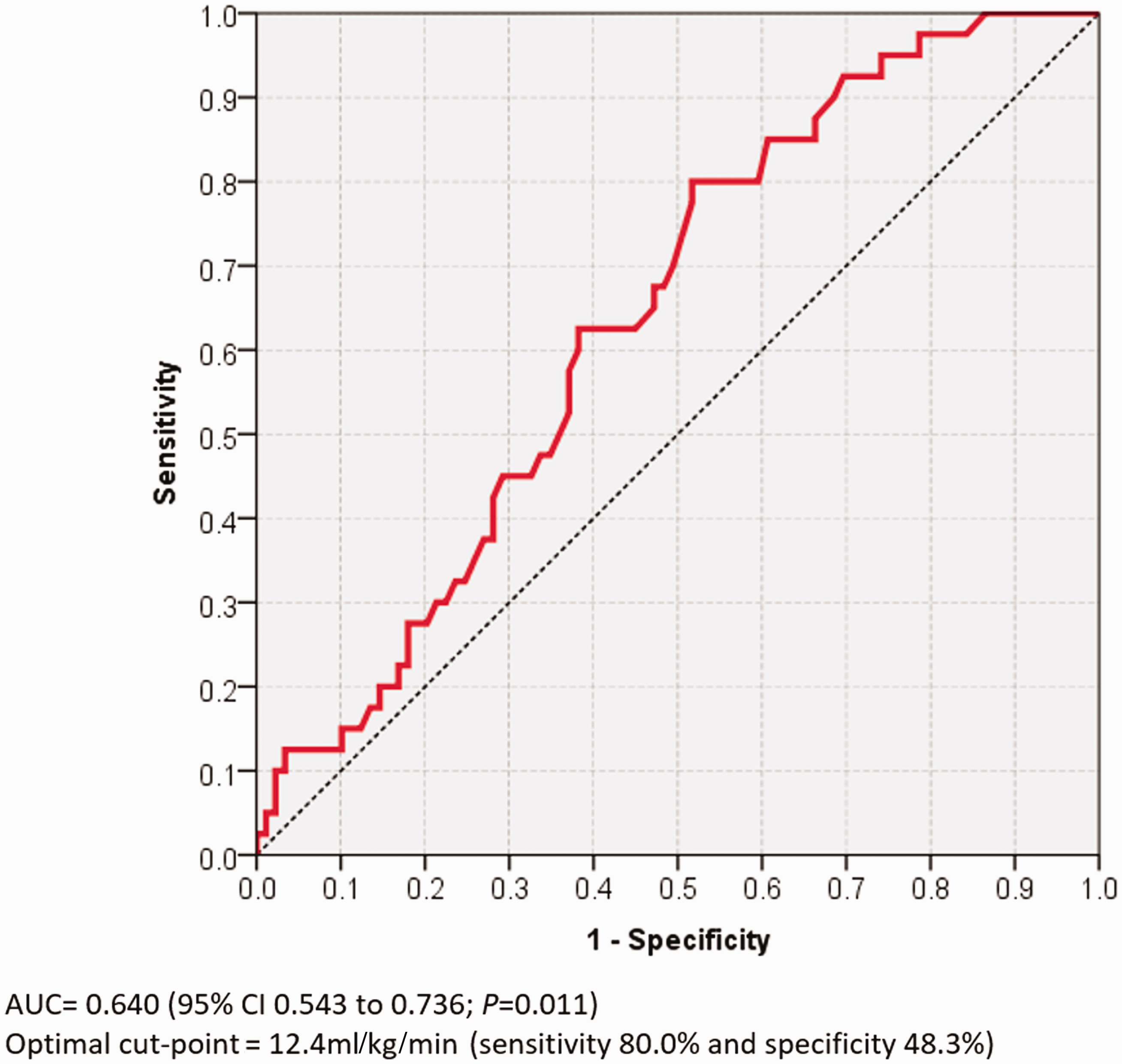
Receiver operating characteristic curve for anaerobic threshold versus presence of any complication. AUC: area under the curve; CI: confidence intervals.
Based on existing discriminatory AT cut points, failure to exceed 11 ml/kg/min was associated with increased odds (odds ratio (OR) 3.6; 95% CI 1.29 to 10.16; P = 0.016)) for developing a postoperative complication compared to those whose AT exceeded 11 ml/kg/min, while failure to exceed 10 ml/kg/min was associated with an OR of 6.2 (95% CI 1.39 to 28.0; P = 0.017) for developing a postoperative complication compared to patients whose AT exceeded this value. We further explored the associations between increasing aerobic fitness and postoperative complications (Table 3). A multivariate analysis was performed adjusting for age, sex, type of cancer, preoperative neoadjuvant chemotherapy and PCI (Table 3). In both models, increased exercise capacity was associated with reduced odds of a complication at predetermined AT cut points. In this cohort, based on AUC, the optimal cut point for AT was 12.4 ml/kg/min, giving a sensitivity of 80.0% and a specificity of 48.3% and a positive predictive value (PPV) of 89.3% and negative predictive value (NPV) of 31.0%.
Association between preoperative anaerobic threshold cut points (ml/kg/min) and presence of any postoperative complication.
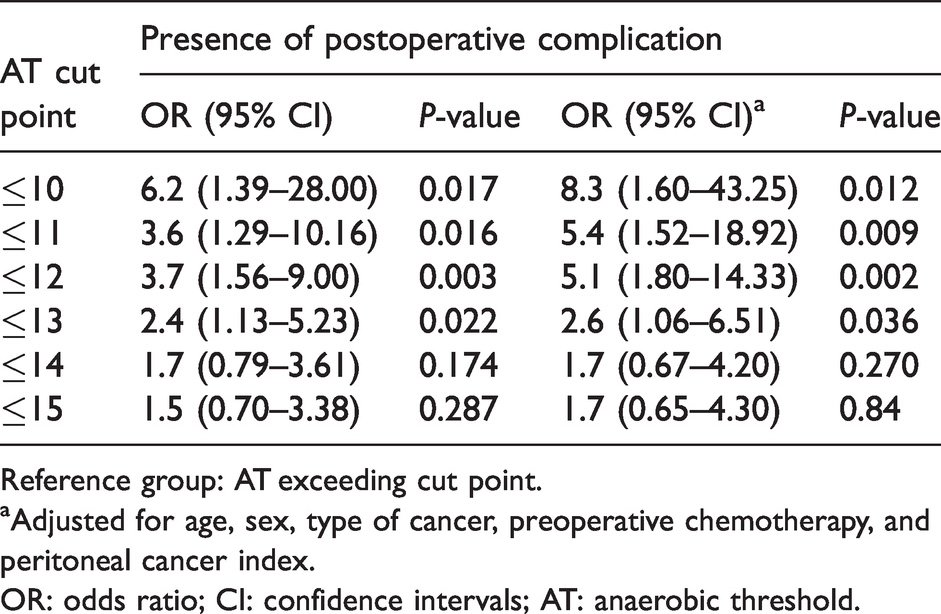
Reference group: AT exceeding cut point.
aAdjusted for age, sex, type of cancer, preoperative chemotherapy, and peritoneal cancer index.
OR: odds ratio; CI: confidence intervals; AT: anaerobic threshold.
Length of stay
The mean (SD) AT in patients with a long hospital stay was 13.3 (3.6) ml/kg/min compared to 14.9 (4.3) ml/kg/min for those who had a short hospital stay (P = 0.021; Figure 5). The mean (SD) V
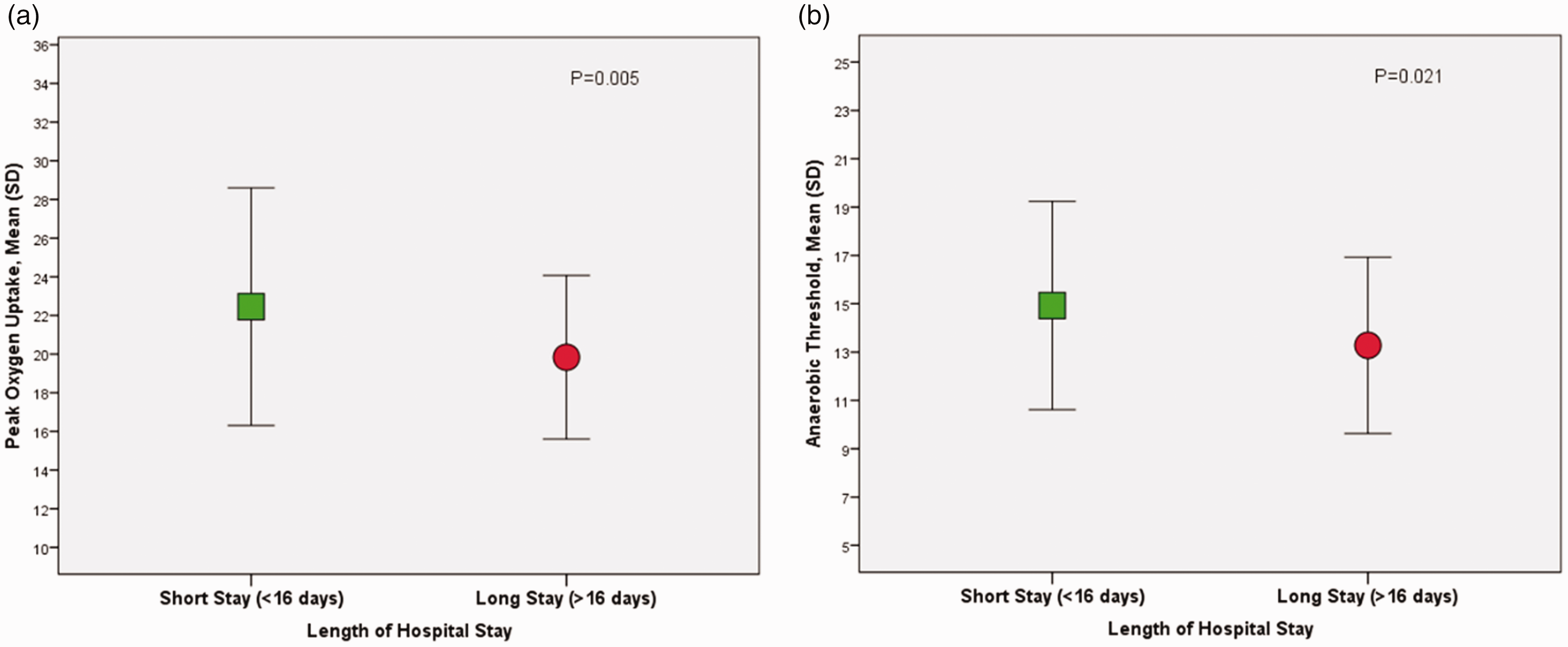
CPET variables (mL/kg/min) and length of hospital stay (N=129).
Discussion
The main finding is that CPET-derived exercise capacity (AT and V
Increasingly CPET variables are used at our hospital to identify a target group for prehabilitation interventions. A structured preoperative exercise programme before CRS and HIPEC has been shown to be feasible and acceptable to patients with peritoneal malignancies, 20 and its ability to reduce postoperative complications in major abdominal cancer surgery, including CRS and HIPEC, is currently being assessed in our patient population. Furthermore, of patients who undergo CRS and HIPEC, almost half receive preoperative neoadjuvant cancer treatments, 2 which are known to acutely reduce cardiopulmonary fitness, 21 and prehabilitation might serve to ameliorate this decline in exercise capacity. While duration of ICU stay was not associated with preoperative CPET variables, this might be explained by the preferential use of epidural catheters for postoperative analgesia, which obligates management in ICU in our institution and independently determines length of ICU stay.
This study adds to the existing literature supporting a discriminatory role for CPET in the risk assessment of patients undergoing major non-cardiac surgery. The largest such study to date, the METS study, reported that CPET-derived VO2 peak predicts moderate and severe postoperative complications, 14 but the range of operations did not meaningfully represent CRS and HIPEC, with only 33% of patients having intra-peritoneal surgery and 24% admitted to a monitored postoperative bed. The mean level of cardiorespiratory fitness in patients without complications in the current study is higher than previously reported values in major abdominal surgery,22,23 which could represent comparatively greater systemic stress following CRS and HIPEC, requiring increased exercise capacity to meet this challenge. This is further supported by the optimal AT cut point in the current study being higher than previously reported values in intra-abdominal surgery, with a systematic review of 35 studies reporting an optimal AT cut point <10.1 ml/kg/min with respect to postoperative morbidity. 10 In the current study, AT <10.1 ml/kg/min was associated with an OR of 6.2 (95% CI 1.39 to 28.0; P = 0.017) for any complication compared to patients whose AT exceeded this threshold.
Our study has a number of strengths. Despite differing primary pathologies, the operative approach was largely homogeneous, and all patients received HIPEC. In addition, all patients received invasive intraoperative haemodynamic monitoring (arterial catheter and central venous catheter) and were routinely admitted to the ICU following surgery. The mean duration of ICU stay exceeded five days, reducing variability in early postoperative care. Furthermore, the current study was prospective in nature, and morbidity data were robustly recorded for the entire hospital stay. CPET methods and reporting were also consistent across all subjects, with all tests conducted in the same department and data reviewed independently by the same clinicians.
Potential weaknesses are its single-centre design, which may limit the generalisability of our findings to other centres undertaking these operations, particularly with reference to optimal CPET-derived cut points, and lack of blinding of the treating team to CPET results (including surgeon, anaesthetist and intensive care staff). That said, any risk reduction strategies employed in patients with low cardiorespiratory fitness would likely increase the discriminatory value of CPET. The AUC of the ROC curves displayed poor test discrimination. Nonetheless, values for AUC observed in the current study are consistent with existing studies, particularly in univariate models.22–24 The predictive value of other commonly used preoperative tests, for example biomarkers and risk calculators, are not known in this population, which makes it difficult to evaluate the incremental discrimination of CPET above other risk assessment tools. A further limitation is failure to explore the prognostic value of other CPET-derived variables, particularly ventilatory equivalent for CO2 (V
Data in this study support the role of CPET as a non-invasive adjunct to preoperative cardiorespiratory fitness more objectively measure and to improve risk assessment of complications in patients scheduled for CRS and HIPEC. While the optimal means of assessing patient risk prior to CRS and HIPEC is not known, in patients with peritoneal malignancy, CPET data can augment the processes of risk assessment, informed consent and collaborative decision-making.
Footnotes
Author Contribution(s)
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.