
Abstract
Background and Objectives:
Tumours of the salivary gland are rare, accounting for 2%–6% of all head and neck cancers. To provide data for comparison with epidemiological studies from different geographic regions and ethnic groups, this research intends to assess the incidence and distribution of salivary gland cancers within an Indian cohort.
Methodology:
We retrospectively collected data on the distribution and histopathological characteristics of salivary gland neoplasms diagnosed in the Department of Histopathology, Apollo Hospitals, Chennai, between June 2014 and June 2024. Pathological findings and demographic data for all cases were retrieved from the laboratory information system.
Results:
Out of 631 patients, 75% (n = 473) were identified as benign, while 25% (n = 158) were classified as malignant. The average age of patients was 44.9 ± 15.3 years. There was a slight male predominance, with a male-to-female ratio of approximately 5.3:4.7. Parotid gland was the most frequently affected site, comprising 68.6% of the tumours, followed by minor salivary glands (18.5%), submandibular gland (11.9%) and sublingual gland (1%). One patient presented with a bilateral tumour and 2.7% were recurrent tumours.
Conclusion:
This study represents one of the largest investigations of primary salivary gland tumours in India, providing comprehensive insights into salivary gland tumours neoplasms in our region. Additionally, gathering epidemiological data on these tumours from various regions worldwide can deepen our understanding of their biology and clinical features.
Keywords
Introduction
Neoplasms of the salivary gland consist of a diverse group of tumours that arise from the epithelial and mesenchymal components of the salivary glands. They are rare, accounting for 2%–6% of head and neck tumours in the literature.[1–3] The estimated global incidence rate ranges from 0.4 to 13.5 cases per 100,000 annually.[1] These neoplasms vary significantly in their histological characteristics, clinical behaviour and prognosis. Understanding the pathology of salivary gland neoplasms is essential for accurately diagnosing, treating and managing these tumours. Salivary gland tumours are classified into benign and malignant categories, with a majority being benign. According to the World Health Organisation (WHO) classification, more than 30 distinct types of salivary gland neoplasms exist, each with unique histological features.[2] The most common benign tumour is the pleomorphic adenoma, which typically occurs in the parotid gland. Malignant tumours, though less common, include mucoepidermoid carcinoma, adenoid cystic carcinoma (AdCC) and acinic cell carcinoma (ACC), among others.[3]
While numerous studies have examined the incidence and histological types of salivary gland tumours in the United States, Europe, Brazil, Jordan and Nigeria, there is limited information regarding their presentation patterns in Asian countries.[4–8] To provide data for comparison with epidemiological studies from different geographic regions and ethnic groups, this study sought to assess the incidence and distribution of salivary gland cancers within an Indian cohort.
Material and Methods
This was a retrospective study on salivary gland neoplasms diagnosed in the Department of Histopathology at Apollo Hospitals, Chennai, between June 2014 and June 2014, with approval from the Institutional Ethics Committee. It included cases from patients treated at the hospital as well as specimens referred from other institutions. Cytology cases were not part of the study. The tissue was fixed in 10% neutral buffered formalin, processed, paraffin-embedded and 4μ sections were cut and stained with haematoxylin and eosin (H and E) and if required, stained with periodic acid-Schiff and mucicarmine stains. All the cases were classified based on morphology and diagnoses were made according to the WHO 2022 histological classification of salivary gland tumours. Staging for the neoplasms was created using the College of American Pathologists protocol.
The pathological findings and clinical data of all cases were retrieved from the laboratory information system. Data entry was done using Microsoft Excel. Summary statistics were presented with mean ± SD and frequency (percentage) for the continuous and categorical factors, respectively. Analysis of variance (ANOVA) or Kruskal–Wallis test was used to assess significant differences in age across diagnostic groups. Chi-square or Fisher’s exact test was used to determine the association between two independent categorical factors. Statistical analysis was carried out by using statistical package for social sciences (SPSS) (IBM, 28.0).
Results
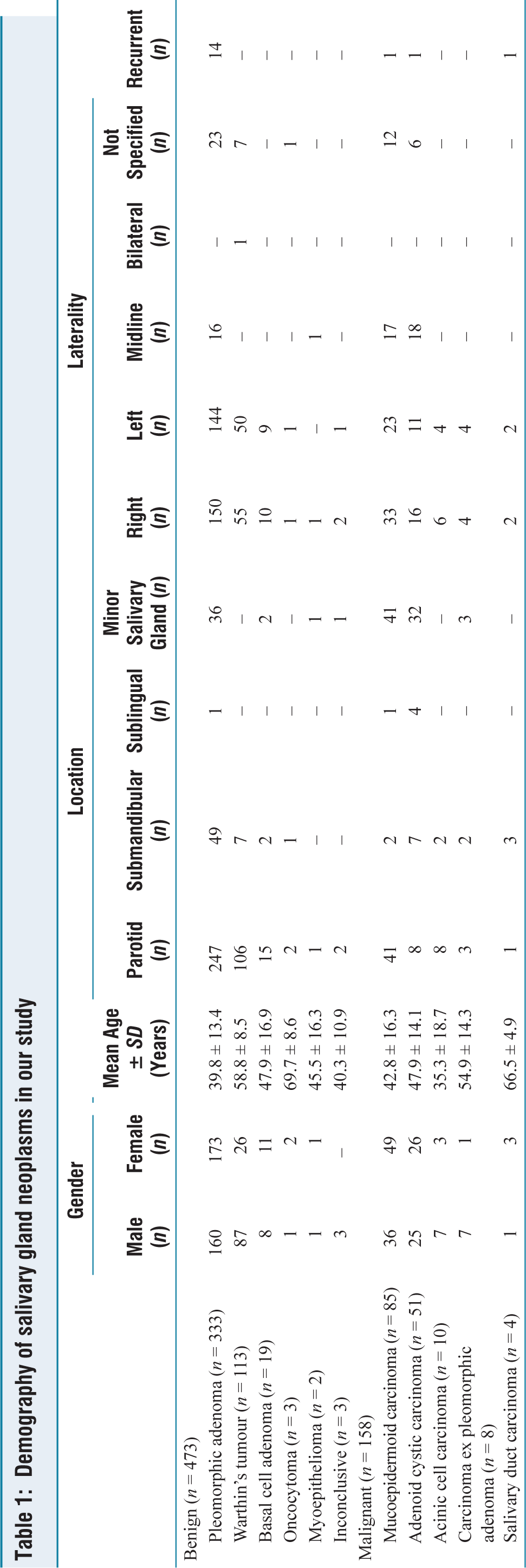
During the study period, a total of 296,740 biopsy specimens were collected. Among these, salivary gland tumours represented a small fraction, accounting for just 0.2% (n = 631). Of these tumours, 75% (n = 473) were identified as benign, while 25% (n = 158) were classified as malignant, resulting in a benign-to-malignant ratio of 3:1. The average age of patients diagnosed with salivary gland neoplasms was 44.9 ± 15.3 years. There was a slight male predominance, with a male-to-female ratio of approximately 5.3:4.7. Regarding the location, the parotid gland was the most frequently affected site, comprising 68.6% (n = 433) of the tumours, followed by minor salivary glands at 18.5% (n = 117), the submandibular gland at 11.9% (n = 75) and the sublingual gland at 1% (n = 6). In terms of laterality, 44.4% (n = 280) were found on the right side, 39.5% (n = 249) on the left, with one patient (0.2%) having a bilateral tumour and 8.2% (52 cases) located in the midline [Table 1 and Figure 1].
Demography of salivary gland neoplasms in our study
Benign Cases
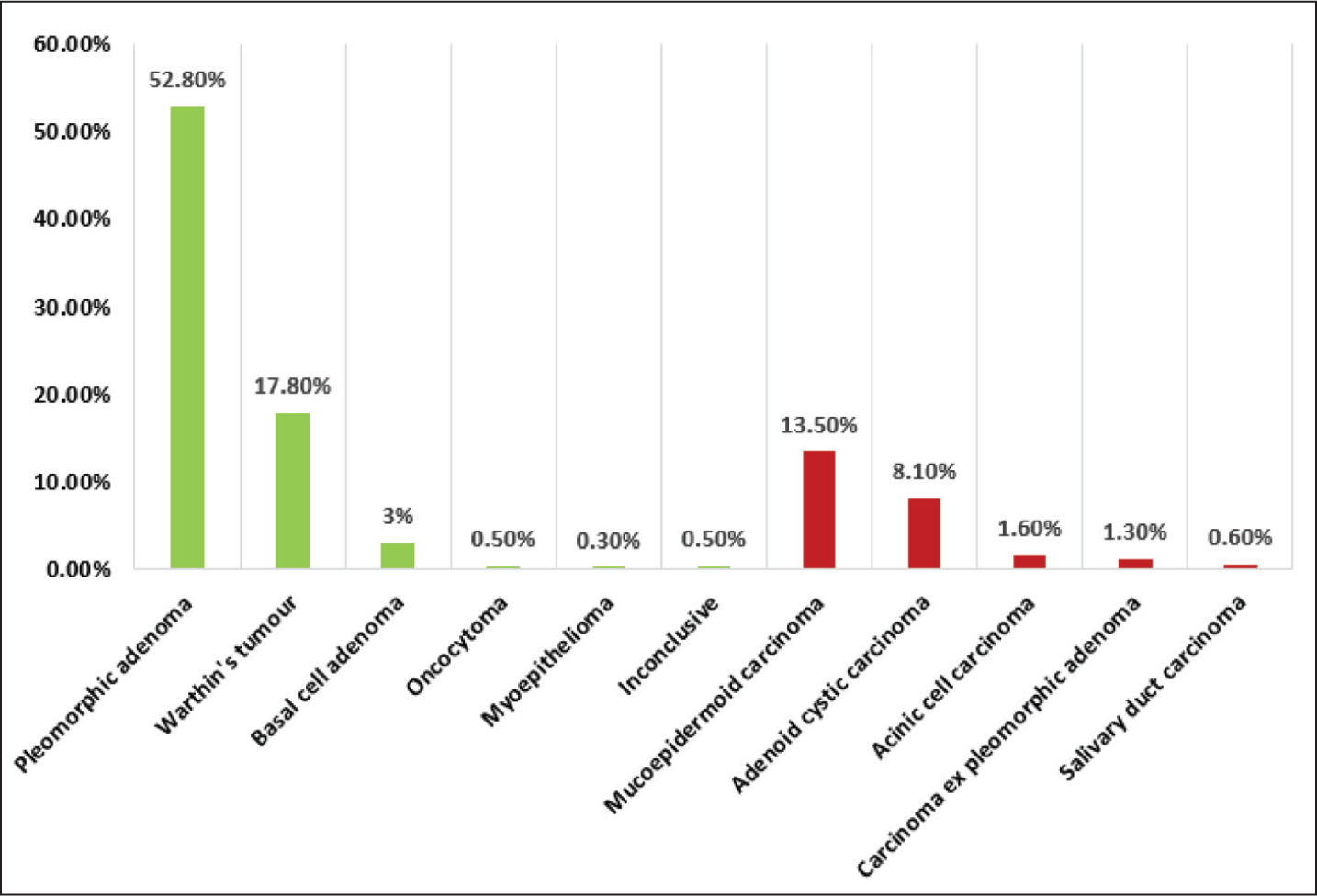
Among the 473 benign cases reported, pleomorphic adenoma was the most common diagnosis, accounting for 52.8% (n = 333). Other benign tumours included Warthin’s tumour at 17.9% (n = 113), basal cell adenoma at 3% (n = 19), oncocytoma at 0.5% (n = 3), myoepithelioma at 0.3% (n = 2) and inconclusive at 0.6% (n = 3) [Figure 2].
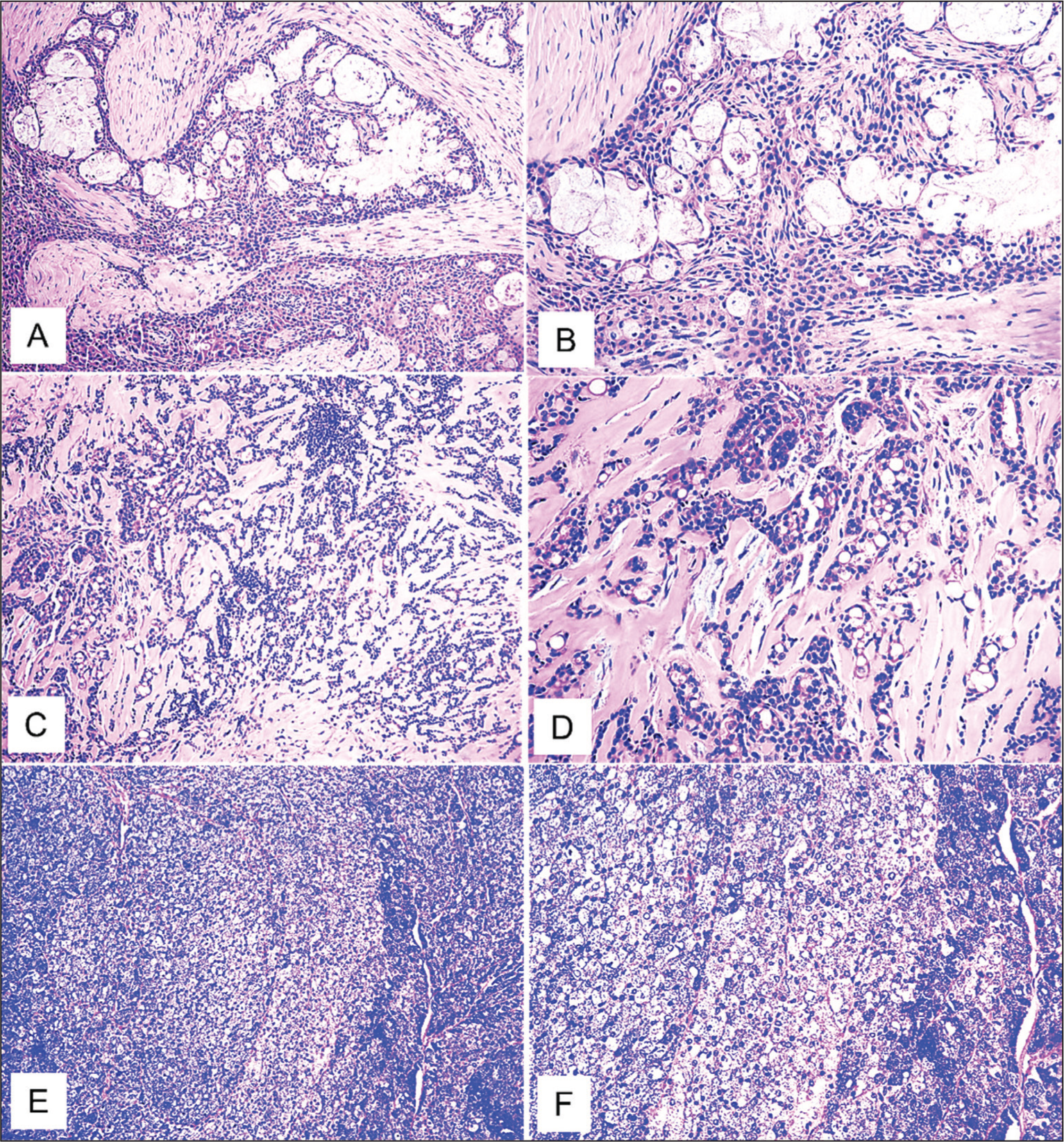
(H and E): A(100X) and B(200X), pleomorphic adenoma; C(100X) and D(200X), Warthin tumour; E(100X) and F(200X), basal cell adenoma
In patients with pleomorphic adenoma (n = 333), the average age at diagnosis was 39.8 ± 13.4 years. This group showed a slight female predominance, with a male-to-female ratio of approximately 4.78:5.88. Regarding tumour location, 74.2% (n = 247) were found in the parotid gland, 14.7% (n = 49) in the submandibular gland and 10.8% (n = 36) in minor salivary glands, with one case located in the sublingual gland (0.3%). In terms of laterality, 45% (n = 150) were right-sided, 43.2% (n = 144) were left-sided, 4.8% (n = 16) were midline and 6.9% (n = 23) the laterality was not specified. Among these cases, 4.2% (n = 14) were recurrent, with 13 of these occurring in the parotid gland, one in the palate and three cases presenting as multifocal tumours.
Warthin’s tumour represented 17.9% (n = 113) of the benign tumours, with a male-to-female ratio of 8.7:2.6, demonstrating a higher male predominance. The average age at diagnosis was 58.8 ± 8.5 years, indicating that these tumours tend to occur in older age groups. The vast majority of Warthin’s tumours were found in the parotid gland, accounting for 93.8% (n = 106), while 6.2% (n = 7) were located in the submandibular gland. In terms of laterality, 48.7% (n = 55) were right-sided, 44.2% (n = 50) were left-sided and 6.2% (n = 7); the laterality was not specified. Notably, there was one patient with bilateral parotid tumours and another presented with multifocal tumours within the parotid gland.
Basal cell adenoma accounted for 3% (n = 19) of the benign tumours, with a mean age at presentation of 47.9 ± 16.9 years. A slight female predominance was seen, with a male-to-female ratio of approximately 2.4:3.7. The majority of basal cell adenomas were found in the parotid gland, making up 79% (n = 15). The remaining tumours were located in the submandibular and minor salivary glands, each accounting for 10.5% (n = 2). Regarding laterality, 52.6% (n = 10) were right-sided, while 47.4% (n = 9) were left-sided.
Three cases of oncocytoma were reported, with a mean age of 69.7 ± 8.6 years. Among these, two patients were female, both having tumours in the parotid gland, one on the right side and the laterality of the other unspecified. The third patient was male, with a tumour located in the left submandibular gland. Additionally, two cases of myoepithelioma were documented: One in a 34-year-old female patient in the hard palate and the other in a 57-year-old male patient in the right parotid gland.
There were three inconclusive cases: Two cases exhibited extensive cystic degeneration, making it difficult to differentiate between pleomorphic adenoma and basal cell adenoma. Additionally, there was a single case with a differential diagnosis of basal cell adenoma and myoepithelioma.
Malignant Cases
Of the 158 malignant cases reported, mucoepidermoid carcinoma was the most prevalent diagnosis, representing 53.8% (n = 85). Other malignant tumours included AdCC at 32.3% (n = 51), ACC at 6.3% (n = 10), carcinoma ex pleomorphic adenoma at 5.1% (n = 8) and salivary duct carcinoma at 2.5% (n = 4) [Figure 3].
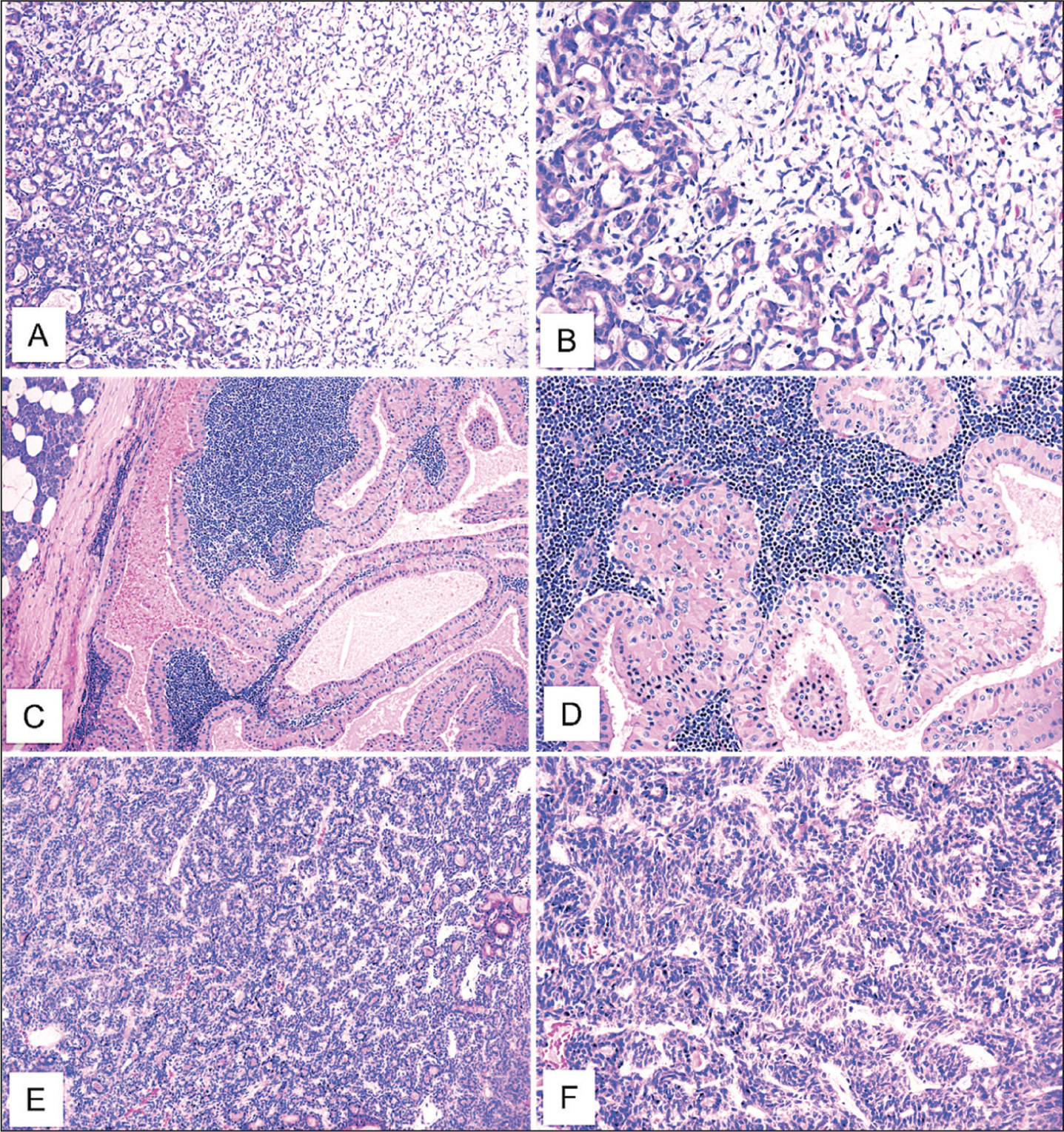
(H and E): A(100X) and B(200X), mucoepidermoid carcinoma; C(100X) and D(200X), AdCC; E(100X) and F(200X), ACC
In patients diagnosed with mucoepidermoid carcinoma (n = 85), the average age at diagnosis was 42.8 ± 16.3 years. This cohort displayed a slight female predominance, with a male-to-female ratio of approximately 3.6:4.9. Most tumours were in the parotid and minor salivary glands, each accounting for 25.9% (n = 41). Tumours in the submandibular gland represented 2.4% (n = 2), while those in the sublingual glands accounted for 1.2% (n = 1). Regarding laterality, 38.9% (n = 33) were right-sided, 27% (n = 23) were left-sided and 20% (n = 17) were midline; laterality was unspecified in 14.1% (n = 12) of cases. Among the midline tumours, 15.3% (n = 13) were found in the lower respiratory tract, including the bronchus and trachea. Additionally, one recurrent case was noted.
AdCC accounted for 32.3% (n = 51) of the malignant tumours, affecting both genders equally, with a male-to-female ratio of approximately 7.5:8.8. The average age at diagnosis was 47.9 ± 14.1 years. The majority of these tumours were found in the minor salivary glands, comprising 62.7% (n = 32), while 15.6% (n = 8) were located in the parotid gland, 13.7% (n = 7) in the submandibular gland and 7.8% (n = 4) in the sublingual gland. In terms of laterality, 31.4% (n = 16) were right-sided, 21.6% (n = 11) were left-sided and 35.3% (n = 18) were midline; laterality was unspecified for 11.8% (n = 6) of cases. Among the midline tumours, 23.5% (n = 12) were situated in the lower respiratory tract, including the bronchus and trachea. Additionally, one recurrent case was noted.
ACC accounted for 6.3% (n = 10) of the malignant tumours, with a mean age at presentation of 35.3 ± 18.7 years. A male predominance was observed, with a male-to-female ratio of approximately 2.1:1. The majority of ACCs were found in the parotid gland, comprising 80% (n = 8). In comparison, the remaining 20% (n = 2) were located in the submandibular gland. Regarding laterality, 60% (n = 6) were right-sided and 40% (n = 4) were left-sided.
Carcinoma ex pleomorphic adenoma accounted for 1.3% (n = 8) of the cases, with a mean age of 54.9 ± 14.3 years. A notable male predominance was observed, with a male-to-female ratio of approximately 2.1:0.3. The majority of tumours were found in the parotid and minor salivary glands, accounting for 37.5% (n = 3) and 25% (n = 2) in the submandibular gland, respectively. Additionally, 50% of the tumours were located on the right side and 50% on the left.
Four cases of salivary duct carcinoma were reported, with a mean age of 66.5 ± 4.9 years. Among these, three patients were female and one was male. Three tumours were located in the submandibular gland, while one, which was recurrent, was found in the parotid gland.
Additionally, one case of high-grade mucoepidermoid carcinoma was associated with Warthin’s tumour and another case of ACC presented alongside a pleomorphic adenoma.
Discussion
The salivary glands give rise to a diverse array of neoplasms and their histopathology is noted to be the most complex and varied. These tumours are rare, accounting for 2%–6% of all head and neck cancers.[1,9] Given their low incidence and the challenges in histological classification due to morphological overlap, epidemiological studies often have limited data to draw from. Studies have revealed regional variances in the incidence and prevalence of these neoplasms.[3,8,9]
Salivary gland tumours can occur in various locations, primarily within the major salivary glands, where most lesions are found. They can also develop in the minor salivary glands located in the palate, floor of the mouth, tongue, retromolar region and lips. In rare instances, these tumours may arise in the nasal cavity, larynx and lower respiratory tract. Additionally, tumours resembling salivary gland neoplasms can originate from lacrimal glands and adnexal structures. Heterotopic salivary tissue may lead to tumours in the mandible, thyroid and lymph nodes. Most tumours in the major salivary glands are benign, while those in the minor salivary glands are often malignant.[3,8,9] Hamid et al. and Bello et al. reported that the parotid gland accounts for 65%–70% of all salivary gland tumours, which aligns with our study findings, where it comprised 69% of the cases.[9,10] The submandibular gland accounts for 10%–15% of all salivary gland cancers, including both benign and malignant neoplasms, distributed evenly. Pleomorphic adenomas are the most predominant, accounting for 34%–36%.[10,11] Tumours in minor salivary glands are estimated to comprise up to 25% of all salivary gland tumours.[10–12] Most research on the demographics of salivary neoplasms has primarily focused on those occurring in either the major or minor salivary glands, with few studies accurately demonstrating the relative frequency of neoplasms across different gland types.[13]
Various factors, including radiation, smoking, trauma, viruses (Ebstein Barr virus [EBV], Human immunodeficiency virus [HIV]), immunosuppression, UV exposure, occupational hazards and genetic predispositions, have been linked to salivary gland neoplasms. Although tobacco and alcohol are not typically linked to most salivary tumours, a strong association exists between Warthin’s tumour and smoking. Genetic factors also play a key role: Pleomorphic Adenoma Gene 1 (PLGA1) and High Mobility Group AT-Hook 2 (HMGA2) are specific to pleomorphic adenoma, Myeloblastosis (MYB) mutations are linked to AdCC and MAML2 rearrangements to mucoepidermoid carcinoma. Studies indicate that 45%–50% of radiation-induced salivary gland tumours are pleomorphic adenomas, while mucoepidermoid carcinoma is the most common malignancy linked to radiation exposure.[14,15]
Clinically, salivary gland tumours often present as painless swellings in the affected glands, although malignant tumours may exhibit additional symptoms such as facial nerve involvement, pain or ulceration. Imaging techniques such as computerized tomography (CT), magnetic resonance imaging (MRI) or ultrasound are crucial to assess the size of the tumour and its connection to adjacent anatomical structures.[6]
Alsanie et al. conducted a multicentric study involving patients from all continents and found that, of the 5,739 cases, 65% were benign and 35% were malignant, similar to our findings.[8] Similarly, the study by Bello et al. on salivary gland neoplasms in patients from Finland and Israel reported a higher occurrence of benign tumours compared to malignant ones, with a ratio of 3:1, consistent with our study.[10] Bruzinga et al. found that the sixth decade of life was the most common age group affected by salivary gland tumours, while our study population exhibited a notably earlier incidence, with an average age of 44 years.[4] In the literature, benign tumours have been reported to occur more in younger and female patients, except Warthin tumours more common in males, in agreement with our findings. Malignant tumours are also seen mostly in elderly females, except for 70% of ACC in males and 90% of carcinoma ex pleomorphic adenoma in the male population in our study.[10]
Among benign salivary gland tumours, pleomorphic adenoma (70%) and Warthin tumour (24%) were the majority in our study, which is consistent with similar demographic studies.[4,8,9] Most benign tumours were found in the parotid gland (79%), followed by the submandibular glands (12.4%), which aligns with findings in global literature.[9,10]
In terms of malignant tumours, mucoepidermoid carcinoma (54%) was the most common, followed by AdCC (32%). While the literature lacks significant studies on the laterality of salivary gland tumours, our findings indicated that both benign and malignant tumours were predominantly right-sided. Additionally, AdCC was more commonly located in the midline (35%) and there was one case of bilateral Warthin tumour.
Complete surgical excision with negative margins is the cornerstone of treatment for benign salivary lesions; enucleation is associated with a higher risk of recurrence. Superficial parotidectomy is used for superficial lesions, while total parotidectomy is reserved for larger tumours.[16–18] Gland-preserving techniques, such as partial superficial parotidectomy and extracapsular dissection, reduce complications and improve quality of life. For benign salivary gland tumours of the palate, wide local excision with pseudo-capsule preservation is recommended, allowing for secondary healing or reconstruction. For malignant salivary gland tumours, additional therapies such as radiation therapy and chemotherapy may be indicated depending on the tumour type, stage and patient factors.[19] Ongoing research into the molecular underpinnings of these tumours promises to enhance our understanding and treatment options in the future. As with all neoplasms, early detection and appropriate intervention are key to improving patient outcomes.
The prognosis of salivary gland tumours varies by histology, with recurrence rates for pleomorphic adenoma ranging from 1% to 5% within 7–10 years, often due to incomplete excision.[17] Our study observed a similar trend, with a recurrence rate of 4.2% for pleomorphic adenoma. Warthin’s tumour has a recurrence rate of 7%–12% and can rarely transform into various carcinomas and it may be linked to lymphoproliferative disorders. Factors such as advanced age, higher tumour stage and distant metastasis, particularly to the lungs, are associated with a poor prognosis. Low-grade mucoepidermoid carcinoma (MEC) with the MECT1-MAML2 fusion has a favourable prognosis, while high-grade MEC and AdCC show poorer survival rates. ACC has a 5-year survival rate of 75%–96%, with survival influenced by factors such as tumour size and gender.[20,21]
Surgical excision may result in complications such as xerostomia and dental issues. Temporary facial nerve palsy occurs in 10%–65% of parotidectomy cases, with permanent paralysis in less than 5%.[22] Frey syndrome can develop in 2%–80% of patients treated with options such as botulinum toxin injections.[23] Radiation therapy may lead to hearing loss, chronic ear problems and rare cases of osteonecrosis and secondary malignancy.[24,25]
The limitations of our study include the lack of correlation between cytology cases and resections, as not all cases had cytology samples for meaningful comparison. Additionally, follow-up data and insufficient examination of surgical procedures and complications due to the unavailability of data in many cases were absent.
Conclusion
The study aims to assess the frequency and distribution of salivary gland tumours and the histopathological characteristics in a quaternary care hospital in South India. Thus far, this is one of the largest studies of primary salivary gland tumours from India. Epidemiological data on these tumours in various parts of the world can be helpful for a better understanding of their biology and clinical characteristics. It can aid in acquiring in-depth knowledge about the nature of salivary gland neoplasms in this part of the country, aiding in better patient care and proper diagnosis.
Footnotes
Acknowledgements
The authors acknowledge the support and cooperation of the hospital staff and medical records department in facilitating access to patient data.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Institutional Ethical Committee Approval Number: AMH-C-S-069/08-24.
Informed consent
A waiver of informed consent was obtained from the Institutional Ethical Committee due to the retrospective nature of the study.
Credit author statement
Dr. Dona Maria George: Conceptualisation, study design, data collection, data analysis and manuscript writing.
Dr. Therese David: Data collection, data analysis and manuscript writing.
Dr. Maya Menon: Conceptualisation, study design, supervision, data analysis, manuscript review and corrections.
Data availability
Data supporting the findings of this study are available from the hospital information system. Access is restricted and may be granted upon reasonable request with appropriate permissions.
Use of artificial intelligence
Artificial Intelligence tools were used solely for grammar correction during manuscript preparation.