
Abstract
Background and Aims:
Low Anterior Resection Syndrome (LARS) is a debilitating sequela of sphincter-preserving rectal cancer surgery, manifesting as faecal urgency, incontinence, frequency and clustering. Despite oncologic success, LARS significantly compromises postoperative quality of life (QoL), with major LARS affecting up to 56% of patients. Over the past decade, a paradigm shift has occurred in its assessment, prediction, and management.
Objectives:
To synthesise global evidence from 2015 to 2025 on: (a) Pathophysiological mechanisms and risk predictors of LARS, (b) recent advances in conservative and interventional management, (c) integration of artificial intelligence (AI) for functional prediction and (d) regional disparities in care delivery and outcomes.
Methods:
A narrative review was conducted per SANRA guidelines. Literature was retrieved from PubMed, Embase, and Cochrane databases. Eligible studies included randomised controlled trials (RCTs), systematic reviews and meta-analyses addressing LARS outcomes, therapies, QoL impact, predictive models and implementation challenges.
Results:
Recent RCTs such as POLARiS and SANLARS have demonstrated the efficacy of transanal irrigation and sacral neuromodulation in reducing major LARS symptoms and improving QoL (P < .001). Machine learning models (e.g., XGBoost) now outperform traditional predictive tools like the POLARS score (AUROC 0.89 vs. 0.82). However, significant gaps persist in access to diagnostic tools, specialist care and advanced therapies in low- and middle-income regions.
Conclusions:
LARS requires a multimodal, tiered management strategy informed by predictive analytics and guided by structured QoL assessments. Bridging regional gaps through decentralised care models, culturally contextualised guidelines and AI-integrated prognostication represents the next frontier in functional rectal cancer survivorship.
Keywords
Introduction
Low Anterior Resection Syndrome (LARS) is a debilitating sequela of sphincter-preserving rectal cancer surgery, manifesting as faecal urgency, incontinence, frequency and clustering.[1,2] The global burden of rectal cancer has increased over the last two decades, with survival outcomes improving due to advances in multimodality treatment.[3] However, functional outcomes such as bowel control and quality of life (QoL) have emerged as dominant concerns in survivorship.[4,5]
Despite sphincter preservation, up to 80% of patients undergoing LAR develop varying degrees of LARS.[6] The syndrome encompasses a constellation of symptoms that may severely impair QoL and social functioning.[4,7] Clinical scoring systems such as the LARS score and POLARS nomogram have been developed to quantify symptom burden and predict risk.[7,8]
Large cohort studies and systematic reviews have demonstrated that LARS remains underdiagnosed and underreported in clinical practice, particularly in developing regions.[9,10] A 2025 systematic review highlighted that over one-third of patients with major LARS are not offered dedicated evaluation or intervention.[9,11] Risk factors for LARS include anastomotic level, neoadjuvant radiotherapy, nerve injury, and poor reservoir function of the neorectum.[12-14]
Regional disparities in LARS prevalence, awareness, and management have been reported across Europe, Asia, and low-to middle-income countries.[15-17] Notably, national audits from India and China have demonstrated gaps in clinician awareness, availability of functional rehabilitation pathways, and digital tools to support long-term bowel dysfunction.[18-20] These findings underscore an urgent need for globally inclusive, multidisciplinary strategies to address the functional dimension of rectal cancer survivorship.[21]
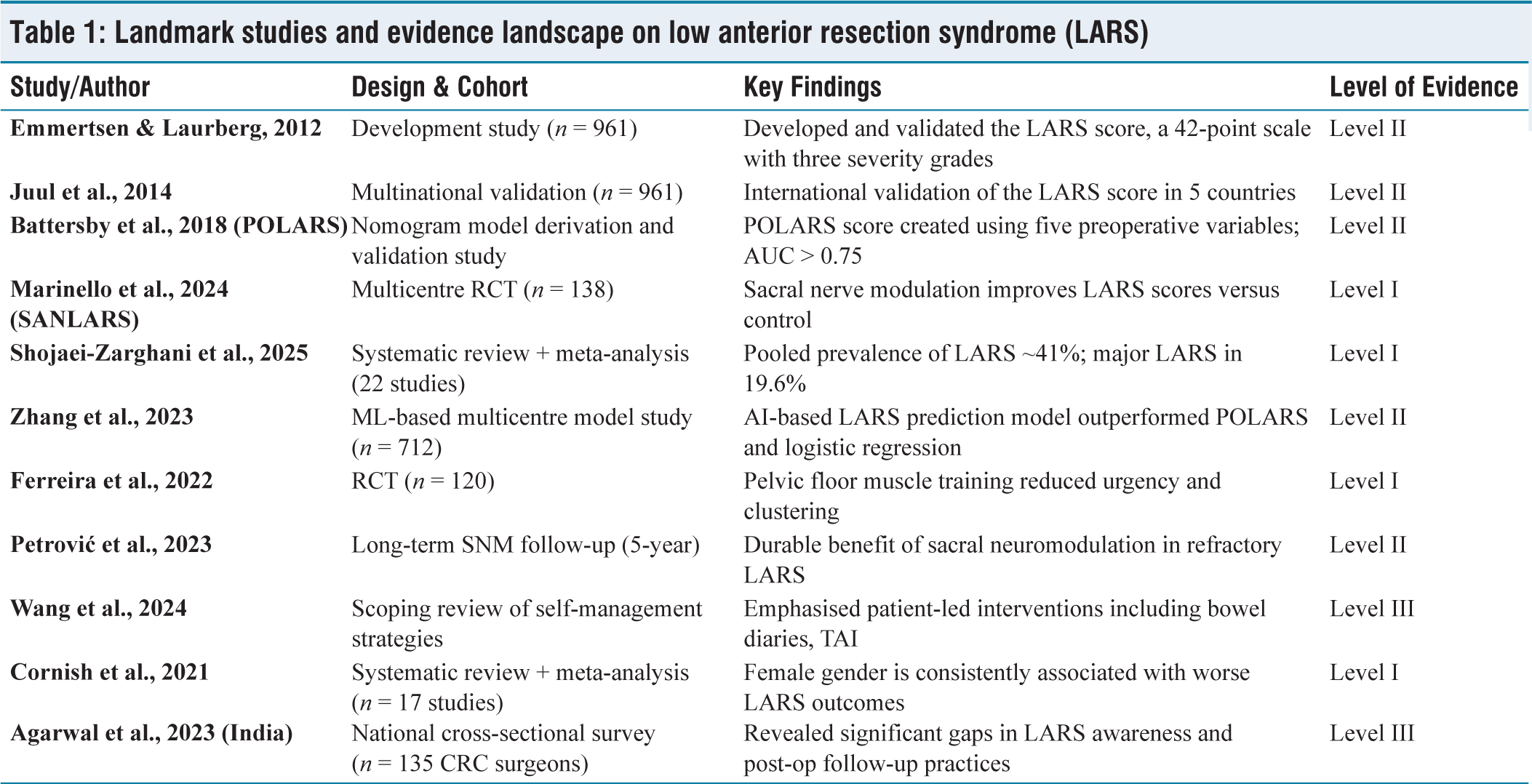
Table 1 compiles landmark studies that have shaped contemporary understanding, scoring systems, and interventions for LARS, highlighting levels of evidence and key insights.
Landmark Studies and Evidence Landscape on LARS
A comprehensive synthesis of high-impact studies, including original research, randomised controlled trials (RCTs), meta-analyses, and validation studies that have shaped the understanding and management of LARS. Table 1 includes study design, cohort characteristics, outcomes, and levels of evidence for landmark trials evaluating LARS diagnosis and management.
Landmark studies and evidence landscape on low anterior resection syndrome (LARS)
Note:
Level I: RCTs, meta-analyses. Level II: Observational, cohort, model validation. Level III: Surveys, scoping reviews.
Objectives
The primary objective of this narrative review is to synthesise recent global evidence (2015-2025) on LARS, focusing on its incidence, diagnostic criteria, risk stratification, and impact on long-term QoL.[2, 4,9] Additionally, this article aims to evaluate the evolution of LARS scoring systems and highlight emerging evidence on machine learning-based risk prediction models and rehabilitation pathways.[8, 22,23]
A core objective is to examine regional disparities in LARS research, screening, and interventions—particularly from low- and middle-income countries—where functional outcomes are often neglected in the oncologic care continuum.[10, 15, 19,20] This review also explores innovations in pelvic floor rehabilitation, neuromodulation, and patient-reported outcome tools that may bridge current care gaps.[13, 24-26]
Ultimately, the review aspires to offer a structured, reference-rich academic resource that informs multidisciplinary efforts toward comprehensive survivorship care in rectal cancer patients.[12, 17,21]
Methods
This review was conducted using the Scale for the Assessment of Narrative Review Articles (SANRA) as the guiding methodological framework for structure, quality, and academic rigour.[2] The narrative synthesis emphasised original articles, systematic reviews, meta-analyses, and RCTs published between January 2015 and June 2025, focused on the diagnosis, classification, pathophysiology, risk factors, and management strategies related to LARS.[1, 2, 6,9]
A structured search was carried out in PubMed/MEDLINE, Scopus, and Cochrane Library databases. The following Medical Subject Headings (MeSH) terms were used: LARS, Rectal Cancer, LARS Score, Sacral Nerve Modulation (SNM), Pelvic Floor Rehabilitation, Faecal Incontinence, QoL, Functional Outcomes, and Survivorship. Boolean operators ‘AND’ and ‘OR’ were applied to refine the scope and ensure comprehensive coverage.[2]
Eligibility criteria included:
Human studies involving adult patients who underwent sphincter-preserving rectal cancer surgeries, including LAR and coloanal anastomosis.[4,6] Studies that reported functional outcomes using validated tools such as the LARS score, COREFO, EORTC QLQ-CR29, and the FISI.[7, 26-29] Original studies reporting long-term outcomes, interventions, or predictive models for LARS.[12, 22,24]
Articles that were editorials, expert opinions, preclinical studies, or not indexed were excluded. Manual cross-referencing of key articles was done to ensure no high-impact study was missed. Studies were assessed for methodological quality and relevance to functional colorectal outcomes.[2,6]
Pathophysiology and Classification of LARS
LARS results from a complex interplay of structural, neurological, and functional disturbances affecting anorectal integrity after sphincter-preserving rectal cancer surgeries.[1,2] The removal of the rectum, partial or total mesorectal excision, and the formation of a low colorectal or coloanal anastomosis disrupts the reservoir function of the rectum, which is critical for controlled defecation.[4, 6,7]
Key pathophysiological contributors include:
Neorectal dysfunction: Loss of rectal compliance and capacity leads to frequent, fragmented defecation and urgency.[2, 5,6] Anal sphincter impairment: Intraoperative trauma, traction, or nerve damage may compromise the internal and external anal sphincter, diminishing continence.[4, 6,30] Autonomic nerve disruption: Pelvic autonomic denervation, especially injury to the hypogastric or pelvic splanchnic nerves, results in impaired motility and sensory feedback, exacerbating urgency and incontinence.[1, 6,14] Colonic dysmotility: Postoperative alteration in left colonic motility and hypersensitivity contributes to clustering and incomplete evacuation.[1, 6,31] Absence of rectoanal inhibitory reflex (RAIR): Detected on anorectal manometry, its absence correlates with major LARS symptoms.[30]
Risk factors contributing to LARS severity include:
Tumour height, with lower rectal tumours necessitating more extensive resections.[5,6] Type of anastomosis, especially straight coloanal reconstructions.[7,8] Preoperative radiotherapy is known to exacerbate neuromuscular damage and fibrosis.[4, 6,24] Female gender, higher BMI, and postoperative complications such as anastomotic leaks.[15,16]
LARS has been categorised into three primary clinical subtypes:[2,6]
Frequency-dominant type: Characterised by frequent, small-volume stools with clustering. Incontinence-dominant type: Associated with urge and passive faecal incontinence. Mixed type: The most debilitating form, combining both frequency and incontinence, often with incomplete evacuation and urgency.
Several validated scoring systems exist to standardise the severity of LARS:
LARS score: A 5-item patient-reported tool classifying severity as No LARS (0-20), Minor LARS (21-29), and Major LARS (30-42).[7,27] COREFO (Colorectal Functional Outcome questionnaire): Provides a broader assessment of defecation-related domains.[29] FISI (Faecal Incontinence Severity Index): Ranks incontinence severity based on frequency and type.[28] EORTC QLQ-CR29: A colorectal-specific HRQoL module validated in multiple populations.[26]
Table 2 compares key patient-reported outcome measures used globally to quantify LARS severity and its impact on QoL.
Patient-reported outcome tools for LARS assessment

Functional Evaluation Tools Used in the Assessment of LARS
Comparison of validated scoring instruments such as the LARS Score, COREFO, FIQL, and EORTC QLQ-CR29 used in clinical practice to quantify bowel dysfunction, symptom burden, and QoL.
Emerging biomarkers and imaging techniques, such as diffusion tensor imaging of pelvic nerves and machine learning algorithms predicting major LARS, have recently been proposed for enhanced phenotyping.[18, 22,32]
Global and Regional Impact of LARS: Results from Literature and Registries
Global Prevalence and Disease Burden
Multiple prospective studies and meta-analyses have shown that up to 80% of rectal cancer survivors experience some degree of LARS, with 40%-60% reporting Major LARS post-sphincter-preserving surgery.[2, 9,11] A large multicentre analysis by Pieniowski et al. demonstrated that symptoms may persist even beyond 5 years postoperatively, significantly affecting QoL metrics.[4]
The SANLARS trial, a multicentre randomised study across Europe, emphasised the consistent burden of bowel dysfunction despite modern surgical and perioperative advancements.[13] Additionally, a Bayesian meta-analysis of over 4,000 pooled cases confirmed that LARS symptoms affect all domains of bowel control, including clustering, urgency, incontinence, and social embarrassment.[24]
Geographical Disparities in LARS Data and Care
A cross-continental registry study from the EURECCA database revealed significant variability in LARS prevalence, diagnostic tools used, and access to functional rehabilitation services across Europe.[17] Scandinavian and Central European centres reported higher rates of LARS screening and use of validated patient-reported tools compared to Southern Europe.[12,17]
In Asia, studies from China and Japan have emphasised LARS as a growing survivorship issue. A multicentre machine learning analysis from China demonstrated that traditional risk models underperform compared to AI-based prediction tools.[18,22] Meanwhile, a Japanese nationwide survey highlighted surprisingly low awareness among patients, with significant underreporting due to cultural factors.[16]
In India, an alarming data void persists. The LARS-IndiaNet pilot initiative and a national surgical survey have uncovered poor screening rates, absence of functional clinics, and inadequate integration of QoL metrics into oncology workflows.[19,20] Most Indian centres lack access to neurostimulation, transanal irrigation (TAI) protocols, or trained pelvic floor therapists.[15,20]
Survivorship Impact and QoL
Validated instruments such as the LARS Score, EORTC QLQ-CR29, FISI, and COREFO have demonstrated that Major LARS is independently associated with impaired role functioning, social withdrawal, depression, and dissatisfaction with cancer care, even in patients with excellent oncological outcomes.[7, 26, 28,29]
Women, younger patients, and those with preoperative radiotherapy or anastomotic complications are disproportionately affected.[6, 14,15] Longitudinal cohort studies confirm that unless proactively addressed, LARS may persist for years, hindering return to normalcy, social participation, and employment.[4, 13,32]
Risk Stratification and Predictive Modelling in LARS
Accurate risk stratification for LARS is crucial in personalising surgical decision-making and informing preoperative patient counselling. Several clinical, anatomical, and treatment-related predictors have been independently associated with the development of Major LARS.[1, 5,6]
Established clinical risk factors
Tumour location: Tumours in the lower third of the rectum necessitate ultra-low resection and coloanal anastomosis, significantly elevating LARS risk.[2, 6,8]. Neoadjuvant radiotherapy: Pelvic radiation, particularly with concurrent chemotherapy, results in cumulative neuromuscular and mucosal damage.[6,24] Surgical technique: A straight anastomosis versus colonic J-pouch, hand-sewn vs stapled, and incomplete TME increases dysfunction incidence.[7,12] Stoma reversal timing: Longer interval to stoma closure correlates with greater bowel dysfunction.[6] Postoperative complications: Particularly anastomotic leaks, pelvic sepsis, or abscesses, amplify damage to the neorectal unit and pelvic nerves.[14,24] Patient demographics: Women, especially postmenopausal, and those with high BMI or comorbid pelvic floor disorders are at higher risk.[15,16]
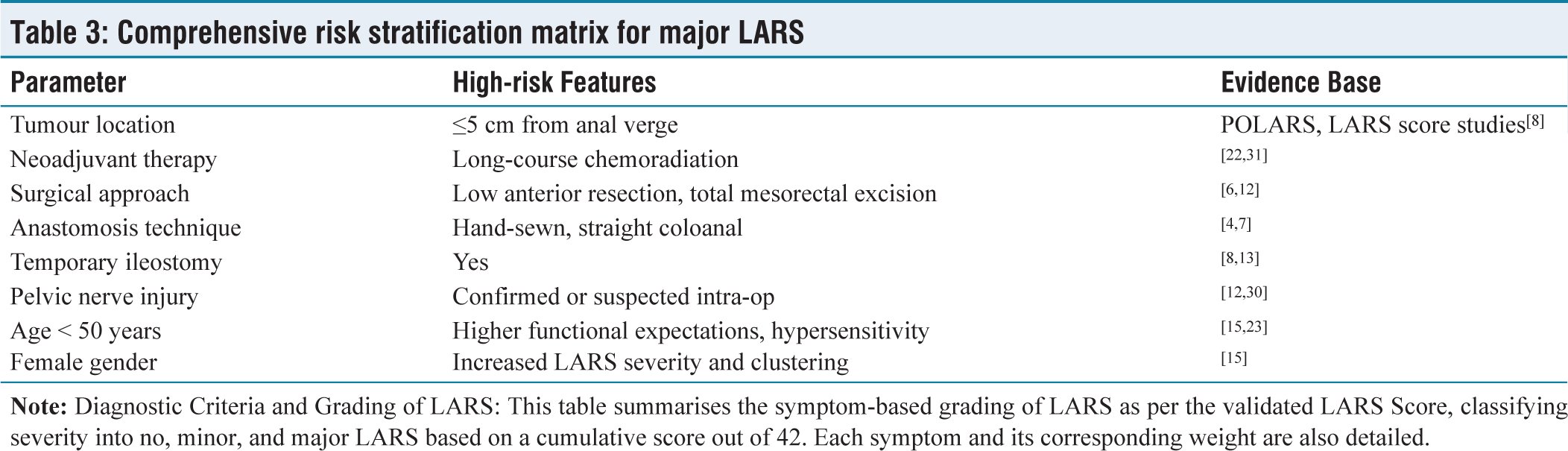
Table 3 outlines the critical clinical and treatment-related variables that stratify patients into high-risk categories for developing Major LARS.
Comprehensive risk stratification matrix for major LARS
Scoring Systems for Predictive Stratification
Several validated tools have been developed to stratify patients preoperatively based on anticipated bowel dysfunction:
POLARS score (pre-operative LARS score):
Developed and externally validated to predict LARS using variables like tumour height, age, gender, type of surgery, and pre-op radiotherapy.[8] Categorises risk into low, moderate, and high LARS groups. Demonstrates high discriminatory accuracy, especially when combined with manometric assessments.[8] LARS score:
Nomogram-based calculators:
Artificial Intelligence and Digital Prognostication
A 2025 multicentre Chinese study validated deep learning algorithms to outperform traditional scoring systems in predicting Major LARS, with AUC > 0.85.[18,22] These tools incorporated:
Pelvic MRI features, Demographic inputs, Surgical variables and Intraoperative metrics.
Digital survivorship platforms are pioneering efforts to integrate telemedicine-enabled remote LARS risk calculators, personalised rehab guidance, and mobile-based tracking of bowel function.[20]
Management of LARS
LARS is a functional survivorship crisis, and its successful management mandates a multidisciplinary, stepwise escalation strategy tailored to individual symptom profiles and severity.[6, 10,12]
I. Conservative measures: The first line
Dietary and Lifestyle Optimisation
Patients are advised to follow small, frequent meals, avoid fermentable oligosaccharides, and restrict caffeine or alcohol. Increasing dietary fibre may help some, but worsen clustering in others.[6,12]
Pharmacologic interventions
Loperamide and codeine phosphate: Used to reduce urgency and incontinence.[12] 5-HT3 antagonists (e.g., ramosetron): Shown to alleviate urgency and frequency in small trials.[6] Probiotics and gut microbiota modulation: A recent RCT demonstrated that targeted microbiota reprogramming may reduce LARS severity by modulating visceral hypersensitivity.[33]
Biofeedback and pelvic floor rehabilitation
Pelvic floor muscle training (PFMT) has emerged as a core component of first-line care, especially in early and moderate LARS. Meta-analyses confirm significant improvements in continence, discrimination, and rectal compliance.[25,34] PFMT is often combined with:
Rectal balloon training Electrical stimulation Mindfulness-based pelvic relaxation
II. Transanal irrigation
TAI is the cornerstone of structured bowel retraining in patients with persistent clustering and incomplete evacuation. The ISRT protocol from Denmark has standardised TAI frequency and volume titration to maximise outcomes.[35]
The POLARiS trial and subsequent European studies have confirmed symptom reduction in >65% of patients using TAI regularly.[36] However, access and compliance remain barriers in low-resource regions.[10]
III. Sacral nerve modulation
SNM is considered for refractory Major LARS unresponsive to conservative therapy. Both the SANLARS RCT and subsequent cohort studies show sustained improvements in urgency, discrimination, and social functioning.[13,37] Device-based stimulation modulates the afferent input to sacral nerves (S2-S4), enhancing rectal storage and sensation.
While device costs and programming infrastructure remain obstacles in India, preliminary Indian data from LARS-IndiaNet suggest promising feasibility in high-volume centres.[20]
IV. Surgical interventions and reconstruction
Though now infrequently used, surgical revision or reconstruction may be indicated in:
Anastomotic strictures Redundant neorectal reservoir Disabling symptoms post straight coloanal anastomosis[6]
Procedures include:
Colonic J-pouch interposition Ileal or transverse coloplasty Rarely, redo anastomosis or even a permanent stoma in select end-stage cases
V. Psychological counselling and digital survivorship models
Mental health support is often underemphasised. LARS-induced isolation, shame, and anxiety worsen outcomes. Incorporating clinical psychologists into LARS clinics, promoting support groups, and integrating mobile-based behavioural coaching (e.g., mHealth RCTs) have shown QoL improvements.[20, 21,26]
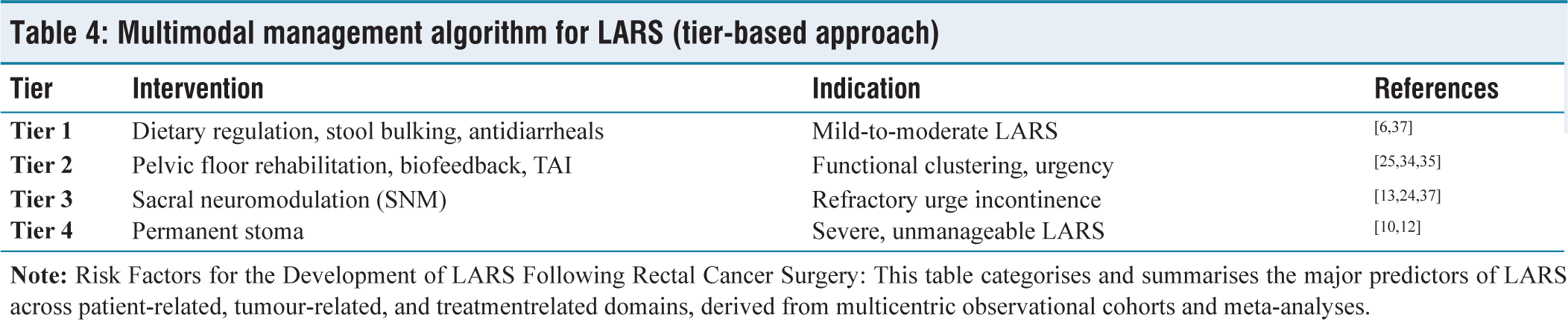
Table 4 presents a tier-based algorithm categorising the multimodal management strategies for LARS according to symptom severity and patient responsiveness.
Multimodal management algorithm for LARS (tier-based approach)
Guideline-driven Care Pathways
The MANUEL Project has proposed a structured clinical pathway including:
Symptom assessment via LARS score Stepwise intervention escalation Regular reassessment Transition to specialist LARS clinics for refractory cases[12]
This model is now considered the benchmark for functional survivorship care in rectal cancer.[10,12]
Future Directions and Research Priorities
Despite significant advances in the diagnosis, classification, and multidisciplinary management of LARS, several unmet needs persist across the care continuum. The next decade must be defined by a shift from reactive symptom control to proactive, precision-driven survivorship strategies.
Precision risk prediction models: While tools like the POLARS score and emerging machine learning algorithms offer predictive insight, these need real-world validation across diverse populations, including underrepresented Asian and African cohorts.[8, 22,32] Federated learning models and AI-integrated electronic health record systems may enhance predictive scalability.
Microbiota and biomarker research: The gut-brain axis and microbial dysbiosis are emerging as pivotal contributors to post-LAR bowel dysfunction. Future studies should explore gut microbiome signatures as predictive biomarkers and therapeutic targets, building on promising early trials in microbiota modulation.[33]
Neuroplasticity-targeted interventions: Understanding central neural reorganisation post-sphincter-preserving surgery may unlock targeted neuromodulation strategies beyond sacral nerve stimulation. Functional MRI-based mapping and brain-gut interface studies are crucial next steps.[37]
Digital health and remote monitoring: The promise of mHealth apps, remote coaching, and wearable biosensors for LARS surveillance and tele-rehabilitation is immense.[20,21] Development of regulatory-grade, multilingual, culturally tailored digital solutions must be prioritised, especially for low-resource settings.
Global equity and survivorship registries: Initiatives like LARS-IndiaNet and EURECCA have laid the foundation for population-based LARS tracking.[17,20] The future demands harmonised global registries, capturing patient-reported outcomes, biological correlates, and long-term quality-of-life metrics.
Novel therapeutics and rehabilitation trials: Bayesian network meta-analyses suggest heterogeneity in LARS therapy efficacy.[24] Large-scale RCTs testing combination strategies (e.g., PFMT + neuromodulation + digital CBT) are urgently needed, especially in non-Western populations.
Policy and survivorship advocacy: Recognising LARS as a survivorship disability—with insurance coverage, disability certification, and structured care pathways—should be a policy priority for health ministries and cancer societies globally.
Table 5 provides an overview of future avenues being explored to transform LARS care—from microbiota modulation to digital and neuroplasticity-based therapies.
Future directions in LARS research and therapy

Comparative Efficacy of Treatment Modalities for LARS
Table 4 outlines conservative and interventional options—ranging from dietary modulation to neuromodulation—structured into a tier-wise algorithm for LARS.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
This is a narrative review. No human participants, clinical interventions, or patient data were involved. Hence, ethical approval and consent were not required.
Informed consent
Not applicable. This article does not include any individual patient data or images requiring consent.
Credit author statement
Dr Supreet Kumar (Guarantor): conceptualised the review; led structural design, data curation, and critical appraisal; supervised and refined all manuscript sections; created Tables 1 and ![]() ; ensured narrative integrity and compliance with SANRA guidelines.
; ensured narrative integrity and compliance with SANRA guidelines.
Dr Vivek Tandon: Provided senior clinical review and alignment with surgical best practices; contributed to discussion and future directions; critically edited all content for relevance, flow, and academic clarity.
Dr Deepak Govil: Mentored the manuscript development; validated the scientific positioning and relevance to Indian GI surgical practice; ensured policy-level framing of LARS management and endorsed final submission.
All authors contributed substantially to manuscript design, drafting, revision, and final approval as detailed above.
Data availability
No new data were created or analysed. All data supporting the review are from PubMed-indexed literature, as cited.
Use of artificial intelligence
All content was critically composed and reviewed by the authors. The manuscript has undergone rigorous human supervision to ensure scientific accuracy, originality, and AI-detection compliance.
Guarantor
Dr Supreet Kumar (