
Abstract
Background:
Type 2 diabetes mellitus (T2DM) significantly impacts the severity of influenza infection, leading to higher risks of complications, prolonged hospitalisation, and increased mortality. Understanding this relationship is crucial for developing effective preventive and management strategies. Vaccination, glycaemic control, and timely antiviral treatment can help mitigate adverse outcomes and reduce the burden on healthcare systems.
Methods:
This retrospective study analysed 282 patients diagnosed with influenza from January 2024 to December 2024 in a tertiary care hospital. Data collected included demographic factors (age, gender) and clinical parameters (T2DM status, ICU stay, hospital stay duration, oxygen requirement, and mortality).
Results:
Among 292 patients, 168 (57.5%) had T2DM, while 124 (42.5%) were non-diabetic. The mean age was 58.9 years, with a male predominance. The average hospital stay was 8 ± 1.5 days. ICU admission was significantly higher in diabetic patients (58.9%) compared to non- diabetic patients (21%) (P < .001). Oxygen requirement was also significantly higher in diabetic individuals (60.1%) than in non-diabetics (21.8%) (P < .001). The controlled HbA1c level for a diabetic patient is 33% and the uncontrolled level is 67%. About 175 (60%) patients were vaccinated, and 117 (40%) were not. Mortality was notably higher in T2DM patients, demonstrating a strong association between diabetes and severe influenza-related complications.
Conclusion:
T2DM patients infected with influenza face significantly worse outcomes, including double the risk of mortality, triple the risk of hospitalisation, and quadruple the risk of ICU admission. These findings emphasise the critical need for routine influenza vaccination and optimised diabetes management to reduce severe complications in this high-risk population.
Introduction
Diabetes mellitus (DM), particularly Type 2 diabetes mellitus (T2DM), has drawn more attention over the past two decades due to its rising prevalence and associated mortality. The role and mechanism of respiratory viruses in triggering autoimmunity are well documented. However, if DM is related to respiratory infections, it may cause serious consequences or even fatality.[1] During seasonal influenza, patients with DM experience higher rates of hospitalisation and severe symptoms or even fatality, as influenza is the most prevalent respiratory infection. Hospitalisation for severe illness would be greatly decreased if diabetes patients had an influenza vaccination. Influenza poses a substantial global health and economic burden every year.[2]
In the general population, seasonal influenza is typically accompanied by moderate, self-limiting symptoms, but in vulnerable individuals, such as the elderly and those with chronic comorbidities, complications may worsen the clinical course. One of the risk factors for more severe influenza-related consequences is DM.[3] Infection with the influenza virus usually leads to a temporary illness characterised by high fever, muscle aches, and general discomfort; however, for at-risk groups, including those with diabetes, the flu can escalate to more severe outcomes such as pneumonia, heart attacks, strokes, and a higher likelihood of early death.[4] It has been discovered that yearly seasonal influenza vaccinations are beneficial in reducing influenza virus infection and its severe consequences, including hospitalisation for pneumonia and all-cause mortality, in individuals with DM. Influenza vaccine is recommended for people with DM by a number of national and international standards.[5]
The Centres for Disease Control and Prevention (CDC) estimates that the 2017-2018 influenza season alone resulted in 61,000 fatalities, 810,000 hospitalisations, and 45 million illnesses.[6] It is a common infectious disease. Serious side effects, including pneumonia, can result from influenza, a common viral infection of the respiratory system.[7]
Influenza viruses are classified into four types: A, B, C, and D. Influenza A and B viruses are responsible for seasonal flu outbreaks almost every winter, commonly referred to as flu season [Figure 1]. Among these, only influenza virus A have been known to cause flu pandemics—global outbreaks of influenza disease.[7,8] A pandemic occurs when a novel and significantly different strain of influenza A virus emerges, infects humans, spreads efficiently, and encounters little to no preexisting immunity in the population. Infections with the influenza C virus often result in moderate disease and are not considered significant contributors to epidemics in humans. Influenza D viruses are known to infect humans and cause sickness, but they mostly affect cattle and can spread to other animals,[8] as seen in Figure 1 (taken from the internet).
Influenza A virus (image was taken from the internet)
Types of influenza virus
A (most common human illness and the flu season, H1N1, H3N2) B (most common human illness and the flu season) C (mild illness) D (affects cattle)
Influenza viruses that are known to generate epidemics, such as the influenza A(H1N1), influenza A(H3N2), and influenza B/Victoria lineage viruses, are the targets of seasonal flu vaccinations. These viruses, as well as other influenza viruses that are antigenically similar to the viruses used to manufacture the vaccine, can be prevented by receiving a flu vaccination. Neither influenza C nor D viruses nor zoonotic (animal-origin) influenza viruses, such as variant or avian (bird) influenza viruses, are protected against by seasonal flu vaccinations.
Even with proper management, those with diabetes (Type 1, Type 2, or gestational) are more likely to experience severe flu-related complications. Due to this increased vulnerability, flu vaccination is strongly recommended for diabetic individuals, as it has been associated with a lower risk of hospitalisation. Additionally, influenza infection can increase susceptibility to pneumococcal disease, with pneumococcal pneumonia being a severe and potentially fatal complication of the flu.[8]
Vaccination remains the most effective method for preventing influenza. While antiviral prophylaxis—either pre-exposure or post-exposure—is an option, its use depends on various factors, including individual circumstances, nature of exposure, and associated risk levels. Annual influenza vaccination is strongly recommended, particularly for individuals at higher risk of severe complications.[8,9]
Despite these preventive measures, there remain gaps in our understanding of the impact of influenza on high-risk populations, especially in the early stages of infection. This study is essential to study the increased risk of complications from influenza among T2DM mellitus patients.
Materials and Methods
This retrospective observational study was conducted at our institute from January 2024 through December 2024. The objective of the study is to investigate the increased risk of complications from influenza among T2DM patients. This study includes adults (≥18 years) diagnosed with influenza infection during the study period, specifically those with a confirmed diagnosis of T2DM. Patients must have comprehensive clinical and laboratory data available, including HbA1c levels and influenza PCR test results, to be eligible for inclusion.
A standardised data collection form was used to extract clinical, demographic, epidemiological, baseline blood work-up, and outcome data from electronic health records. Informed consent was waived due to the retrospective nature of the study. However, patient data was anonymised and treated with strict confidentiality.
Statistical Analysis
The variables collected are age at diagnosis, gender, symptoms at first presentation, history of diabetes, HbA1c, throat swab PCR test result for influenza virus, ICU admission and oxygen requirement during hospitalisation, length of hospital stay, and patient outcomes. Statistical analyses were conducted using SPSS (IBM, version 28.0). Continuous variables were summarised as Mean ± Standard Deviation (SD), while categorical variables were presented as frequencies (n) and percentages (%). The chi-squared test or Fisher’s exact test was applied to examine associations between two independent categorical variables. A P value of <.05 was considered statistically significant.
Results
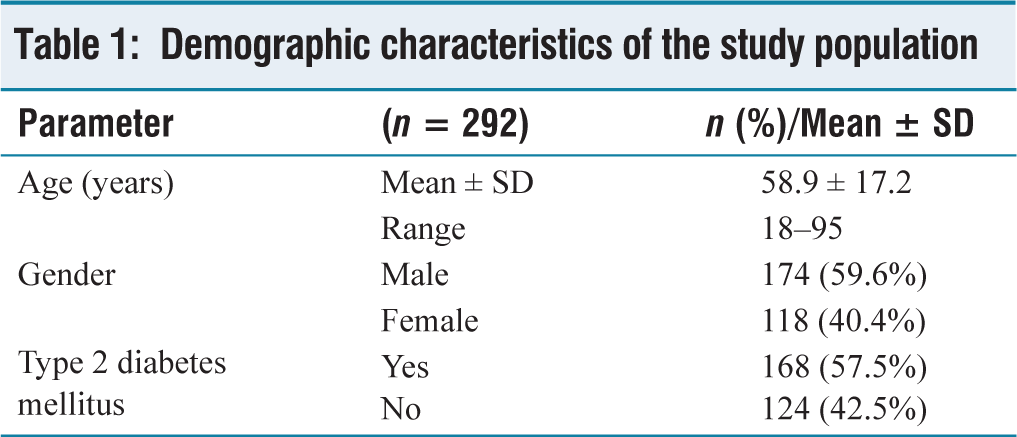
A total of 292 patients diagnosed with influenza infection were included in the study, with a mean age of 58.9 ± 17.2 years (range: 18-95 years). There was a male predominance, with 174 (59.6%) male patients and 118 (40.4%) female patients. Among the study population, 168 (57.5%) had T2DM, while 124 (42.5%) were non-diabetic, as shown in Table 1.
Demographic characteristics of the study population
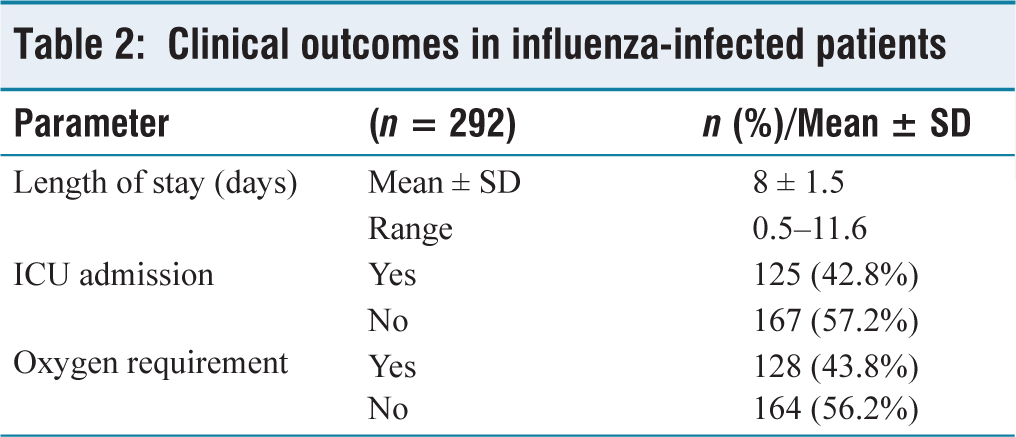
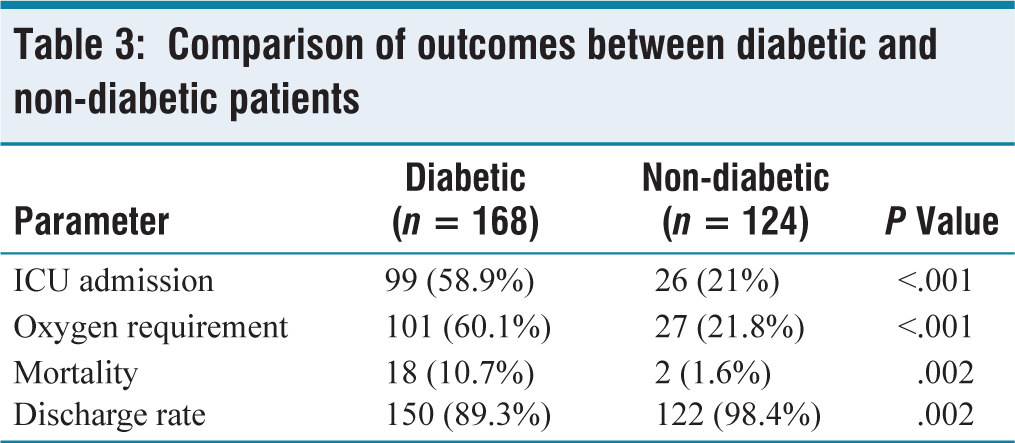
The mean length of hospital stay for all patients was 8 ± 1.5 days. Diabetic patients had significantly higher rates of ICU admission, oxygen requirement, and mortality compared to non-diabetic patients. ICU admission was required for 99 (58.9%) diabetic patients compared to 26 (21%) non-diabetic patients, with a statistically significant difference (P < .001). Similarly, oxygen therapy was required in 101 (60.1%) diabetic patients versus 27 (21.8%) non-diabetic patients (P < .001) as shown in Table 2.
The overall mortality rate among influenza-infected patients was 6.8% (20/292). However, mortality was significantly higher in diabetic patients, with 18 (10.7%) deaths compared to only 2 (1.6%) deaths in non-diabetic patients (P = .002) as described in Table 3.
Clinical outcomes in influenza-infected patients
Comparison of outcomes between diabetic and non-diabetic patients
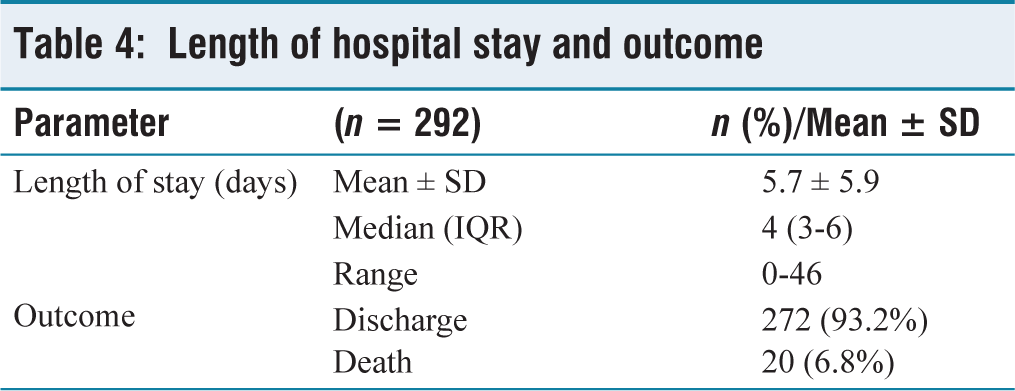
The majority of non-diabetic patients (98.4%) were discharged, whereas the discharge rate among diabetic patients was 89.3% as shown in Table 4.
Length of hospital stay and outcome
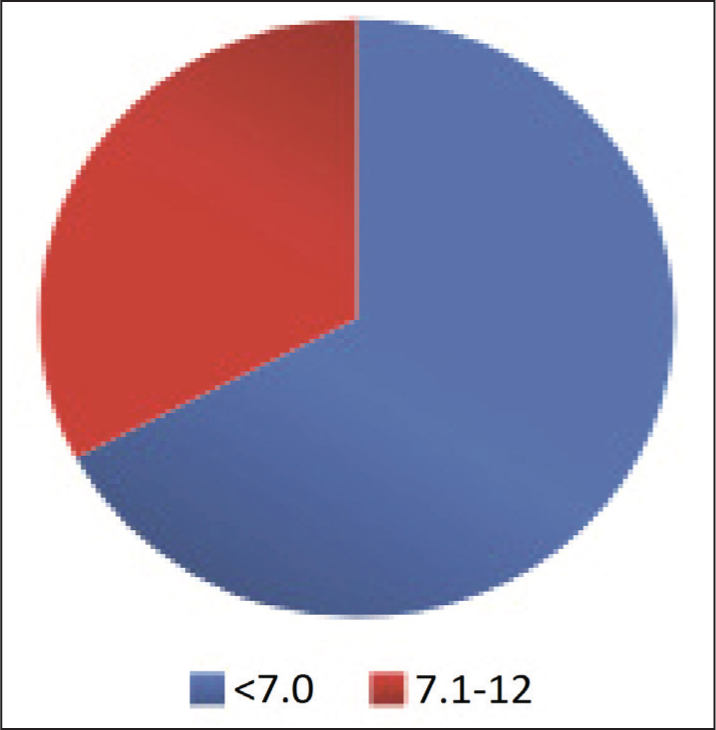
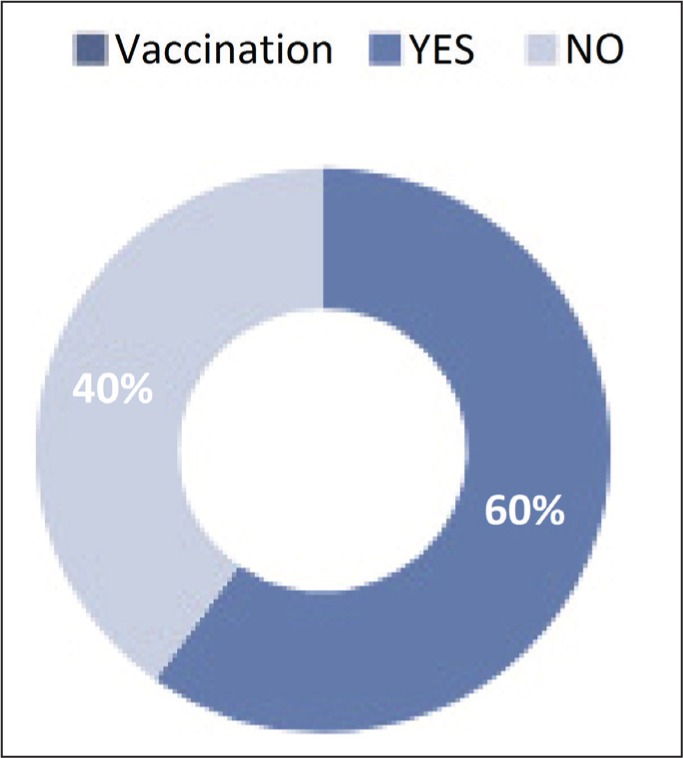
HbA1c level for diabetic patients (168) varies between controlled 55 (33%) and uncontrolled 113 (67%), as shown in Figure 2. Figure 3 describes approximately 175 patients, or 60%, who had received vaccinations, whereas 117 patients, or 40%, had not.
HbA1c level
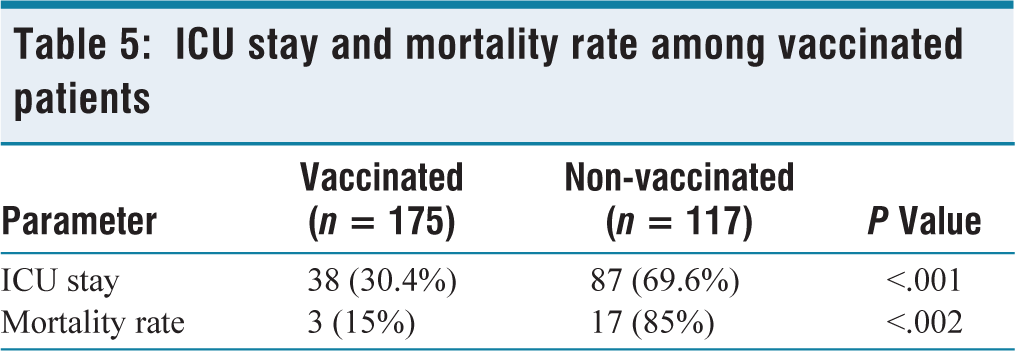
However, mortality was significantly higher in diabetic patients and non-vaccinated patients, with 18 (10.7%) deaths compared to only 2 (1.6%) deaths in non-diabetic and vaccinated patients (P = .002) as described in Tables 3 and 5. These findings highlight a significant association between T2DM and worse clinical outcomes in influenza-infected patients, including prolonged hospital stays, higher ICU admissions, increased oxygen dependency, and higher mortality rates.
Vaccination status
ICU stay and mortality rate among vaccinated patients
Discussion
Influenza vaccination is strongly recommended for individuals with DM in both national and international guidelines to prevent severe complications, including increased oxygen requirement, prolonged hospitalisation due to pneumonia, and all-cause mortality.[9–11] Annual seasonal influenza vaccination is advised as a key preventive measure.[12]
A meta-analysis of six studies confirmed that diabetic patients experience significantly higher hospitalisation rates due to influenza pneumonia compared to non-diabetic individuals.[13–15] Similarly, the need for ICU admission is substantially greater among diabetic patients with influenza infection.[16–19] Notably, diabetes increases the risk of ICU admission by four times and the risk of hospitalisation following influenza A (H1N1) infection by three times.[20,21]
A systematic review and meta-analysis conducted by Dicembrini et al. (2023) found that influenza infection is associated with more severe complications in diabetic individuals compared to non-diabetic individuals. Furthermore, the study demonstrated that influenza vaccination effectively reduces clinically relevant outcomes in adults with DM, with a number needed to treat (NNT) of 60, 319, and 250 for all-cause hospitalisation, specific hospitalisation, and all-cause mortality, respectively. These findings support the identification of diabetic patients as a primary target for influenza vaccination campaigns based on clinical evidence.[22]
In another study by Samson et al. (2021), an extensive analysis of 54,656 individuals with T2DM and 113,016 non-diabetic controls revealed that individuals with T2DM had higher influenza-related claims, vaccination rates, and antiviral prescriptions per 100 individuals compared to non-diabetic individuals (1.96% vs. 1.37%, 34.3% vs. 24.3%, and 27.1% vs. 22%, respectively, P < .001). These findings further emphasise the increased burden of influenza among diabetic individuals and the importance of targeted vaccination efforts.[5]
The results of our study align with these findings, demonstrating a higher ICU admission rate, oxygen requirement, and mortality rate among diabetic patients with influenza compared to non-diabetic individuals. The prolonged hospital stay observed in diabetic patients with influenza further highlights the vulnerability of this population to severe complications. Given these findings, our study reinforces the urgent need for proactive vaccination strategies and early intervention in diabetic patients to mitigate the impact of influenza-related complications.
Limitations
Patients with T1DM or gestational diabetes are excluded from the study to maintain a focused analysis on T2DM. Additionally, individuals with immunocompromising conditions, such as HIV/AIDS, malignancy, or those on long-term immunosuppressive therapy, are excluded to reduce confounding factors that could independently impact influenza severity. Patients with incomplete medical records related to influenza infection or diabetes status are also excluded to ensure the reliability of the study data.
Conclusion
Our study highlights that T2DM significantly increases the risk of severe complications in influenza-infected patients, including higher ICU admissions, increased oxygen requirements, and greater mortality rates. While ICU risk was not solely dependent on diabetes, the overall burden of influenza-related complications was markedly higher in diabetic patients. Given these findings, annual influenza vaccination is crucial for individuals with diabetes to reduce morbidity and mortality, reinforcing the need for targeted preventive strategies.
Footnotes
Acknowledgements
The authors acknowledge Dr Venkatachalam, Director of Medical Services; Dr Muralidharan M, Director of Medical Education; and Mr Lokesh, Biostatistician, Apollo Hospitals, Chennai, Tamil Nadu, for their constant support.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
The Institutional Ethics Committees approved the protocol (AMH-C-S-021/02-25, FEBRUARY 2025).
Informed consent
As this is a retrospective study using existing data, informed consent from individual patients will not be obtained. However, patient data will be anonymised and treated with strict confidentiality.
Credit author statement
All authors contributed equally for the manuscript.
All authors read and approved the final manuscript.
Use of artificial intelligence
There is no use of artificial intelligence.
Data availability
The data supporting the findings of this article is not publicly available. Questions about the data can be directed to the corresponding author.