
Abstract
Background:
A frequent treatment for end-stage osteoarthritis is total knee replacement (TKR), which can cause excruciating postoperative pain. Optimising recovery and rehabilitation results requires effective pain management. The analgesic effectiveness of continuous adductor canal block catheter (CACB) with posterior capsular infiltration and single-shot adductor canal block (SACB) in patients having unilateral robotic TKR was evaluated in this study.
Methods:
This retrospective study included 60 patients who underwent unilateral robotic TKR between December 2023 and December 2024. Patients were divided into two groups of 30 each: Group 1 received a SACB with posterior capsular infiltration, while Group 2 received a CACB with posterior capsular infiltration. The visual analog scale (VAS) was used to measure postoperative pain in the recovery room and at 12 hours, 24 hours, and 48 hours after surgery. This was the main primary measure. The time it took to provide rescue analgesics was the secondary outcome.
Results:
Both groups were comparable in terms of demographic characteristics and American society of anaesthesiologists (ASA) physical status. Group 2 (CACB) demonstrated significantly lower VAS pain scores at all time points compared to Group 1 (SACB) (P < .001). In Group 2, the average duration before the first rescue analgesia was considerably longer (634.5 ± 71.2 minutes) compared to Group 1 (435.8 ± 26.9 minutes, P < .001). The groups’ differences in pain scores become more noticeable after one day, with Group 2 continuing to have superior analgesia.
Conclusion:
When paired with posterior capsular infiltration, continuous adductor canal block (ACB) offers better analgesia than the SACB for patients having robotic TKR. While both techniques provide effective pain relief in the first 24 hours, CACB demonstrates sustained analgesic efficacy beyond this period, resulting in delayed requirement for rescue analgesia and better pain control. This enhanced pain management approach may contribute to improved rehabilitation outcomes and shorter hospital stays.
Keywords
Introduction
Total knee replacement (TKR) remains one of the most successful orthopaedic procedures for treating end-stage osteoarthritis, with more than 700,000 procedures performed annually in the United States alone.[1–3] Despite its effectiveness in relieving chronic pain and restoring function, TKR is associated with significant postoperative pain that can impede early mobilisation, delay rehabilitation, and negatively impact patient satisfaction and outcomes.[4] Therefore, improving healing and maximising functional outcomes require effective pain management.
The evolution of TKR has seen significant advancements with the introduction of robotic assistance, which creates a virtual, patient-specific 3D reconstruction of the knee joint using anatomical data in computerised software.[1] Robotic TKR has demonstrated improved precision in component positioning and alignment compared to conventional techniques, potentially leading to better functional outcomes and implant longevity.[1] However, the management of postoperative pain remains a critical challenge regardless of surgical technique.
Various analgesic modalities have been employed for pain management after TKR, including systemic analgesics, neuraxial techniques, peripheral nerve blocks, and local infiltration analgesia. Among these, adductor canal block (ACB) has gained popularity due to its ability to provide effective sensory analgesia while preserving quadriceps motor function, thereby facilitating early mobilisation and rehabilitation.[9] ACB can be administered as a single-shot adductor canal block (SACB) or through a continuous catheter-based infusion, each with distinct advantages and limitations.
SACB offers technical simplicity, reliability, and effectiveness, but its analgesic duration is limited to 16–24 hours, potentially resulting in rebound pain.[1] Conversely, continuous adductor canal block catheter (CACB) extends the analgesic effect through continued local anaesthetic infusion but requires additional resources, expertise, and carries risks, such as catheter dislodgement or infection.[5] The optimal approach for balancing pain relief with early rehabilitation remains debated, with conflicting evidence in the literature regarding the superiority of CACB over SACB.[4]
Furthermore, posterior capsular infiltration has become a complementary method for treating posterior knee discomfort that ACB alone might not be able to sufficiently address.
The posterior knee capsule is richly innervated by branches of the tibial nerve and is a significant source of pain following TKR.[3] Local anaesthetic infiltration in this area may provide accelerated rehabilitation and reduce opioid consumption post-procedure.[4]
Despite growing interest in these techniques, there is limited evidence specifically comparing SACB versus CACB when combined with posterior capsular infiltration, particularly in the context of robotic TKR. Previous studies have primarily focused on conventional TKR or have compared these techniques separately without considering their combined effect.[5–11]
The rationale for our study stems from the need to determine the most effective analgesic approach for patients undergoing robotic TKR, considering both the immediate postoperative period and the subsequent days when rehabilitation efforts intensify. By comparing SACB versus CACB when combined with posterior capsular infiltration, we aim to provide evidence-based guidance for optimising pain management protocols in this evolving surgical field.
Materials and Methods
This was a retrospective study analysing data from patients who underwent unilateral robotic TKR between December 2023 and December 2024. All patients who underwent unilateral robotic TKR surgery during the study period and who met the inclusion and exclusion criteria were included.
A total of 60 patients who satisfied the inclusion and exclusion criteria were included in the study, with 30 patients in each group:
Group 1: Single-shot adductor canal nerve block with posterior capsular infiltration Group 2: Continuous adductor canal nerve block catheter with posterior capsular infiltration
Aim
Our study compared single-shot and continuous adductor canal nerve block, both in conjunction with posterior capsular infiltration, to ascertain the most efficient method of analgesia for patients having robotic TKR.
Objectives
Primary objective: To compare postoperative pain scores, measured by the visual analog scale (VAS), between two groups of patients who have undergone robotic TKR. Group 1: Patients receiving single-shot adductor canal nerve block with posterior capsular infiltration Group 2: Patients receiving continuous adductor canal nerve block catheter with posterior capsular infiltration
Pain scores were assessed in the recovery room and at 12 hours, 24 hours, and 48 hours postoperatively.
Secondary objective: To document and compare the time to first rescue analgesic administration between the two groups.
Inclusion Criteria
Patients with osteoarthritis of the knee requiring primary TKR during hospitalisation
Patients aged more than 18 years
American society of anaesthesiologists (ASA) physical status of I to III
Exclusion Criteria
Individuals whose body mass index is greater than 40 kg/m²
Individuals who are allergic to any of the medications included in the multimodal perioperative pain regimen, systemic opioids (fentanyl, morphine, hydromorphone), or local anaesthetics
Patients undergoing revision knee replacement
Patients with impaired kidney function or coagulopathy
Patients with chronic pain syndromes or chronic opioid use (defined as regular daily doses of systemic opioids during the six months before surgery)
Study Procedure
All patients received a standardised anaesthetic protocol consisting of spinal anaesthesia with 0.5% bupivacaine heavy (12.5 mg-15 mg) and underwent robotic TKR by the same surgical team using the same surgical technique.
Group 1 (SACB with Posterior Capsular Infiltration)
Patients received SACB with 20 ml of 0.125% bupivacaine with 0.2 ml of 1:100,000 adrenaline and 8 mg dexamethasone. The block was conducted using ultrasound guidance at the mid-thigh level, with identification of the femoral artery, sartorius muscle, and saphenous nerve within the adductor canal.
Group 2 (CACB with Posterior Capsular Infiltration)
Patients received a continuous ACB with the initial bolus of 20 ml of 0.125% bupivacaine with 0.2 ml of 1:100,000 adrenaline and 8 mg dexamethasone, followed by catheter placement under ultrasound guidance. Postoperatively, a continuous infusion of 0.125% bupivacaine was administered at 8 ml/hr for 48 hours.
Posterior Capsular Infiltration (Both Groups)
The posterior capsular infiltration was performed by the operating surgeon in both groups using a standardised solution containing 15 ml of 0.5% bupivacaine, 0.5 ml 1:100,000 adrenaline, and 2 ml of ketamine (1:10 dilution) in a total volume of 50 ml.
Postoperative Management
All patients received a standardised multimodal analgesic regimen consisting of:
Intravenous paracetamol 1g every 8 hours Intravenous ketorolac 30 mg every 12 hours for the first 24 hours, followed by oral celecoxib 200 mg twice daily
Rescue analgesia was administered as intravenous tramadol 50 mg when the VAS score was ≥4 or when requested by the patient.
Data Collection
Data were collected from patient records, including demographic information, such as age, gender, and BMI, as well as ASA physical status. The VAS was used to measure pain at multiple intervals, including in the recovery room immediately after surgery and at 12 hours, 24 hours, and 48 hours after the procedure. After the procedure ended, the time it took to provide the first rescue analgesic was also recorded in minutes. The study’s protocol was approved by the Institutional Ethics Committee . As a retrospective study using existing data, individual patient consent was not required. However, all patient data were anonymised and handled with strict confidentiality in accordance with institutional guidelines.
Statistical Analysis
Statistical analysis involved descriptive statistics, where continuous variables expressed as mean ± standard deviation (SD), and categorical variables as frequency (percentage). The median and interquartile range (IQR) were presented for data that were not normally distributed. The Shapiro-Wilk test was used to assess data normality, and comparisons between groups were performed using the Student’s t-test or Mann-Whitney U test for continuous variables, and the Chi-square or Fisher’s exact test for categorical variables. The Friedman test was used to analyse changes in VAS scores over time within each group, with the Wilcoxon signed-rank test conducted for post-hoc pairwise comparisons. SPSS software (IBM, version 28.0) was used for all analyses, and a P value of less than .05 was deemed statistically significant.
Methodology
All patients who underwent Unilateral Robotic TKR surgery between December 2023 and December 2024, and who met the inclusion and exclusion criteria, were included in this study. They were divided into two groups. One group received only a single-shot adductor canal nerve block. The other group was provided with a continuous adductor canal nerve block catheter with local anaesthetic infiltration in the posterior capsule in both groups. The post-operative pain scores were documented with the VAS score, and the time of the first rescue analgesic given was noted. This was done periodically at the recovery room, 12 hours, 24 hours, and 48 hours postoperatively. In this way, the two groups were compared for analgesic efficacy.
Results
Demographic Characteristics and Baseline Parameters
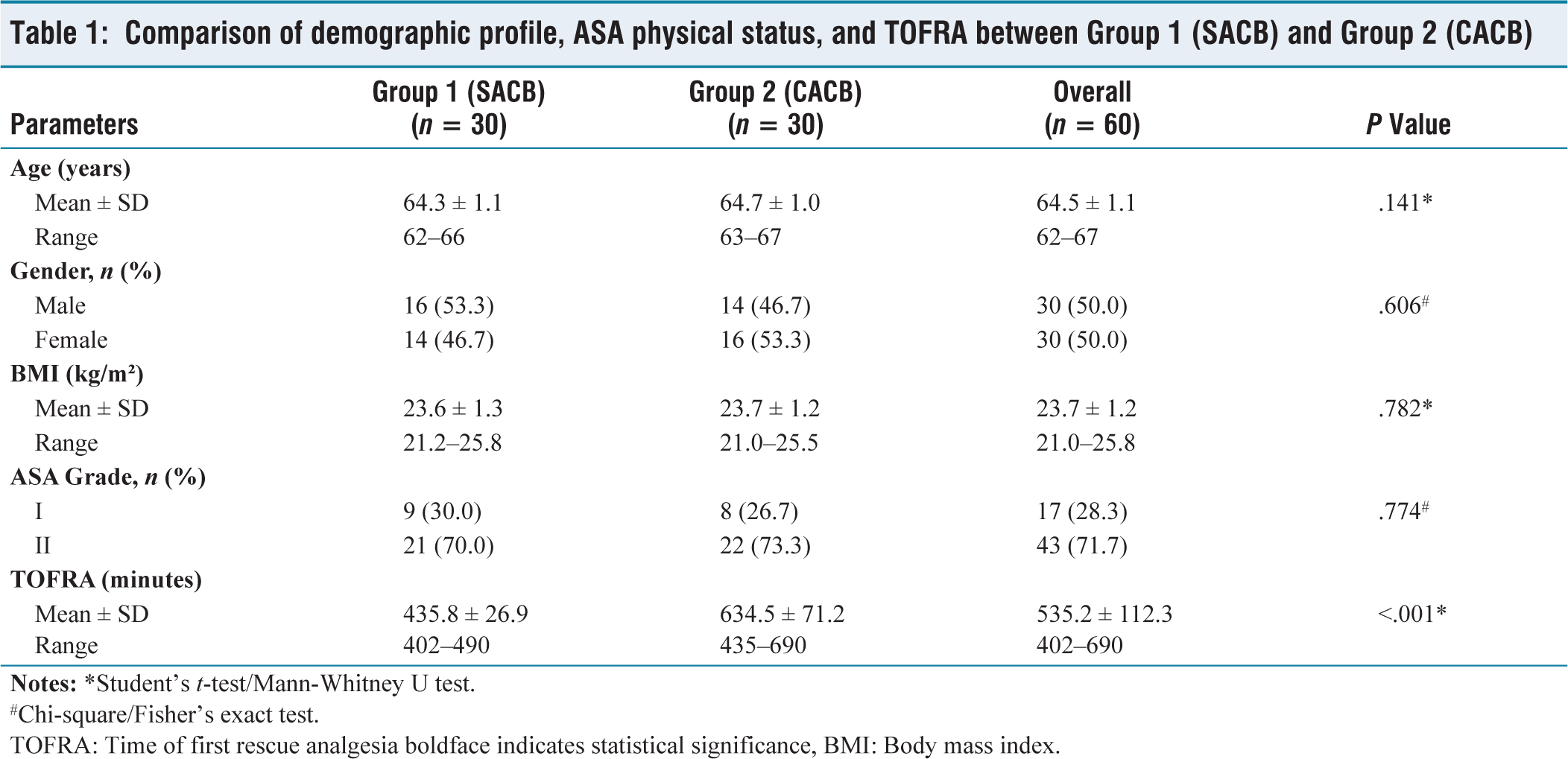
With 30 patients in each group, the study included 60 patients who had unilateral robotic complete knee replacements. The demographic characteristics and baseline parameters of the study population are presented in Table 1.
Comparison of demographic profile, ASA physical status, and TOFRA between Group 1 (SACB) and Group 2 (CACB)
#Chi-square/Fisher’s exact test.
TOFRA: Time of first rescue analgesia boldface indicates statistical significance, BMI: Body mass index.
The mean age of patients in Group 1 (SACB) was 64.3 ± 1.1 years, which was slightly lower than Group 2 (CACB) at 64.7 ± 1.0 years (P = .041). Gender distribution was comparable between the groups, with Group 1 having 16 males (53.3%) and 14 females (46.7%), while Group 2 had 14 males (46.7%) and 16 females (53.3%) (P = .606).
The mean BMI was similar between the groups, with Group 1 at 23.6 ± 1.3 kg/m² and Group 2 at 23.7 ± 1.2 kg/m² (P = .782). Most patients in both groups were classified as ASA II (70.0% in Group 1 and 73.3% in Group 2), with no significant difference in ASA distribution between the groups (P = .774).
Group 2 (CACB) demonstrated a significantly longer length of 634.5 ± 71.2 minutes compared to Group 1 (SACB) at 435.8 ± 26.9 minutes (P < .001), indicating a statistically significant difference between the groups in the time to first rescue analgesia (TOFRA).
Pain Scores (VAS)
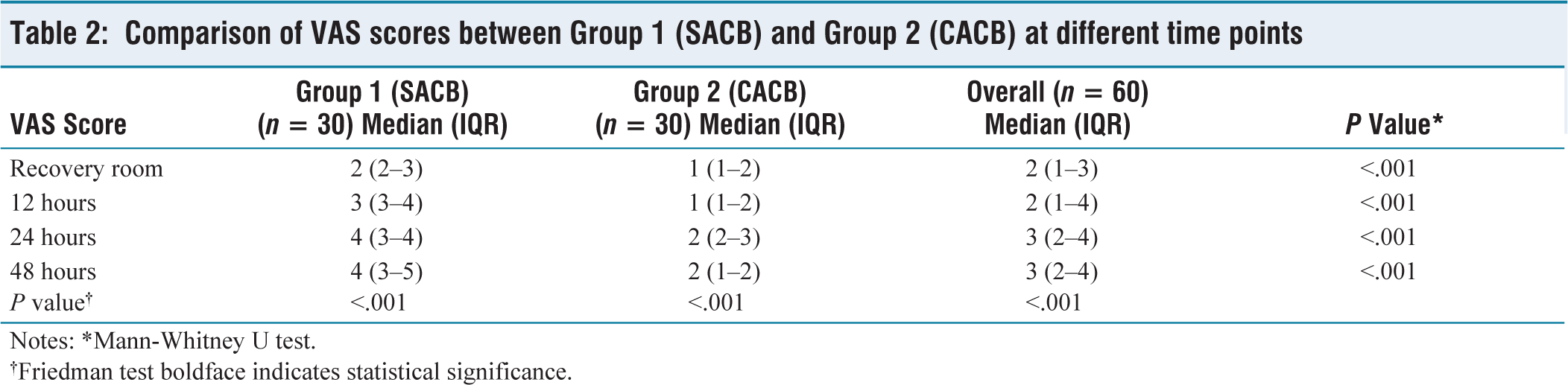
The VAS was used to measure postoperative pain levels at four different intervals in time: during recovery and 12 hours, 24 hours, and 48 hours after surgery. Table 2 presents the findings.
Comparison of VAS scores between Group 1 (SACB) and Group 2 (CACB) at different time points
†Friedman test boldface indicates statistical significance.
In the recovery room, Group 2 (CACB) patients had significantly lower median VAS scores of 1 (IQR: 1–2) compared to Group 1 (SACB) patients who had median scores of 2 (IQR: 2–3) (P < .001). This pattern of lower pain scores in Group 2 continued at all subsequent time points.
At 12 hours postoperatively, the median VAS score for Group 1 increased to 3 (IQR: 3–4), while Group 2 maintained a median score of 1 (IQR: 1–2) (P < .001). At 24 hours, Group 1 showed a further increase to a median score of 4 (IQR: 3–4), while Group 2 had a median score of 2 (IQR: 2–3) (P < .001). The most substantial difference was observed at 48 hours, with Group 1 maintaining a median score of 4 (IQR: 3–5) compared to Group 2 with a median score of 2 (IQR: 1–2) (P < .001).
The Friedman test showed statistically significant changes in VAS scores over time within both groups (P < .001), indicating a temporal pattern in pain intensity during the postoperative period.
Pairwise Comparison of VAS Scores at Different Time Points
The Wilcoxon signed-rank test was performed to compare VAS scores between consecutive time points within each group. The results are presented in Table 3.
Pairwise comparison of VAS scores at different time points within each group

In Group 1 (SACB), there were statistically significant increases in pain scores between all consecutive time points: from recovery room to 12 hours (P < .001), from 12 hours to 24 hours (P < .001), and from 24 hours to 48 hours (P = .046).
In contrast, Group 2 (CACB) showed no significant change in pain scores between the recovery room and 12 hours (P = .157), indicating stable analgesia during this period. A significant increase was noted between 12 hours and 24 hours (P < .001), but the change between 24 hours and 48 hours lacked statistical significance (P = .083), suggesting stabilisation of pain levels after 24 hours in the CACB group.
Distribution of Time to First Rescue Analgesia
The distribution of the TOFRA between the two groups is presented in Table 4.
Distribution of TOFRA in minutes

The distribution shows a clear separation between the two groups, with minimal overlap. In Group 1 (SACB), all patients required rescue analgesia within 500 minutes, with the majority (66.7%) needing it between 400 minutes and 450 minutes. In contrast, Group 2 (CACB) showed a wider distribution, with 73.3% of patients requiring rescue analgesia after 550 minutes, and nearly a quarter (23.3%) extending beyond 650 minutes.
The prolonged analgesic efficacy offered by the CACB in comparison to the single-shot approach is shown by this substantial difference in TOFRA (P < .001).
Discussion
Effective pain management following TKR is crucial for optimal recovery, early mobilisation, and improved functional outcomes. Our study aimed to compare the analgesic efficacy of SACB versus CACB, both combined with posterior capsular infiltration, in patients undergoing unilateral robotic TKR. The results demonstrate the superior analgesic efficacy of CACB with posterior capsular infiltration across all measured time points.
The demographic characteristics of our study population were comparable between the two groups, with a slight but statistically significant difference in age (Group 1: 64.3 ± 1.1 years vs. Group 2: 64.7 ± 1.0 years, P = .041). This minimal age difference is unlikely to have clinical significance or impact on the study outcomes. The gender distribution, BMI, and ASA physical status were also comparable between the groups, suggesting that the observed differences in pain scores and TOFRA can be attributed to the different analgesic techniques employed rather than patient characteristics.
One of the most striking findings of our study was the significantly longer TOFRA in the CACB group compared to the single-shot group (634.5 ± 71.2 minutes vs. 435.8 ± 26.9 minutes, P < .001). This represents a difference of approximately 3.3 hours, which is clinically significant in the context of postoperative pain management. This finding aligns with the results of Zhang et al.[4] who conducted a PRISMA-compliant meta-analysis and discovered that, when compared to single-shot methods, continuous ACB offers superior analgesia over a 48 hour period.
The VAS pain scores in our study demonstrated consistently lower values in the continuous block group at all time points, with the most pronounced differences observed at 24 hours and 48 hours postoperatively. This temporal pattern is particularly noteworthy as it suggests that while SACB provides reasonable analgesia in the immediate postoperative period, its effect diminishes over time, resulting in progressively increasing pain scores. In contrast, continuous ACB maintains a more stable level of analgesia throughout the observation period.
This pattern of ongoing approaches for persistent analgesia is consistent with Sercia et al.’s[12] findings, who reported that continuous (ACB) significantly decreased 48 hour pain scores compared to single-shot techniques. Similarly, Sun et al.[5] concluded in their GRADE analysis that continuous catheter (ACB) provides better analgesic efficacy than a single-shot block in primary TKR.
Interestingly, we observed that pain scores in the continuous block group did not significantly change between the recovery room and 12 hours postoperatively (P = .157), suggesting stable analgesia during this period. This finding has important clinical implications, as the immediate postoperative period is critical for initiating early mobilisation and rehabilitation protocols. Stable pain control during this phase may facilitate earlier physical therapy interventions and potentially improve functional outcomes.[13]
The combined posterior capsular infiltration and ACB in both groups most likely helped both groups achieve the overall successful pain control that our study found. A major source of pain after TKR that may not be sufficiently addressed by ACB alone is the posterior knee capsule, which is densely innervated by tibial nerve branches.[3] Local anaesthetic infiltration in this area has been shown to provide accelerated rehabilitation and reduce opioid consumption post-procedure.[4,13]
Our results are in line with those of Rajkumar et al.[10] who demonstrated that a combination of ACB with posterior capsular local infiltration results in improved pain management, good range of motion, faster recovery, and less narcotic use compared to either technique alone. Similarly, Li et al.[10] found that multi-site infiltration analgesia, when combined with ACB, provides superior pain management and early rehabilitation compared to peripheral nerve blocks alone.
Wang et al.[6] conducted a meta-analysis of randomised controlled trials and concluded that continuous ACB is a better choice compared to single-shot block after primary TKR, which aligns with our findings. They noted that continuous techniques not only provided better analgesia but also improved functional recovery parameters.
In contrast to our findings, Hussain et al.[5] reported in their systematic review and meta-analysis that continuous ACB provided no significant advantage over SACB in terms of analgesia, pain management, functional recovery, or opioid-related side effects during the first 48 hours postoperatively. This discrepancy may be attributed to differences in study populations, surgical techniques (robotic vs. conventional TKR), and the addition of posterior capsular infiltration in our study protocol.
The use of robotic assistance in TKR in our study population may have influenced the postoperative pain profile and the efficacy of the analgesic techniques. Robotic TKR has been associated with improved precision in component positioning and alignment, potentially resulting in different soft tissue trauma patterns compared to conventional techniques.[1] This highlights the importance of evaluating analgesic techniques specifically in the context of evolving surgical technologies.
The clinical implications of our findings are significant. When paired with posterior capsular infiltration, the prolonged length of analgesia offered by a CACB may enable earlier and more efficient engagement in rehabilitation programs, which could result in better functional outcomes and shorter hospital stays. The delay in requiring rescue analgesia may also contribute to reduced opioid consumption, which is particularly important in light of ongoing concerns about opioid use and its associated adverse effects.[4]
However, it is important to acknowledge that continuous catheter techniques require additional resources, expertise, and monitoring compared to single-shot blocks. Factors, such as cost-effectiveness, resource availability, and individual patient characteristics should be considered when selecting the optimal analgesic approach for TKR patients.
Several limitations of our study warrant consideration. First, the retrospective design inherently introduces potential selection bias and confounding factors. Second, our follow-up was restricted to 48 hours after surgery, making it impossible to evaluate longer-term outcomes including patient satisfaction, hospital stay duration, and functional recovery. Third, we did not specifically evaluate the impact of the different analgesic techniques on mobilisation, rehabilitation protocols, or opioid consumption, which are important aspects of postoperative recovery. Finally, our study was conducted at a single centre with expertise in robotic TKR, which may limit the generalizability of our findings to other settings.
Future prospective randomised controlled trials with larger sample sizes, extended follow-up periods, and comprehensive outcome measures including functional recovery parameters, opioid consumption, patient satisfaction, and cost-effectiveness would provide more robust evidence to guide clinical practice in this evolving field.
Conclusion
In patients having unilateral robotic TKR, our study shows that continuous ACB, when paired with posterior capsular infiltration, offers better analgesic efficacy than SACB. The continuous technique resulted in consistently lower pain scores at all measured time points and significantly delayed the requirement for rescue analgesia.
While both techniques provide effective analgesia in the immediate postoperative period, the continuous ACB maintains superior pain control beyond 24 hours, which may be particularly important for facilitating rehabilitation during this critical phase of recovery. In order to provide complete pain management, the combination of posterior capsular infiltration treats posterior knee discomfort that may not be sufficiently addressed by ACB alone.
For patients having robotic TKR, our results lend credence to the efficacy of CACB with posterior capsular infiltration as an analgesic technique. However, the selection of the optimal analgesic approach should consider individual patient factors, resource availability, and institutional expertise.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
IEC-BMR Application No.: AMH-C-S-009/02-25.
Informed consent
Not applicable.
Credit author statement
Not applicable.
Data availability
Not applicable.
Use of artificial intelligence
Not applicable.