
Abstract
Background:
Total hip replacement (THR) is a common procedure for treating osteoarthritis that can result in significant postoperative pain. Effective pain management is critical for optimising recovery and rehabilitation outcomes. This study compared the analgesic efficacy between continuous suprainguinal fascia iliaca block versus continuous lumbar plexus block in patients undergoing unilateral total hip replacement surgery.
Methods:
This retrospective study included 60 patients who underwent unilateral total hip replacement surgery between December 2023 and December 2024. Two groups of thirty patients each were formed from the patients. Group 1 received a continuous suprainguinal fascia iliaca block, while Group 2 received a continuous lumbar plexus block. The primary outcome of this study was to measure the postoperative pain assessed using the Visual Analogue Scale (VAS) in the postoperative period at 30 minutes, 1 hour, 2 hours, 6 hours, 12 hours, 24 hours, 36 hours and 48 hours.
Results:
In terms of ASA physical status and demographic traits, both groups were similar. Group S (continuous suprainguinal fascia iliaca block) demonstrated a significantly lower VAS pain score compared to Group L (continuous lumbar plexus block). Group L required substantially more rescue analgesia than Group S (P < .001).
Conclusion:
For patients having unilateral complete hip replacement surgery, continuous suprainguinal fascia iliaca block offers better analgesia than continuous lumbar plexus block. The need for rescue analgesia is less in patients availing continuous suprainguinal fascia iliaca block than continuous lumbar plexus block. This enhanced pain management approach may contribute to improved rehabilitation outcomes and shorter hospital stays.
Keywords
Introduction
One of the most economical and reliably successful orthopaedic procedures is total hip arthroplasty (THA). For individuals with end-stage degenerative hip osteoarthritis, it offers consistent results. In particular, it leads to better quality of life, pain reduction and functional restoration.[1]
Since it has been demonstrated to affect the final result, the underlying diagnosis that causes a degenerative hip is a crucial factor to take into account. THA consistently reduces pain both temporarily and permanently and produces favourable clinical and functional results as reported by patients. Generally speaking, THA yields even more dependable and constantly favourable outcomes than its equivalent operation, total knee arthroplasty (TKA).[2,3]
Ultrasound (US)-guided suprainguinal fascia iliaca block (SIFIB), initially introduced in 2011, targets the inguinal ligament from the fascia iliaca compartment cephalad.[4] A fascia iliaca block applies a local anaesthetic to the plane between the fascia iliaca and the iliacus muscle below, which contains the femoral nerve and lateral femoral cutaneous nerve (LFCN). It is used for hip, knee and thigh anaesthesia and pain relief.[5]
One anaesthetic option for older adults having hip surgery is lumbar plexus block (LPB). Because LPB targets the somatic nerve in the psoas area, it may be safe. The adequate analgesia administered both during and after surgery is what makes LPB so effective. The term ‘acceptability’ refers to the degree of muscular relaxation and immobility after surgery.[6]
In this article, we compared the pain score between the continuous suprainguinal fascia iliaca block versus continuous lumbar plexus block in patients undergoing unilateral total hip replacement surgeries.
Materials and Methods
Study Design
This is a retrospective study analysing data from patients who underwent unilateral total hip replacement surgery between December 2023 and December 2024.
Study Population
All patients who underwent unilateral total hip replacement surgery during the study period and who met the inclusion and exclusion criteria were included.
Sample Size
A total of 60 patients who satisfied the inclusion and exclusion criteria were included in the study, with 30 patients in each group:
Group L: Continuous lumbar plexus block group Group S: Continuous suprainguinal fascia iliaca block group
Inclusion Criteria
Patient undergoing unilateral total hip replacement surgery
Patients over 18 years of age
ASA grade I-III
Exclusion Criteria
Chronic opioid addiction and/or use of other kinds of analgesic drugs for more than 3 months
Inability to communicate due to severe dementia, language barrier or end-stage disease
Nerve block contraindications such as infection in the puncture site or severe coagulation dysfunction
Allergic to local anaesthetics
Aim
Our study aimed to determine the most effective method of analgesia for patients undergoing unilateral total hip replacement surgery by comparing continuous suprainguinal fascia iliaca block and continuous lumbar plexus block.
Objectives
Primary objective: To compare the postoperative pain score using the Visual Analog Scale (VAS) between the two groups.
Secondary objective: To document and compare the requirement of rescue analgesia between the groups.
Study Procedure
All patients received a standardised anaesthetic protocol consisting of spinal anaesthesia with 0.5% Bupivacaine heavy (12.5-15 mg) and underwent unilateral total hip replacement surgery by the same surgical team using the same surgical technique. Group S received ultrasound-guided continuous suprainguinal fascia iliaca block with an initial bolus of 20 ml of 0.15% ropivacaine, followed by infusion at a rate of 6 ml/hr post-surgery. Group L received an ultrasound-guided continuous lumbar plexus block with an initial bolus of 20 ml of 0.15% ropivacaine, followed by infusion at a rate of 6 ml/hr post-surgery.
Postoperative Management
All patients received a standard multimodal analgesic regimen consisting of
Intravenous paracetamol 1 g every 8 hours Intravenous ketorolac 30 mg every 12 hours for the first 24 hours, followed by oral celecoxib 200 mg twice daily
Rescue analgesia is administered as intravenous tramadol 50 mg when the VAS score is 7 and above, or when requested by the patient.
Data Collection
Data were collected from patient records, including demographic information such as age, gender, height, weight and ASA physical status. Pain scores were assessed using the Visual Analog Scale (VAS) at multiple time points: 30 minutes after surgery, 1 hour, 2 hours, 6 hours, 12 hours, 24 hours, 36 hours and 48 hours postoperatively. The need for requirement of rescue analgesics was also documented. The study protocol received approval from the Institutional Ethics Committee, and as a retrospective study using existing data, individual patient consent was not required. However, all patient data were anonymised and handled with strict confidentiality in accordance with institutional guidelines.
Methodology
All patients who underwent unilateral total hip replacement surgery between December 2023 and December 2024 and who satisfy inclusion and exclusion criteria are taken in this study. Two groups were formed out of them. Continuous lumbar plexus block was administered to one group, whereas continuous suprainguinal fascia iliaca block was administered to the other. The postoperative pain scores were documented with the VAS scores, and the need for requirement of rescue analgesia was noted. This was done periodically at 30 minutes after the surgery, 1 hour, 2 hours, 6 hours, 12 hours, 24 hours, 36 hours and 48 hours. In this way, the two groups were compared for analgesic efficacy.
Statistical Analysis
Summary statistics were presented with Mean ± SD and frequency (percentage) for the continuous and categorical factors, respectively. The median (IQR) was presented for the Visual analogue score. Student’s t-test/Mann Whitney U test was used to determine the significant changes between the two blocks. The relationship between two independent categorical variables was ascertained using the Chi-Square/Fisher’s exact test. Significant changes over time were identified using the Friedman test. P value < .05 is considered as statistically significant. All the statistical analysis was computed by using SPSS (IBM, 28.0)
Results
A total of 60 patients who underwent unilateral total hip replacement surgery were included in the study, with 30 patients in each group. The demographic characteristics and baseline parameters of the study population are presented in Table 1.
Demographic factors
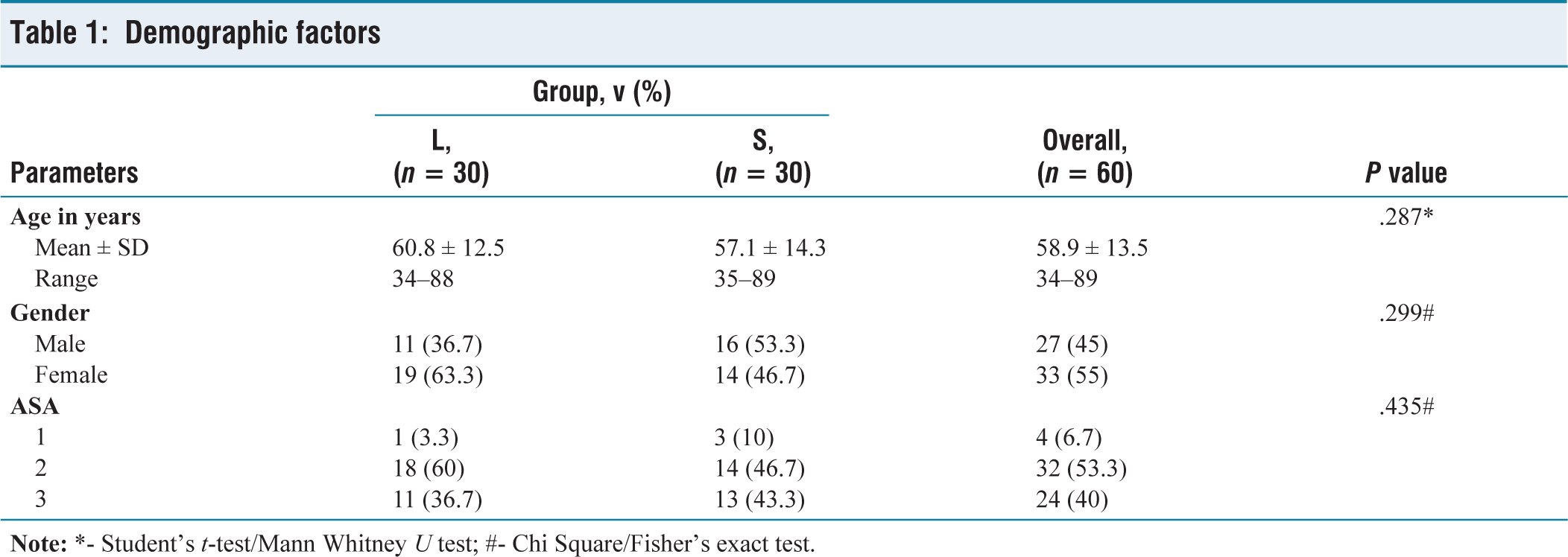
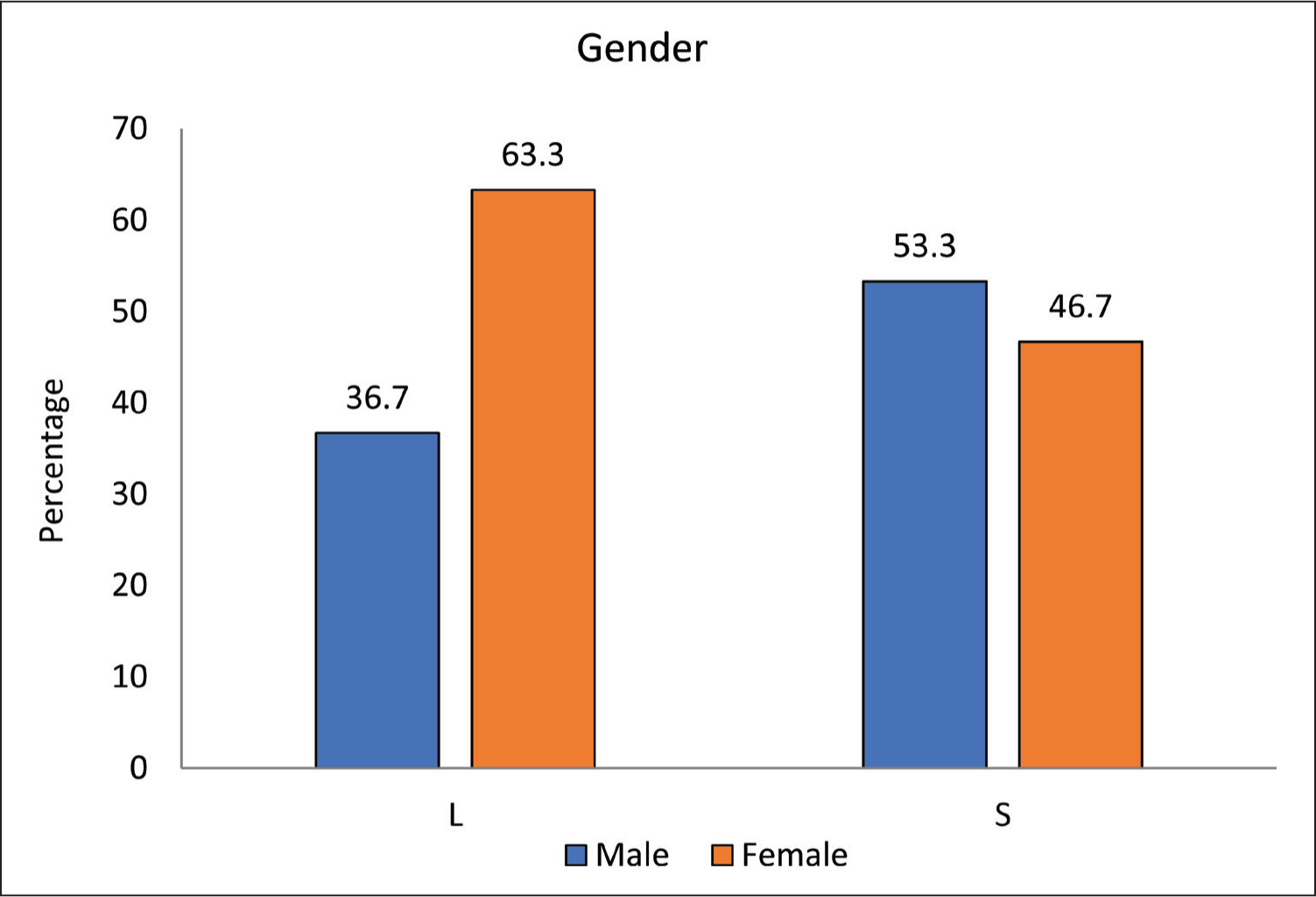
The mean age of patients in Group L was 60.8 ± 12.5 years, which was slightly higher than Group S, which was 57.1 ± 14.3 years (P = .287). Gender distribution was comparable between the groups, with Group L having 11 males (36.7%) and 19 females (63.3%), while Group S had 16 males (53.3%) and 14 females (46.7%). The number of ASA 1 in Group L is 1 patient, and Group S is 3 patients. The number of ASA 2 in Group L is 18 patients, and Group S is 14 patients. The number of ASA 3 in Group L is 11 patients, and Group S is 13 patients. The gender distribution is depicted in Figure 1.
Bar chart for gender distribution between the groups
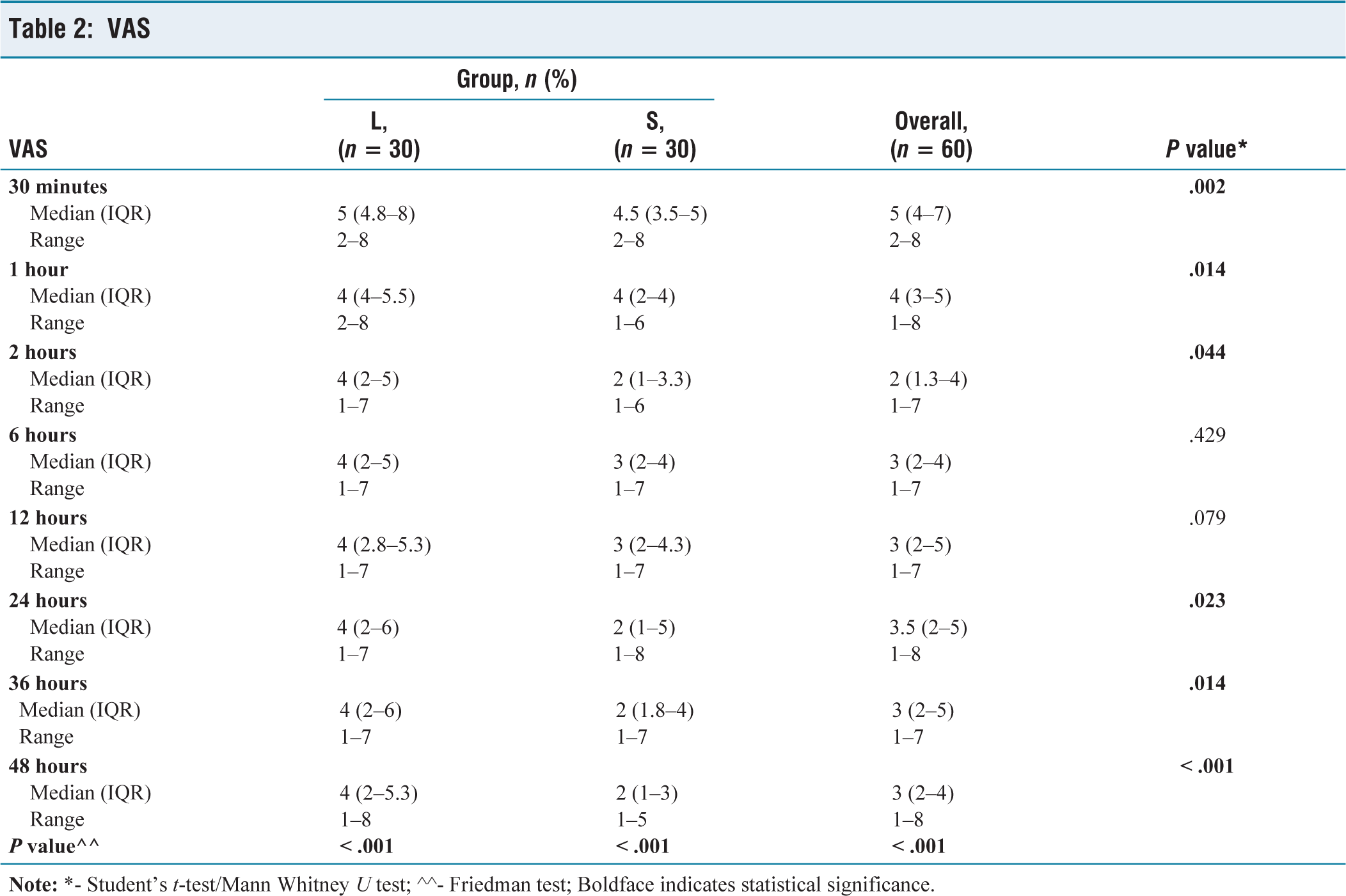
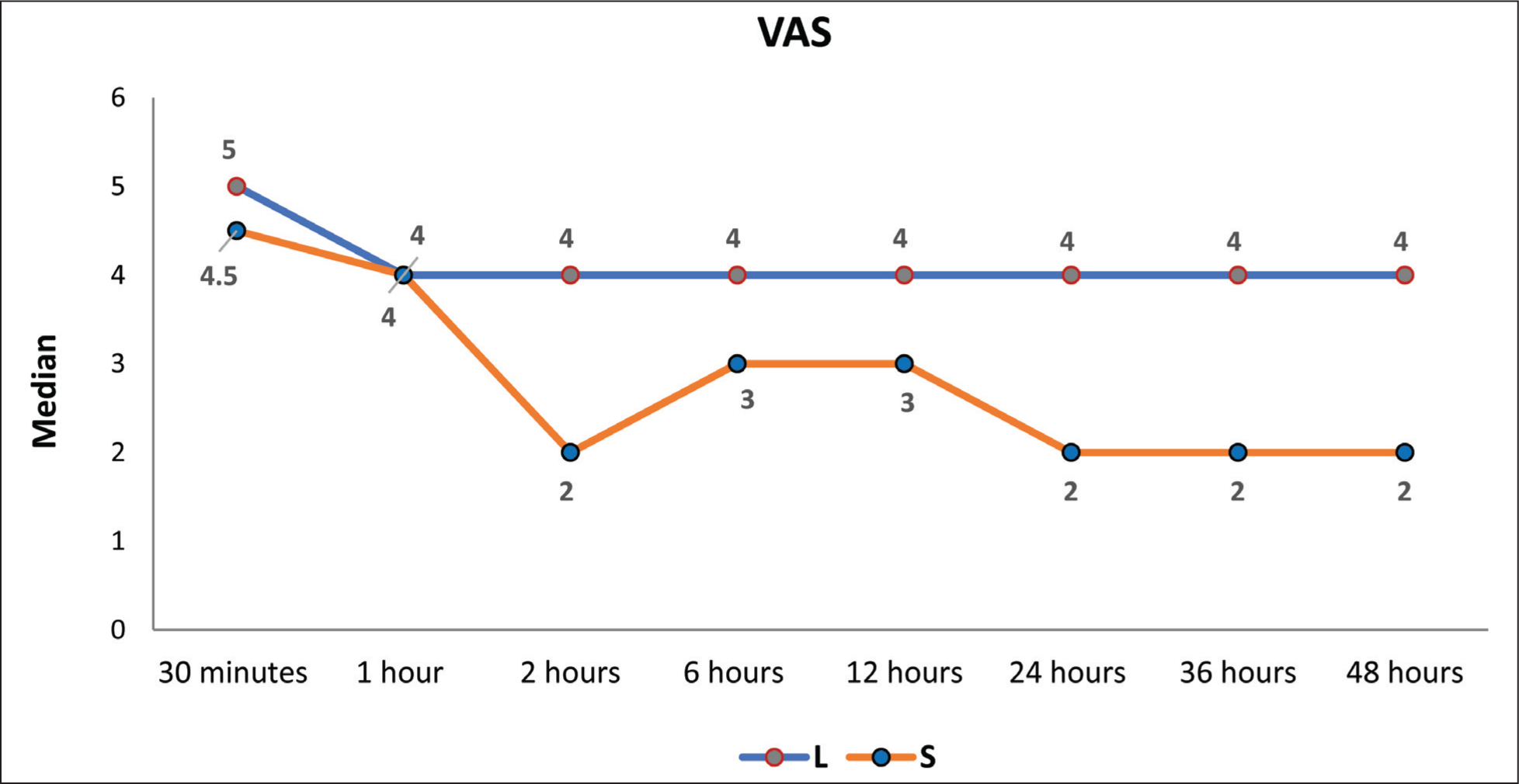
The VAS score at 30 minutes post-surgery is significantly high in the L group, with a P value of .002. The VAS score at 1-hour post-surgery is significantly high in the L group with a P value of .014. The VAS score at 2 hours post-surgery is statistically significant with a P value of .044. The comparison of VAS scores at 6 hours and 12 hours postoperatively is not statistically significant. However, at 24 hours, 36 hours and 48 hours postoperatively, the VAS score between the two groups shows an increasing trend of statistical significance with a high score in Group L compared to Group S. These VAS score comparisons were explained in Table 2, and the median VAS score is depicted in Figure 2.
VAS
Line graph of median value trend of VAS score between the groups
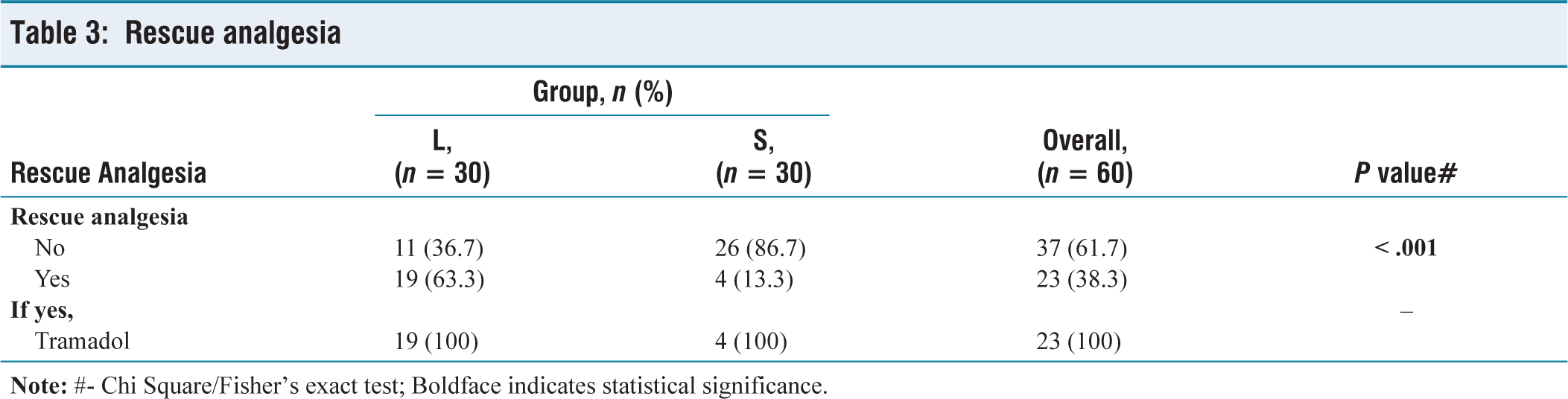
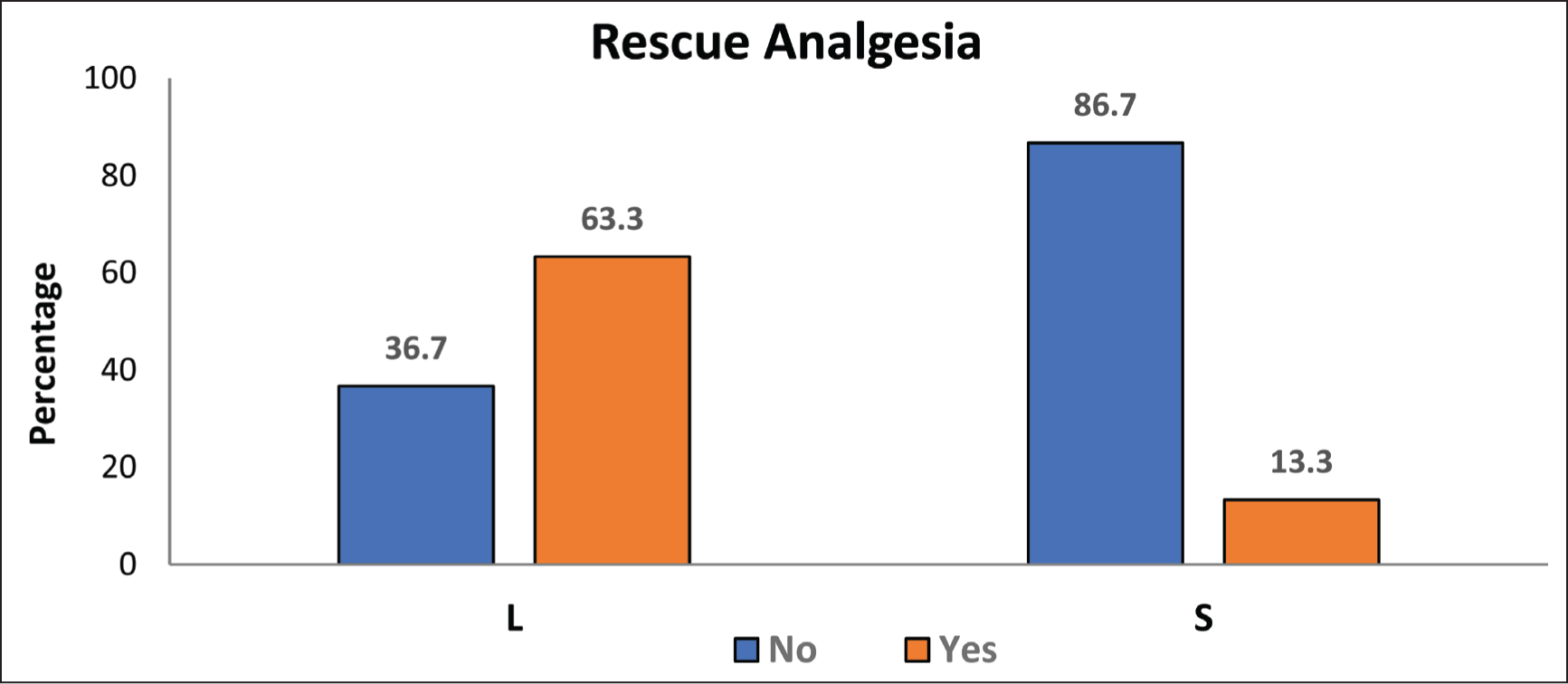
The need for the requirement of rescue analgesia between two groups shows that it is significantly high in Group L when compared to Group S with a P value < .001. Patients with VAS scores more than or equal to 7 were given rescue analgesia, which is an injection of Tramadol 50 mg given intravenously. Out of 30 participants in Group L, 19 patients had the requirement for rescue analgesia. Whereas in Group S, only 4 patients had the requirement for rescue analgesia. This is depicted in Table 3 and Figure 3.
Rescue analgesia
Bar chart for distribution of requirement of rescue analgesia between the groups
Discussion
For the best healing, early mobilisation and enhanced functional results after total hip replacement surgery, pain management is essential. Our study aimed to compare the analgesic efficacy between the continuous suprainguinal fascia iliaca block versus the continuous lumbar plexus block. The results demonstrate the superior analgesic efficacy of continuous suprainguinal fascia iliaca block over continuous lumbar plexus block.
The demographic factors between both groups were comparable. One of the striking findings of our study is the very low requirement of need for rescue analgesia in Group S compared to Group L since the VAS score is higher in patients in Group L than in Group S.
Comparing different regional anaesthetic procedures for hip surgery among the analysed studies revealed important information about their efficacy, safety and usefulness.
D. Bravo et al. (2020)[7] compared US-guided LPB with SIFIB in patients having total hip replacements in their randomised experiment. Their results imply that SIFIB may lead to a prolonged sensory block, even if they did not find any appreciable variations in terms of pain management or breakthrough opioid demand. They hypothesise that the comparatively avascular fascia iliaca compartment is the cause of this longer block duration. Conversely, the psoas muscle, which is where LA is deposited for LPB, would have more vascularisation, which would speed up the resorption of LA molecules. However, here in our study, we are comparing continuous blocks instead of single shot blocks compared in the above study.
Numerous research assessed the lumbar plexus block (LPB) and fascia iliaca block (FIB). According to Badiola et al. (2018),[8] even though the FIB group consumed more opioids right after surgery, FIB was not inferior to LPB in terms of post-arthroscopy pain management.
Vichainarong et al. (2024)[9] reported additional comparisons between SIFIB and PENG blocks and found no discernible difference in pain ratings or fentanyl usage between the two following THA. However, the quadriceps strength of the PENG group was better maintained. In their comparison of LPB with SIFIB in juvenile hip/femur operations, DeLong et al. (2021)[10] found that SIFIB was safer and easier to use, with shorter procedure times and marginally improved pain scores.
In their 2022 study, Azizoğlu and Rumeli[11] compared SIFIB to epidural analgesia (EA). SIFIB showed comparable overall analgesia with fewer side effects, such as hypotension, although EA had lower pain scores after 18 hours, indicating its use in situations where EA presents hazards.
Lastly, Lu et al. (2018)[12] came to the conclusion that, particularly at longer postoperative intervals, LPB provides superior hemodynamic stability and postoperative analgesia in older hip replacement patients when compared to FIB.
In conclusion, PENG may provide better motor preservation, but SIFIB is a more adaptable, safer and efficient substitute for LPB and EA. It is especially praised for its simplicity of administration and lack of adverse effects.
Several limitations of our study warrant consideration. First, the retrospective design inherently introduces potential selection bias and confounding factors. Second, our follow-up was limited to 48 hours postoperatively, which precludes assessment of long-term outcomes such as functional recovery, length of hospital stay and patient satisfaction. Third, we did not specifically analyse the impact of the different analgesic techniques on mobilisation or rehabilitation protocol, which are important aspects of postoperative recovery. Lastly, the fact that our study was limited to a single THR-focused institution may have limited the applicability of our findings in other contexts. Future prospective randomised controlled trials with larger sample sizes, extended follow-up periods and comprehensive outcome measures, including functional recovery parameters, patient satisfaction and cost-effectiveness, would provide more robust evidence to guide clinical practice in this evolving field.
Conclusion
Our study demonstrates that continuous suprainguinal fascia iliaca block provides superior analgesic efficacy compared to continuous lumbar plexus block. However, the selection of the optimal analgesic approach should consider individual patient factors, resource availability and institutional expertise.
Footnotes
Acknowledgements
To the Research department, Apollo Hospitals, Chennai.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval
Institutional ethical committee approval has been obtained.
IEC – BMR Application No. AMH-C-S-010/02-25.
Informed consent
As this is a retrospective study using the existing data, informed consent from individual patients were not obtained. However, patient data will be anonymised and treated with strict confidentiality.
Credit author statement
Participated in data acquisition, literature research, investigations, data analysis and manuscript preparation. Participated in conceptualisation, investigation, supervision, data analysis and manuscript editing.
Both the authors have reviewed and approved the manuscript.
Data availability
Data presenting the study’s findings is available with the corresponding author.
Use of artificial intelligence
No.