
Abstract
Background:
Chronic rhinosinusitis (CRS) is a significant health concern that impacts approximately 5%–12% of the overall population. Presently, rhinosinusitis is defined as the presence of characteristic symptoms and objective proof of mucosal inflammation as demonstrated by diagnostic nasal endoscopy (DNE) or computerised tomography scan paranasal sinuses (CT scan PNS). Despite limitations, nasal endoscopy and CT have transformed our understanding and approach in treating CRS.
Objectives:
The purpose of this study is to compare the diagnostic efficacy of nasal endoscopy with CT of PNS to diagnose CRS.
Methods:
A prospective study was conducted at Apollo Main Hospital, Chennai, Tamil Nadu, India, including patients with symptoms suggestive of CRS between August 2022 and May 2024. DNE findings were compared with CT PNS findings using Lund–Mackay and modified Lund-Kennedy scoring systems.
Results:
Among 60 patients, DNE showed a sensitivity of 69.6% (left nostril), 85.2% (right nostril) and a specificity of 85.7% (left nostril), 100% (right nostril). It was statistically significant with CT PNS (P value <0.001).
Introduction
Chronic rhinosinusitis (CRS) is a significant health concern that impacts approximately 5%–12% of the overall population.[1] It is an inflammation of the sinonasal mucosa. This inflammation often leads to a range of symptoms, including nasal discharge, nasal block/obstruction, reduced sense/loss of smell and facial pain/pressure. In addition to causing physical discomfort, it continues to be a prevalent cause of morbidity, poor performance at work or school and social embarrassment. It also places a significant financial burden on the patient because of missed workdays resulting from doctor or hospital visits.[2]
The underlying mechanism of CRS is complex, involving multiple contributing factors, and not fully understood. It involves a complex interplay of host factors, environmental influences and microbial elements. The ostiomeatal complex (OMC) is a key area of interest as it consists of narrow channels and openings that connect various sinuses. These pathways can become obstructed due to anatomical variations, secretions, mucosal swelling, polyps and other factors. Such blockages impede sinus drainage, leading to stasis, inflammation and secondary infections, which subsequently produce symptoms.[3]
The European position paper on rhinosinusitis and nasal polyps (EPOS) now defines rhinosinusitis based on the presence of characteristic symptoms along with objective proof of inflammation of the mucosa. The criteria to diagnose CRS include at least one of the two symptoms of nasal block and purulent nasal discharge and at least one other symptom such as reduction of loss of smell or headache.[4] Radiographic evidence of paranasal sinus (PNS) inflammation and/or the presence of purulent mucus or oedema in the anterior ethmoid area or middle meatus, polyps in the middle meatus or nasal cavity are all objective proof of inflammation.[5]
Nasal endoscopy has become a further objective method of evaluating CRS, and it is now utilised in all centres globally to supplement physical examinations to confirm the disease’s diagnosis. It offers assistance in determining the mucosa’s integrity and in observing mucosal alterations, polyps, crusting and/or discharge up close.[6] The surgery field’s telescopic perspective provides a detailed view of both anatomical and pathological changes within the sinuses. It is feasible to observe the orbital walls and cribriform plate, which could result in orbital problems and cerebrospinal fluid (CSF) rhinorrhoea during the surgical procedure. Simultaneously, landmarks that can be used to guide the procedure through an endoscope can be defined to prevent these issues.[7]
Nevertheless, diagnostic nasal endoscopy’s (DNE) drawbacks include its incapacity to determine the disease’s extent within the ethmoidal sinus, its failure to detect disease in the middle meatus that is restricted and the existence of concealed air spaces such as posterior ethmoidal cells.[8]
Another significant and established study that has been conducted for decades and is considered the gold standard investigation for CRS is the CT scan. It effectively identifies areas that can demonstrate predisposing causes of CRS, such as anatomical variations, trauma and tumours, which may narrow the OMC and sinus drainage channels.[6] As this offers a ‘ROAD MAP’ to guide the surgical approach and steer the procedure, it is now required and a legal necessity to analyse the PNS and nasal cavity prior to functional endoscopic sinus surgery (FESS).[9] However, the danger of radiation exposure, high false positive rate and high expense are some of its drawbacks.[3] Thus, in recent years, endoscopy and computed tomography (CT) have transformed our understanding and approach to treating CRS.
In this study, we have compared the efficacy of nasal endoscopy with CT scan to diagnose CRS.
Aim and Objectives
The aim of this study was to compare the efficacy of DNE versus CT of PNS to diagnose CRS in a tertiary health care centre.
Materials and Methods
This prospective observational study was carried out from August 2022 to May 2024 in our institute’s Department of ENT and Head and Neck Surgery.
Inclusion Criteria
Patients aged more than 16 years of age with symptoms suggestive of CRS based on EPOS criteria, who consent to undergo CT scan PNS and endoscopic examination and patients who are radiologically (CT PNS) positive according to Lund–Mackay scoring system were included in the study.
Exclusion Criteria
Patients presenting with epistaxis, acute attacks of sinusitis, allergic symptoms, allergic fungal sinusitis and sinus malignancy were excluded from the study. Patients with past history of sinus surgery, dental implant surgery and maxillofacial surgery with plating, female patients who are pregnant, negative CT score according to Lund–Mackay scoring system and who are not willing to participate were also excluded from the study.
Methodology
A total of 60 patients were selected based on inclusion and exclusion criteria. A thorough history taking and ear, nose and throat examination were performed. Patients who were clinically diagnosed with CRS underwent CT PNS followed by DNE. CT PNS findings were recorded using Lund–Mackay scoring system. DNE was performed under topical anaesthesia spray by ‘3 pass technique’ and findings were noted using modified Lund-Kennedy scoring system.
Statistical Methods
Data entry was done in an MS Excel spreadsheet. Descriptive statistics were presented with frequency (percentage). Diagnostic accuracy with sensitivity, specificity, negative predictive value (NPV) and positive predictive value (PPV) was performed between CT and DNE. Kappa statistics were used to determine the agreement between CT and DNE findings. A P value < .05 is considered statistically significant. All the statistical analysis was carried out by using SPSS (IBM, 28.0)
Results
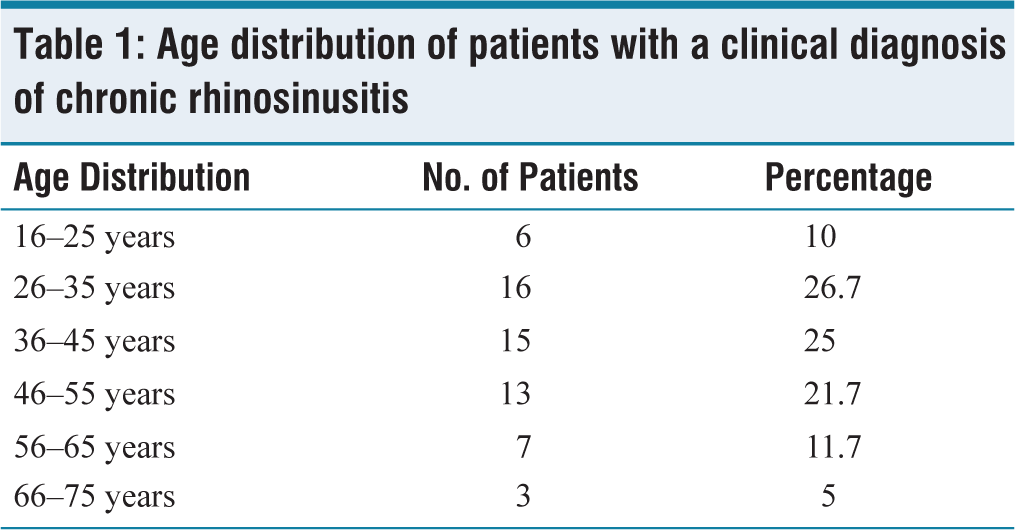
Out of 60 patients with CRS, 6 patients (10%) were aged between 16 and 25 years of age, 16 patients (26.7%) were aged between 26 and 35 years, 15 patients (25%) were aged between 36 and 45 years, 13 patients (21.7%) were aged between 46 and 55 years, 7 patients (11.7%) were aged between 56 and 65 years and 3 patients (5%) were aged between 66 and 75 years [Table 1].
Age distribution of patients with a clinical diagnosis of chronic rhinosinusitis
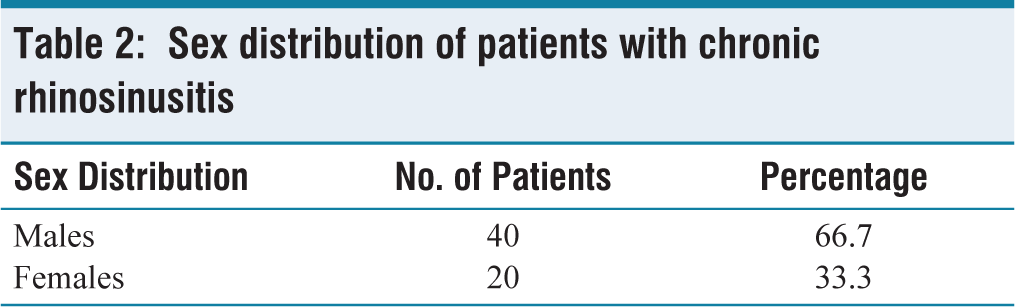
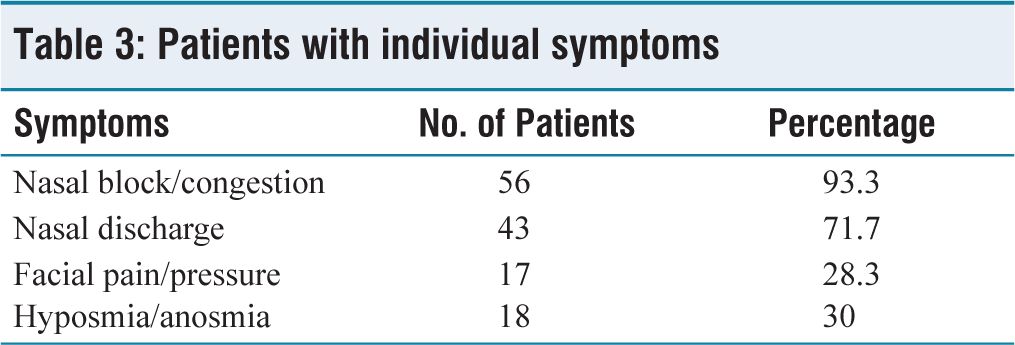
Tables 2 and 3 demonstrate sex distribution and individual symptoms in a group of 60 patients.
Sex distribution of patients with chronic rhinosinusitis
Patients with individual symptoms
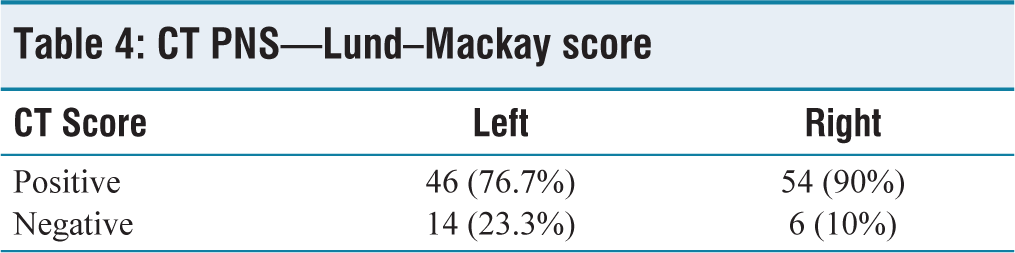
On CT scan PNS, left nostril showed a positive Lund–Mackay score in 46 patients (76.7%) and negative score in 14 patients (23.3%). Meanwhile, right nostril showed a positive Lund–Mackay score in 54 patients (90%) and negative score in 6 patients (10%) [Table 4].
CT PNS—Lund–Mackay score
On endoscopic examination, left nostril showed a positive modified Lund-Kennedy score in 34 patients (56.7%) and negative score in 26 patients (43.3%). Meanwhile, the right nostril showed a positive modified Lund-Kennedy score in 46 patients (76.7%) and negative score in 14 patients (23.3%) [Table 5].
DNE—Modified Lund–Kennedy score
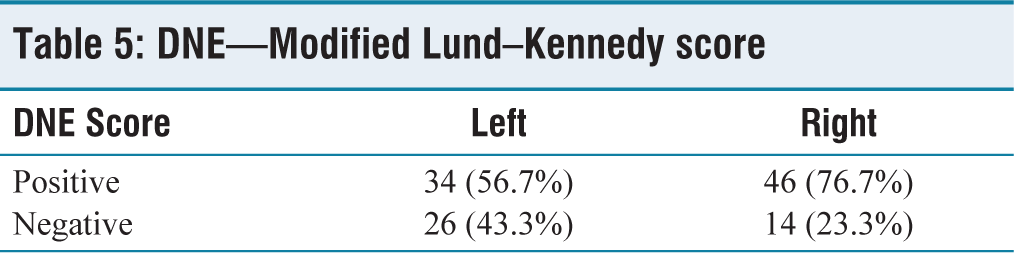
Table 6 reveals that DNE in the left nostril had 69.6% sensitivity and 85.7% specificity. There was a 46.2% NPV and 94.1% PPV.
Diagnostic accuracy between DNE score and CT PNS score in left nostril
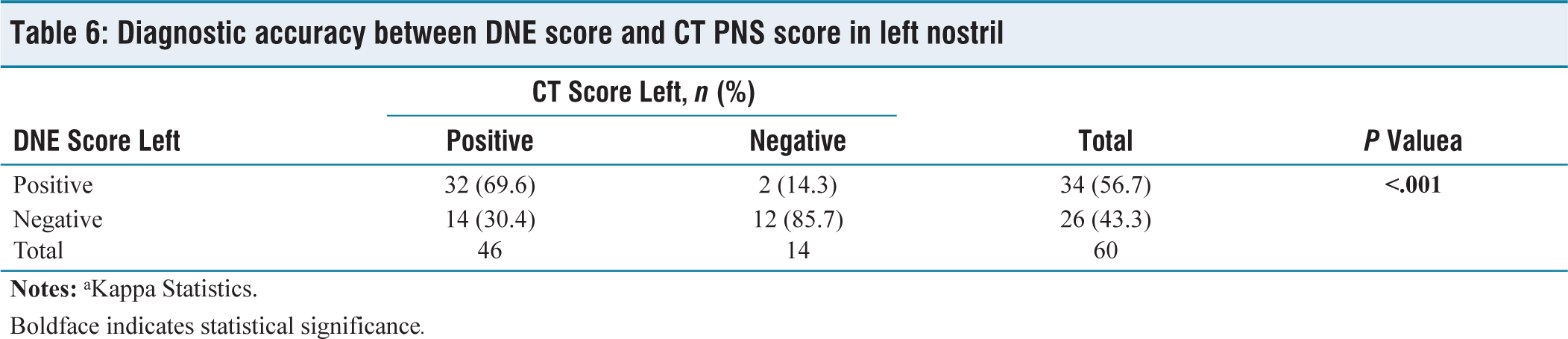
Boldface indicates statistical significance.
As indicated in Table 6, out of 60 patients with a clinical diagnosis of CRS, 46 had a positive Lund–Mackay score on a CT scan of the PNS in the left sinuses. Among these, 32 (69.6%) patients also had a positive score on DNE, and 14 (30.4%) had negative score on DNE. The remaining 14 patients had negative scores on CT scan. Of the remaining 14 patients with negative Lund–Mackay scores on CT, 12 (85.7%) had negative scores on DNE, while 2 (14.3%) had positive scores on DNE. The P value was <.001 which was statistically significant.
Table 7 reveals that DNE in the right nostril had 85.2% sensitivity and 100% specificity. There was a 42.9% NPV and 100% PPV.
Diagnostic accuracy between DNE score and CT PNS score in right nostril
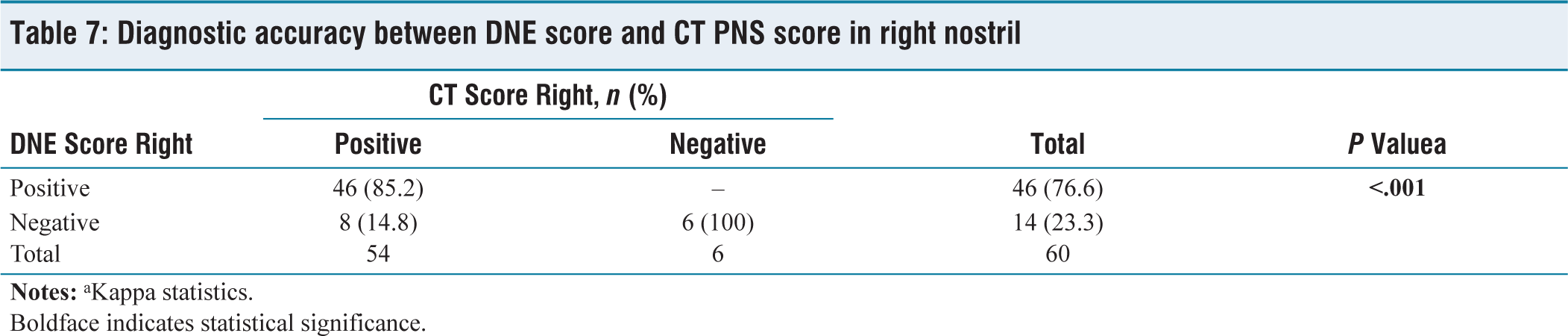
Boldface indicates statistical significance.
As shown in Table 7, among the 54 patients with a positive Lund–Mackay score on CT scan PNS in the right sinuses, 46 (85.2%) had a positive score on DNE, and 8 (14.8%) had negative score on DNE. Of the remaining 6 patients with negative score on CT scan, all 6 (100%) had negative score on DNE. The P value was <.001 which was statistically significant.
Discussion
Concurring with the previous studies done by Pratibha Krishniya et al.,[10] Ehtesham Ahmad Raushan et al.[11] and Nitin V. Deosthale et al.,[12] CRS was more predominant in 26–35 years of age.
In our study, CRS was more common in males (66.7%) than females (33.3%), which is in concurrence with previous studies by Priyanko Chakraborty et al.,[3] Peri Sreekavya et al.[13] and Pratibha Krishniya et al.[10]
The predominant symptom that the majority of patients present in our study is nasal block/congestion, which is concurring with previous studies by Priyanko Chakraborty et al.,[3] Vanitha Brindha Baba Caliaperoumal et al.,[2] Pratibha Krishniya et al.[10] and Peri Sreekavya et al.[13]
According to previous studies by Priyanko Chakraborty et al.,[3] Pratibha Krishniya et al.,[10] Karthika Nathan et al.[14] and Nitin V. Deosthale et al.,[12] the sensitivity and specificity of nasal endoscopy bilaterally were 78.08% and 66.67%, 93.18% and 83.33%, 92.31% and 72.33%, 94% and 86% respectively which were in concurrence with our study. It was statistically significant, indicating that the DNE is as effective as CT PNS in diagnosing CRS. In addition, in our study, we individually analysed both nasal cavities, wherein the sensitivity and specificity of nasal endoscopy on the left side were 69.6% and 85.7%, and 85.2% and 100% on the right side.
Conclusion
CRS is one of the most prevalent diseases seen in ENT practice. In our study, we conclude that the most common age group involved was 25–36 years. Majority of patients came with complaints of nasal block/congestion.
According to our study, we conclude that the DNE is as effective as CT PNS in diagnosing CRS. However, CT PNS is imperative preoperatively to rule out anatomical abnormalities such as sphenoid sinus pneumatisation, olfactory fossa and so on, and for delineating the extent of disease.
Limitations
The results were from a single tertiary care centre. A multi-institutional study might yield more information. Also, expanding the study to include a larger group may yield more reliable results.
List of abbreviations
CRS—Chronic rhinosinusitis
CRSwNPs—CRS with polyps
CRSsNPs—CRS without polyps
OMC—Ostiomeatal complex
EPOS—European position paper on rhinosinusitis and nasal polyps
FESS—Functional endoscopic sinus surgery
CSF—Cerebrospinal fluid
DNE—Diagnostic nasal endoscopy
CT—Computerised tomography
PNS—Paranasal sinuses
PPV—Positive predictive value
NPV—Negative predictive value
Footnotes
Credit author statement
KRS helped in acquisition, analysis and interpretation of data and drafting of the manuscript.
All the authors conceptualised and designed the study and revisited it for intellectual content and final approval of complete manuscript.
Data availability
Data supporting the findings of this study is available with the corresponding author.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
The study was approved by Institutional Ethics Committee – Bio Medical research, Apollo Hospitals, Chennai, and the IEC number is AMH-DNB- 051/08-22.
Informed consent
Consent to participation has been obtained from the patients before their enrolment into the study. Written informed consent has been obtained from all the patients who met the eligible criteria.
Use of artificial intelligence
Nil.