
Abstract
Background:
Multiple non-invasive and invasive diagnostic tests for thyroid swelling are available, but fine-needle aspiration cytology (FNAC) is considered the gold standard investigation before surgery. Histopathological examination of surgically excised thyroid swellings remains the definitive method for determining thyroid gland pathology. Despite its limitations, FNAC is widely used due to its availability, accuracy and cost-effectiveness.
Objectives:
This study aims to evaluate the diagnostic accuracy of FNAC in assessing thyroid swellings and to correlate FNAC findings with histopathological diagnoses.
Methods:
A retrospective study was conducted at Apollo Main Hospital, Chennai, India, including patients who underwent surgery for thyroid lesions between January 2019 and July 2023. FNAC results were compared with final histopathological diagnoses using sensitivity, specificity and κ-statistics for statistical analyses.
Results:
Among 99 patients, FNAC showed a sensitivity of 73.2%, specificity of 81% and accuracy of 77.8%. The agreement between FNAC and histopathology was statistically significant (κ 0.542; P < .001). However, discrepancies were noted: 11 neoplastic FNAC diagnoses were later found to be non-neoplastic, while 11 non-neoplastic FNAC diagnoses were upgraded to neoplastic upon histopathology.
Conclusion:
FNAC is effective for the initial evaluation of thyroid lesions but should be combined with clinical and radiological assessments for better accuracy. Further research with larger samples may enhance understanding of FNAC’s diagnostic reliability.
Keywords
Abbreviations
CT: computed tomography; FNAC: fine-needle aspiration cytology; HPE: histopathological examination; NPV: negative predictive value; PPV: positive predictive value
Introduction
Thyroid abnormalities are frequently encountered in surgical practice, with a global prevalence ranging from 4% to 7%. The likelihood of malignancy in thyroid goitres is estimated to be around 10%. It is more prevalent among women than men. Due to associated risks, it is not feasible to surgically remove all thyroid lesions.[1]
Numerous diagnostic tests, such as computed tomography (CT) scan, ultrasound and fine-needle aspiration cytology (FNAC), among others, are available for evaluating goitre. Definitive diagnosis necessitates a morphological assessment of the lesions, making FNAC and histopathological examination (HPE) essential tests. FNAC was initially described by Leyden in 1883. Martin and Ellis first documented the diagnosis of thyroid lesions through aspiration cytology in 1930.[2]
As per the recommended guidelines set forth by the American Thyroid Association and the National Comprehensive Cancer Network, FNAC should be employed as the primary diagnostic test due to its superior diagnostic accuracy and cost-effectiveness.[2] The role of FNAC is complementary to histopathology, and when used alongside clinical and radiological evaluations, it offers the most reliable initial assessment for guiding management decisions. While ancillary techniques such as immunohistochemistry, electron microscopy, cytogenetics and molecular biology have advanced the ability to achieve precise type-specific diagnoses, they are costly and not routinely performed, typically being reserved for complex cases. Therefore, FNAC remains a straightforward and efficient method for the initial tissue diagnosis of thyroid lesions.[3]
Nevertheless, challenges with FNAC include ensuring the representativeness of the sampled area, the adequacy of aspirated material and the quality of slide preparation. If these issues can be addressed effectively, FNAC remains the optimal method for diagnosing thyroid lesions.[3] Guidelines for fine-needle aspiration of thyroid nodule specimens by the Papanicolaou Society of Cytopathology aim to minimise the false-negative rate to prevent overlooking carcinomas. Their objective is to –achieve a false-positive rate of less than 3% and a false-negative rate of less than 2%.[4]
While American Thyroid Association guidelines are rigorously implemented in tertiary centres, adhering to these protocols can be challenging in primary and rural areas of developing countries like India. In India, individuals from remote regions often travel to metropolitan cities for treatment, as the availability of medical resources and standard training of medical specialists is not uniform. Due to these reasons, follow-up for these patients becomes challenging and almost impossible. This study examines the role of FNAC as a quick, inexpensive diagnostic tool and its impact on subsequent management in such scenarios.
Materials and Methods
This retrospective study was conducted in the Department of ENT and Head and Neck Surgery at our institute between January 2019 and July 2023.
Aims and Objectives
Clinical evaluation of various types of thyroid swellings and correlation between FNAC findings and HPE of these thyroid swellings.
Inclusion Criteria
All patients, irrespective of age and sex, who presented with thyroid swellings to the Department of ENT and underwent fine-needle aspiration studies and surgery (hemithyroidectomy/total thyroidectomy) by the three senior authors in our institute, were included.
Sample Collection and Method
All demographic data, FNAC reports and final HPE reports were obtained retrospectively from our Medical Records Department after obtaining ethical clearance. All patients underwent detailed clinical examination, including palpation of the neck. Whenever the disease was difficult to palpate or in clinically cystic lesions, an ultrasound-guided FNAC was done. Patients with Bethesda categories I, II and III were given the choice of periodic follow-up. For Bethesda IV, patients were given the option of hemithyroidectomy and HPE; those patients who were not willing to follow up or were unwilling to undergo hemithyroidectomy underwent total thyroidectomy. Patients with Bethesda V and VI underwent total thyroidectomy. The FNAC diagnosis was compared with the final HPE diagnosis, and statistical data were compiled for correlation.
Statistical Analysis
Statistical analysis was performed using SPSS (IBM, 28.0) in consultation with a statistician. Descriptive statistics were presented as frequency (percentage). Diagnostic accuracy, including sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV), was calculated between FNAC and HPE. κ-Statistics was also performed to determine the agreement between FNAC and HPE. P < .05 was considered statistically significant.
Results
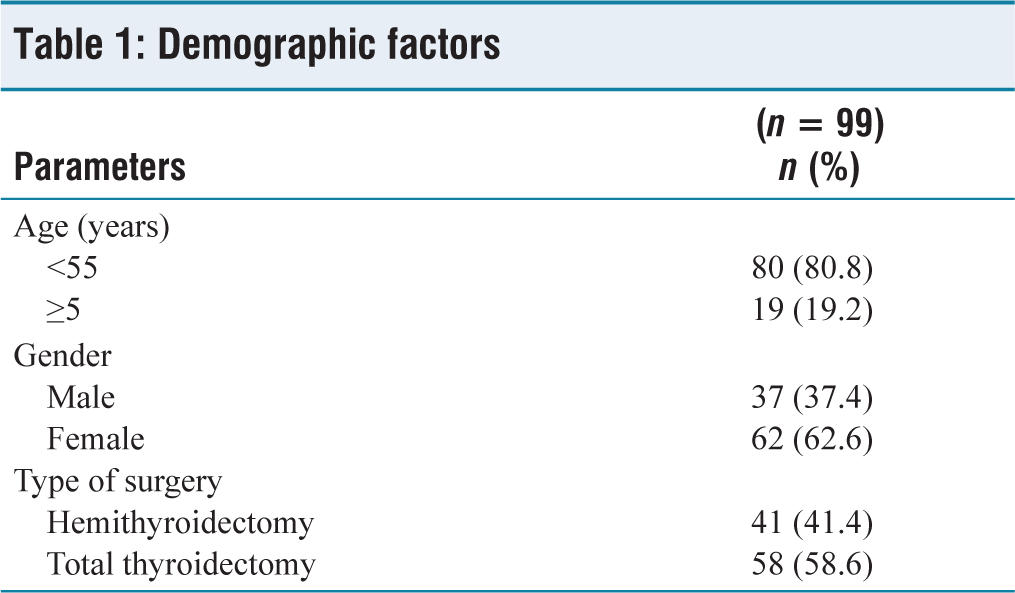
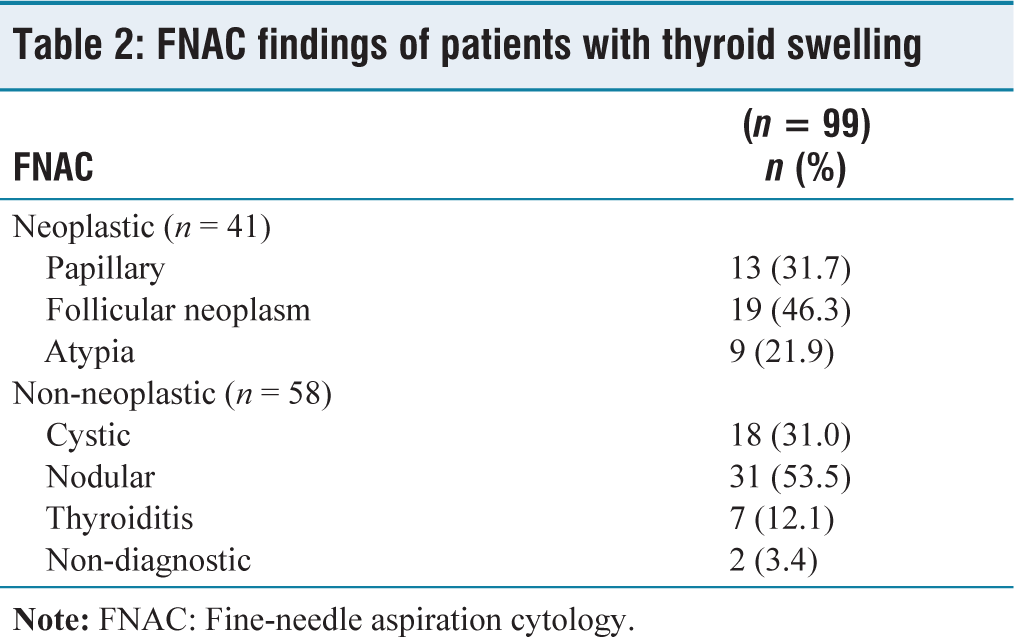
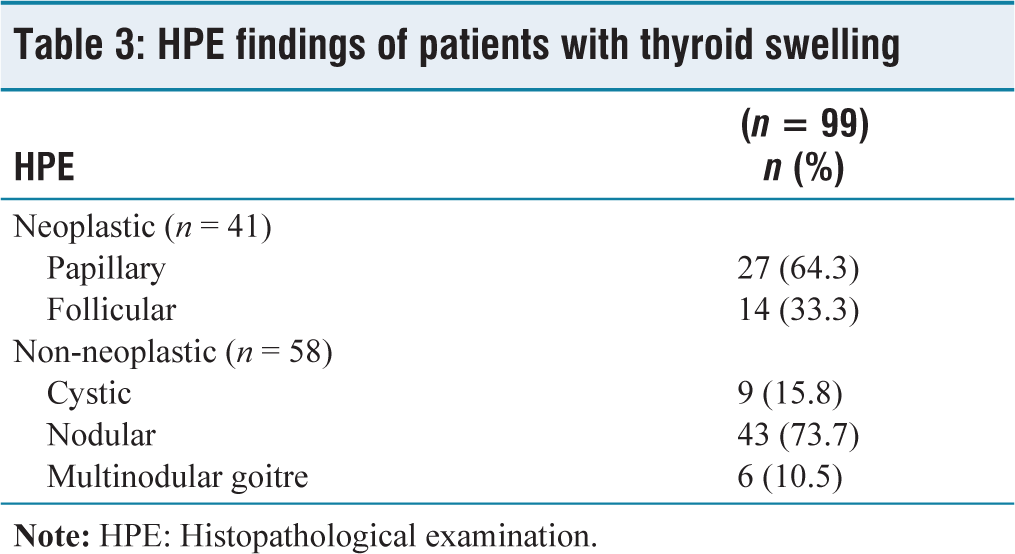
In this group of 99 patients, the majority were under 55 years of age, 62 (62.6%) were females and 58 (58.6%) patients underwent total thyroidectomy [Table 1]. As demonstrated in Tables 2 and 3, majority of the thyroid swellings were non-neoplastic in nature. From Table 4, it was found that the FNAC demonstrated a sensitivity of 73.2% (95% confidence interval (CI): 57.1%–85.8%) and a specificity of 81% (95% CI: 68.6%–90.1%). The PPV was 73.2% (95% CI: 60.8%–82.7%), while the NPV was 81% (95% CI: 71.7%–87.8%). Overall, the accuracy of the test was 77.8% (95% CI: 68.3%–85.5%).
Demographic factors
FNAC findings of patients with thyroid swelling
HPE findings of patients with thyroid swelling
Correlation between FNAC and HPE findings
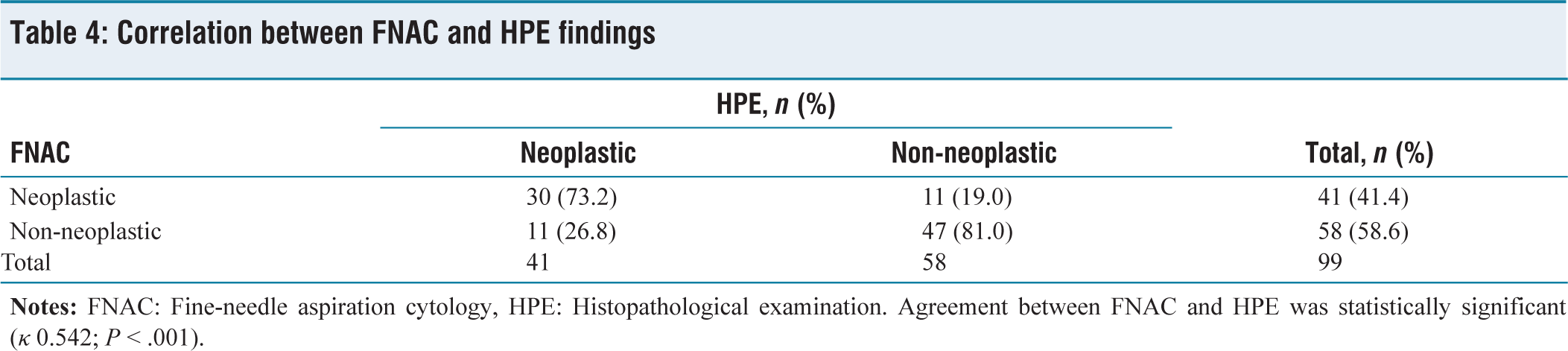
For 11 patients who underwent FNAC, the results were revised from neoplastic to non-neoplastic after HPE [Table 4]. Of these, six patients initially diagnosed with follicular neoplasm on FNAC were found to have a nodular goitre on HPE, while four patients’ diagnoses were downgraded from atypia to nodular goitre and one from atypia to cystic goitre.
In 11 patients, the FNAC results were upgraded from non-neoplastic to neoplastic on histopathology [Table 4]. Of these 11 patients, 4 initially diagnosed with nodular goitre on FNAC were found to have papillary carcinoma, 3 with nodular goitre were diagnosed with follicular carcinoma, 3 with cystic goitre turned out to be papillary carcinoma and 1 case initially classified as ‘non-diagnostic’ on FNAC was also proven to be papillary carcinoma.
As indicated in Table 5, of the 41 cases with neoplastic changes identified on FNAC, only 30 were ultimately confirmed as neoplastic, while the remaining 11 were determined to be non-neoplastic. The following findings were noted: All 13 patients initially diagnosed with papillary carcinoma via FNAC were confirmed to have papillary carcinoma in the final histopathology report. Of the 19 patients diagnosed with neoplasm on FNAC, 13 were confirmed as neoplastic (2 with papillary carcinoma and 11 with follicular carcinoma), while 6 were reclassified as non-neoplastic lesions in the histopathology report. Among the 9 patients with atypia detected by FNAC, 4 were diagnosed with papillary carcinoma, and 5 were found to have non-neoplastic lesions in the final histopathology report.
HPE findings of patients with neoplastic changes on FNAC
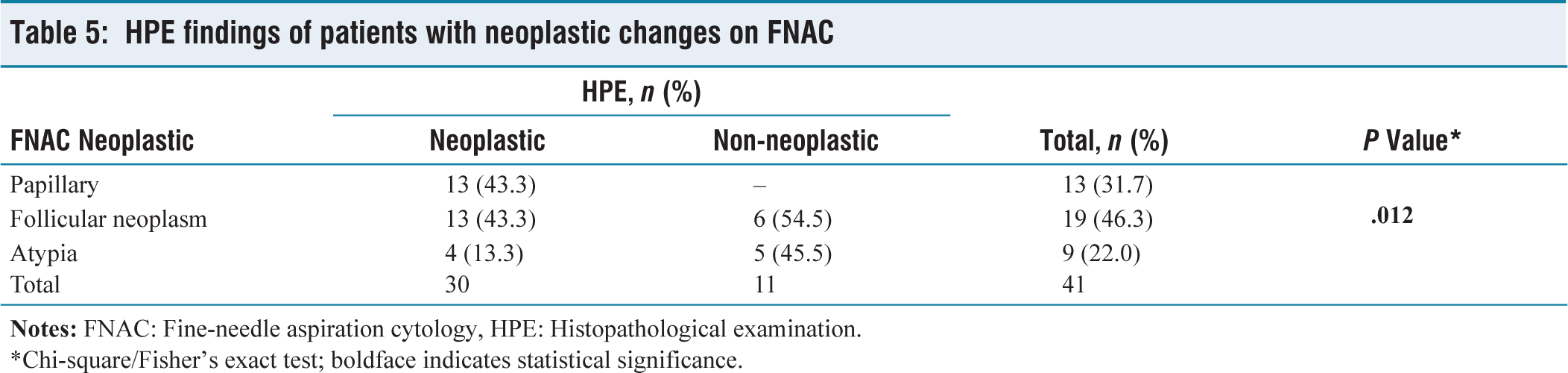
*Chi-square/Fisher’s exact test; boldface indicates statistical significance.
As shown in Table 6, among the 58 cases that exhibited non-neoplastic changes on FNAC, 11 patients’ results proved to be neoplastic, and the following diagnoses were observed:
Of the 18 patients initially diagnosed with cystic goitre via FNAC, 15 were confirmed to have cystic or nodular goitre, while 3 were ultimately diagnosed with papillary carcinoma in the final histopathology report. Of the 31 patients diagnosed with nodular goitre by FNAC, 24 were found to be non-neoplastic (including 1 cystic, 22 remaining nodular and 1 with multinodular goitre). The remaining 7 cases were reclassified as neoplastic (4 with papillary carcinoma and 3 with follicular carcinoma) in the final histopathology report. Additionally, of the seven patients diagnosed with thyroiditis by FNAC, all were confirmed as thyroiditis in the final histopathology report. However, among the two cases classified as ‘non-diagnostic’ by FNAC, one was ultimately diagnosed with nodular goitre and the other with papillary carcinoma based on the final histopathology report.
HPE findings of patients with non-neoplastic changes on FNAC
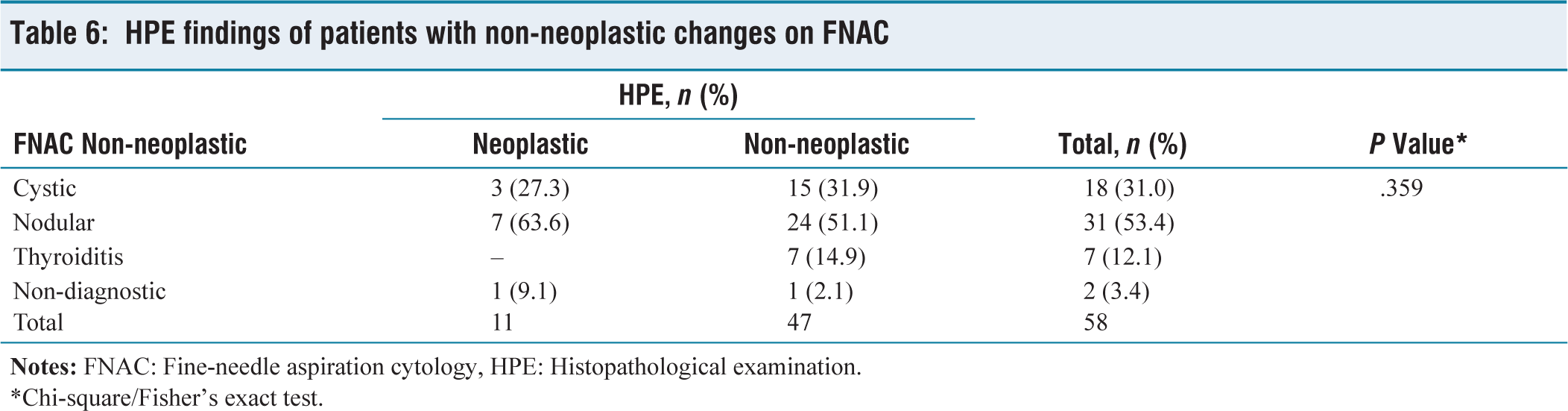
*Chi-square/Fisher’s exact test.
Discussion
While the overall agreement between FNAC and final HPE was statistically significant (P < .001), the P value for FNAC of non-neoplastic lesions compared to the final HPE was not statistically significant (P < .359). This suggests that FNAC, while a useful diagnostic tool, may not always provide a definitive diagnosis. FNAC serves as a valuable diagnostic tool, but it should be supplemented with clinical examination and neck imaging (such as ultrasound or CT scan) to improve diagnostic accuracy and aid in surgical decisions, especially when the FNAC report is non-neoplastic.
In developing countries like India, where guidelines may be challenging to implement in rural or outreach areas, relying solely on FNAC might lead to over-treatment or under-treatment. Our study noted cases where neoplastic findings in FNAC were downgraded to non-neoplastic in the final HPE. Performing total thyroidectomies in such instances, especially without other compressive symptoms, might result in unnecessary postoperative complications such as hypocalcaemia, voice changes and poor quality of life. A confounding factor in this study is that different pathologists with varying levels of experience performed FNAC and HPE. Additionally, expanding the study to include a larger group may lead to different results.
Conclusion
FNAC is a straightforward evaluation tool with limitations in thyroid swelling. It is most effective when used in conjunction with clinical examination and other diagnostic investigations.
Footnotes
Acknowledgements
We thank Dr Shivashankari (Research Assistant) and Logesh (Biostatistician) from the Research Department, Apollo Hospital Chennai.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
The study was approved by Institutional Ethics Committee – Bio Medical research, Apollo Hospitals, Chennai, and the IEC number is AMH-C-S-079/ 08-24.
Informed consent
Not applicable.
Credit author statement
K.R.S.: Data collection, literature review, investigation, data analysis, writing—original draft preparation.
A.A.: Literature review, writing—original draft preparation.
S.K.: Conceptualisation, investigation, supervision, data analysis, writing—review and editing.
N.N. and P.S.R.: Conceptualisation, investigation, supervision, validation, writing—review and editing.
All authors: Reviewed and approved the final manuscript.
Data availability
Data presenting the study’s findings are available from the corresponding author.
Use of artificial intelligence
Not applicable.