
Abstract
Introduction:
The interface between tuberculosis (TB) and HIV is increased in countries like India where both TB and HIV infection are maximally prevalent. Worldwide, TB is the second leading infectious killer after COVID-19. Ten percent of persons infected by both TB and HIV develop TB disease annually and in one-third of them, it turns out to be fatal. HIV- tuberculosis co-infection has an atypical presentation which mostly depends on the degree of immunosuppression.
Aims and Objectives:
To study the socio-demographic profile, clinical manifestations, and radiological presentation with relation to the CD4 count of patients co-infected with pulmonary TB and HIV.
Methodology:
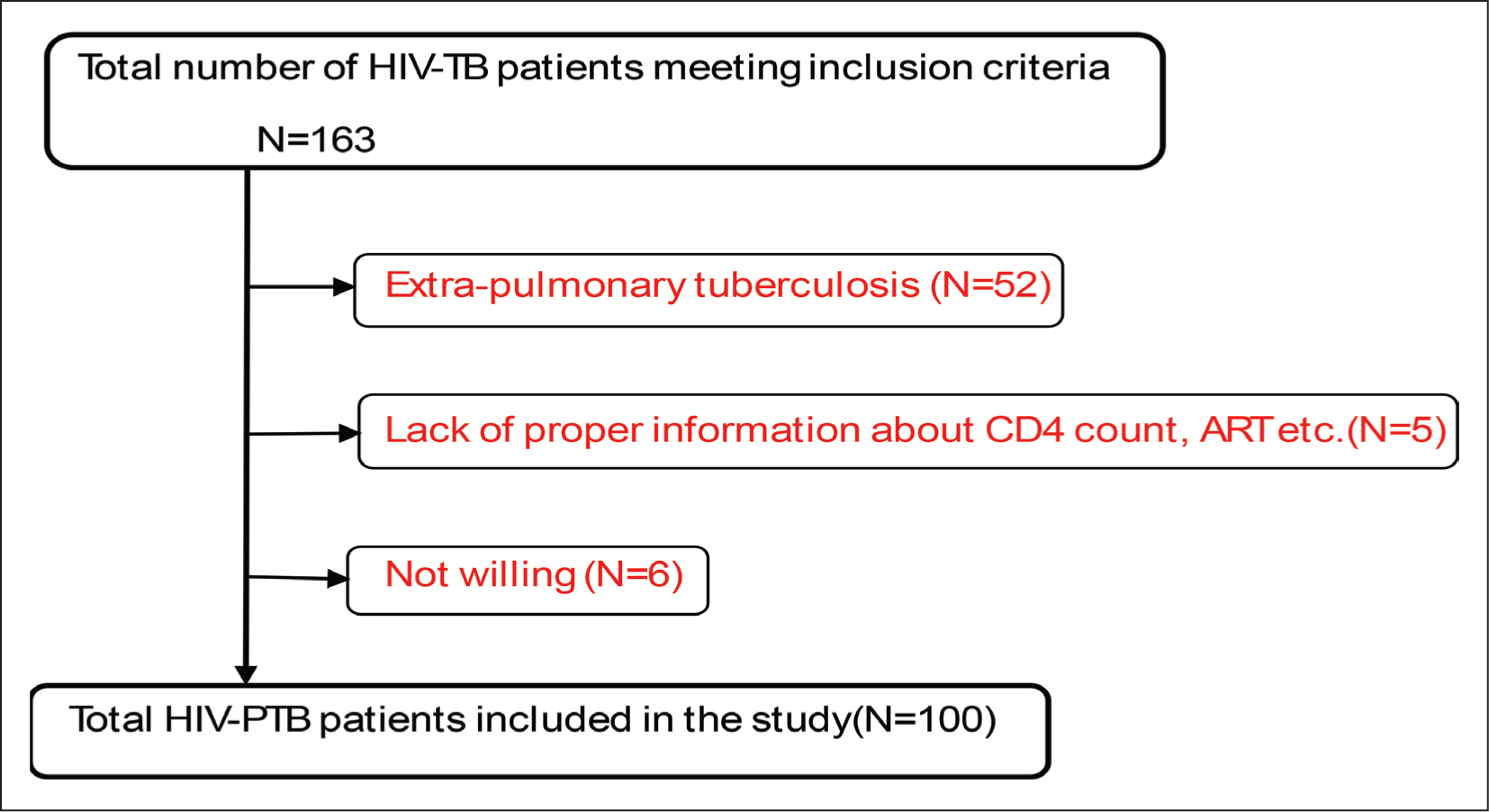
This is a hospital-based observational, cross-sectional study done in 100 HIV-PTB co-infected patients from Nov’2021 to Nov’2023. The study was carried out after getting Institutional ethics clearance and Informed written consent from the participants.
Results:
The majority (74%) were males with 75% belonging to 31–50 years of age. Fifty-eight percent had a CD4 count between 50 and 200 cells/mm 3 . Fever (90%) was the most common presenting symptom followed by cough (85%). Atypical features of TB were present in 52% of the patients.
Conclusion:
CBNAAT must be indicated as a primary diagnostic modality for detecting TB in PLHIV. Atypical presentations of TB on Chest X-rays are common which are attributed to low CD4 count (≤200) in the present study. Awareness regarding HIV/AIDS, safe sex practices and cough etiquette is the need of the hour.
Introduction
The world’s highest concentration of tuberculosis (TB) cases is found in India. India is home to around 14 million cases of TB, of which 1.8 million incident cases—of which 0.82 million are highly contagious smear-positive cases—occur here annually.[1] HIV and TB have a synergistic interaction. In nations like India, where HIV infection and TB are most common in individuals between the ages of 15 and 49, there is a greater interaction between the two infections.[2] In nations with limited resources, the link between HIV and TB poses an urgent and serious danger to public health and socioeconomic conditions.[3]
HIV-negative individuals with a TB infection have a yearly probability of <0.5% for acquiring an overt disease,[4] whereas 10% of those with an HIV infection develop TB disease.[5] When it comes to opportunistic infections, TB is actually the most prevalent one among patients from underdeveloped nations who passed away from AIDS.[6] According to reports, over one-third of HIV-positive individuals die from TB, and active TB enhances the morbidity and mortality of the disease.[5] Compared to those without HIV, those living with HIV had a 16 (uncertainty interval 14–18) times higher risk of developing TB illness. For those living with HIV, TB is the main cause of death.
Worldwide, TB is the second most common infectious killer after COVID-19 (above HIV and AIDS).[7] 7.5 million people were newly diagnosed with TB in 2022 with India accounting for about 27% of cases. TB caused an estimated 1.30 million deaths (95% UI: 1.18–1.43 million). According to WHO, India is the nation with the highest rates of TB, HIV-associated TB, and multidrug-resistant tuberculosis (MDR/RR-TB) between 2021 and 2025, in the world.[7] HIV-associated tuberculosis has atypical presentation which mostly depends on the intensity of immunosuppression.[7]
The areas and demographic categories with the highest HIV prevalence have also had the largest increase in TB cases, indicating that the HIV epidemic is at least partially accountable for the rise in TB cases.[8] There is evidence that TB and other infections induce cytokines that enhance the replication of HIV and this drives the patient into a full picture of AIDS.[9] The atypical presentation and increased association of TB and HIV warrants a profile of such patients.
Aims and Objectives
To study the socio-demographic profile, clinical manifestations and radiological presentation with relation to CD4 count of patients co-infected with pulmonary TB and HIV.
Methodology
This is a hospital-based observational, cross-sectional study done in HIV-PTB co-infected patients attending the Government Hospital for Chest and Communicable Diseases (GHCCD), Visakhapatnam from November 2021 to November 2023. The study was carried out after getting Institutional ethics clearance and Informed written consent from the participants. Sample size calculation for the current study was done with the following formula:
Sample Size (n) = (Z1-α/2) 2 × p (1 – p) / e 2
Assuming, Z1-α/2 = 1.96 (for 95% confidence interval),
p = 0.50 (Prevalence), e = 0.10 (margin of error)
The minimum required sample size will be 96 which was rounded off to 100.
Inclusion criteria:
HIV-positive cases who were diagnosed to have TB already and are using ATT. HIV-positive cases (+/- ART) that are recently detected with active TB and started on ATT. PTB patients using ATT and found to be HIV-positive on screening.
Exclusion criteria:
HIV-positive cases who were previously treated for PTB and presently not using ATT. Active PTB patients using ATT but HIV-positive patients with only extra-pulmonary TB (including Pleural TB) but no pulmonary TB. Patients <18 years old.
All the data was entered in Microsoft Office Excel and analysed using the same. Comparison between CXR features and CD4 count was done using chi-square test in Graph pad prism software.
Results
Out of the 100 HIV-PTB co-infected patients studied 74% (N = 74) were male and 26% (N = 26) were female.
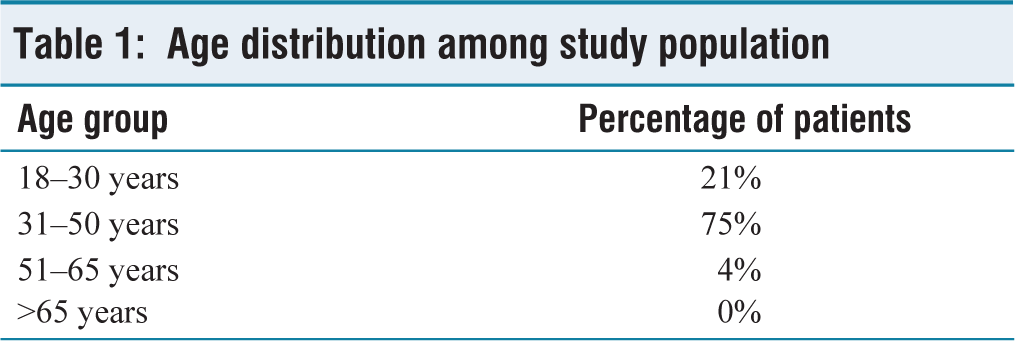
As seen in Table 1, 21% of patients were in the age group of 18–30 years, 75% patients fell in the group of 31–50 years of age, only 4% patients were in the age group of 51–65 years and none was above 65 years. The mean age of the patients was 36.55 years.
Age distribution among study population
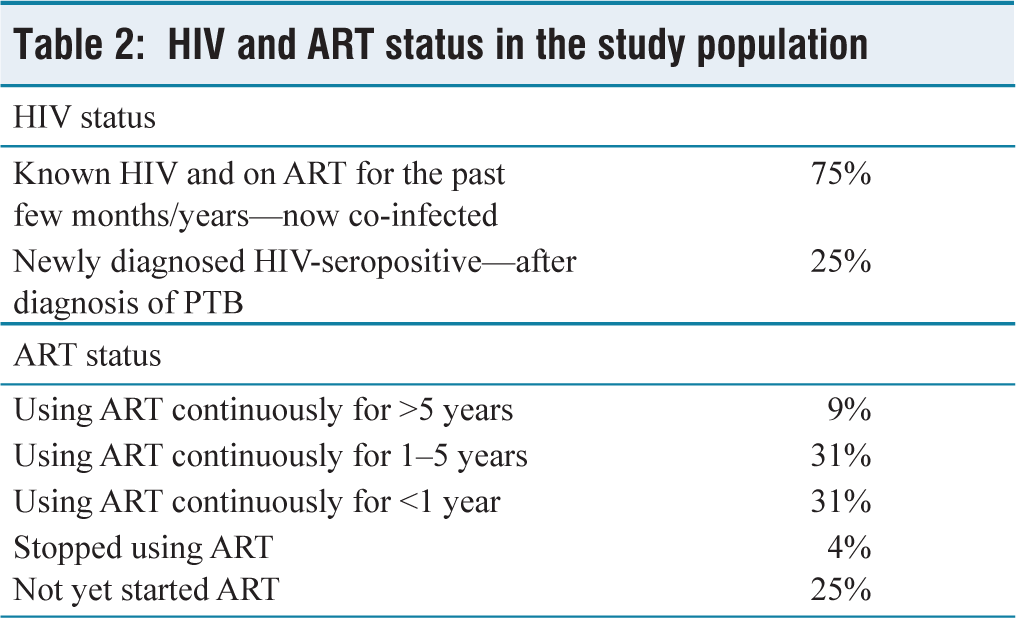
Most of the patients were known HIV seropositive cases using ART for few years. It is observed from Table 2 that 75% of the co-infected patients in the present study are using ART of whom 9% have been using it for more than 5 years, 31% for 1–5 years and 31% for less than one year while 4% have discontinued ART (stopped using ART) due to different reasons. Twenty-five percent of the co-infected patients are diagnosed as HIV seropositive recently during routine screening done after the diagnosis of pulmonary TB and they have not yet started ART.
HIV and ART status in the study population
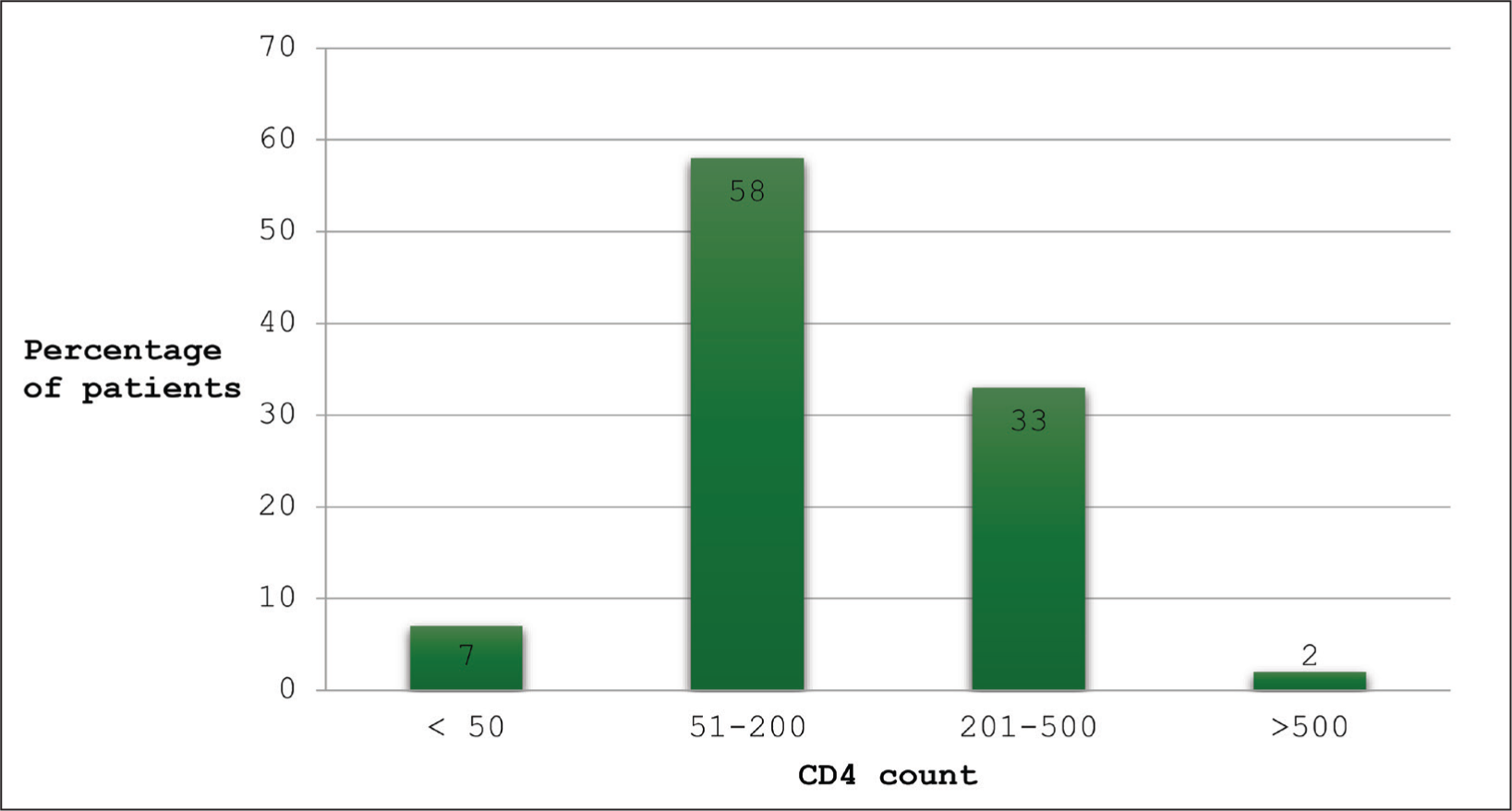
As evident from Figure 1, 7% of the patients had CD4 count <50 cells/mm3, 58% had CD4 count in between 50 and 200 cells/mm3, 33% had CD4 count 201–500 cells/mm3 and only 4% had CD4 count above 500 cells/mm3.
Distribution of CD4 count in HIV-TB study population
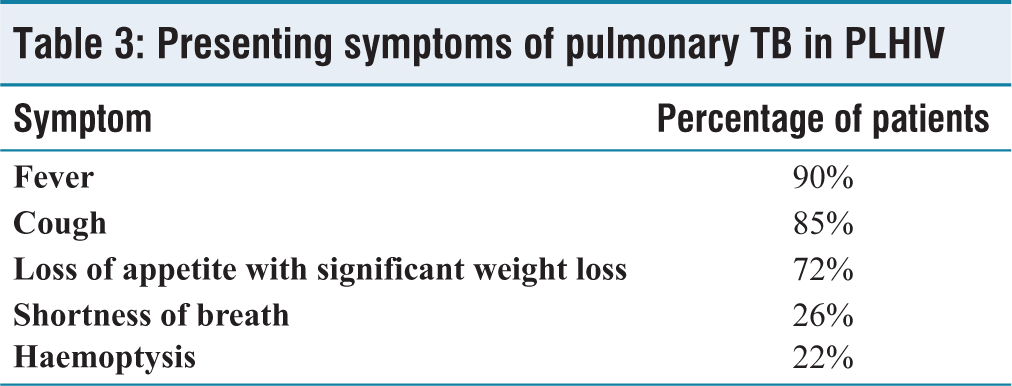
It is evident from Table 3, that 90% of the patients complained of fever making it the most common presenting symptom of pulmonary TB in people living with HIV/AIDS. The next common symptoms were cough (85%), loss of appetite with loss of weight (72%), shortness of breath (26%) and haemoptysis (21%).
Presenting symptoms of pulmonary TB in PLHIV
Out of 100 patients, 79% of patients were microbiologically diagnosed whereas 21% of patients were clinically diagnosed.
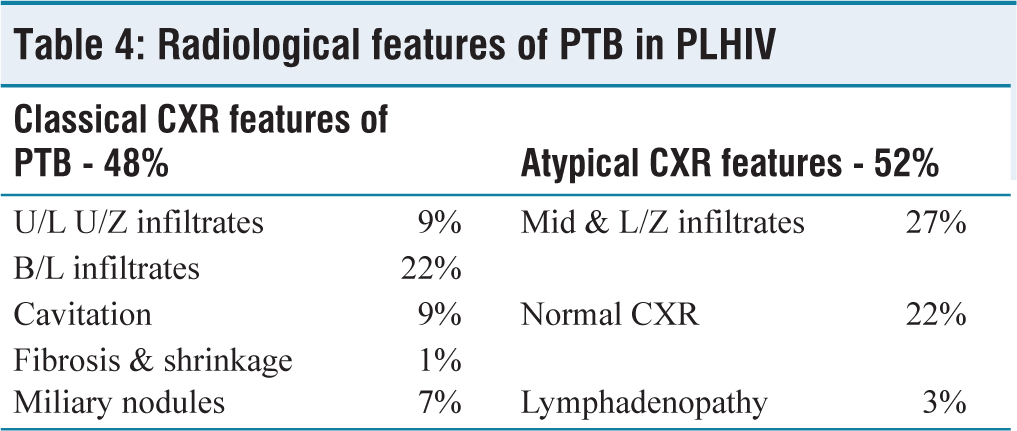
Classical features of pulmonary TB were present in 48% of patients whereas, 52% of patients had atypical radiological features of TB in the form of mid/lower zone infiltrates (27%), mediastinal/hilar lymphadenopathy (3%) and normal chest radiograph (22%) as evident from Table 4.
Multidrug-resistant pulmonary TB was present in 7% of the cases. Of the remaining cases, 28% were previously treated pulmonary TB cases while 63% were new pulmonary TB cases.
Radiological features of PTB in PLHIV
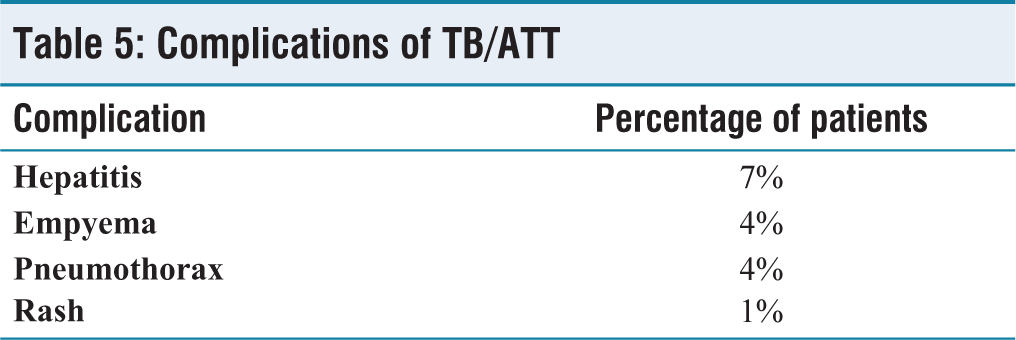
Of the 16% patients who presented with complications of TB/ATT, majority of patients presented with drug-induced hepatitis (7%), 4% with tubercular empyema, 4% with pneumothorax and 1% with ATT-induced skin rash as evidenced from Table 5.
Complications of TB/ATT
Discussion
Most of the patients, that is, 74% of HIV-PTB co-infection are male, while females are only 26%. The male preponderance noted in the current study was similar to that of other studies as mentioned in Figure 2. In a study by Patel et al.,[10] Praveen Kumar et al.,[11] Purushottam et al.[12] 82%, 90.5%, and 58% of the patients were male, respectively, and 18%, 9.5%, and 42% were females, respectively. This male predominance observed in the studies may be attributed to high sexual promiscuity in males which leads to increased HIV in males and so HIV-TB co-infection. The reason may also be less health care sought by female patients due to the stigma attached with these diseases.
Enrolment of patients in the study
The age-wise distribution observed in the present study was similar to that noted in previous studies. In the study by Patel et al.,[10] 34% are below 30 years of age, 64% are in the age group of 31–50 years and only 2% are above 50 years of age. In a study by Christopher et al.[13] in Nigeria 32% of the patients were below 30 years age, 56% were in the age group of 31–50, 8% were 51–65 years and 4% above 65 years. This age group of 31–50 years is the prime age for actively working and earning in a person’s life. So, diseases in this age will hamper a person’s career and financial progress and in turn, effect that person’s and his/her family’s economic status permanently, thus affecting the nation’s economy as well.
In the study by Christopher et al.,[13] the mean CD4 count of HIV-TB co-infected patients was 150 while that of non-TB HIV patients was 276. Mean CD4 count in present study was 183.62 whereas, in studies by Agarwal et al.,[14] it was 108.2. HIV-positive individuals with low CD4 cell counts have significantly reduced immunity, which leaves them vulnerable to new TB infections or the reactivation of latent infections and a rapid deterioration of their clinical state. It is already known that TB increases the viral load in the HIV-positive population six to seven times.[15] While it is more common at CD4 counts <300 cells/μl, TB is unique in that it can occur at a wide range of CD4 counts, unlike toxoplasmosis or cryptococcal meningitis, which occur at very low numbers.
As observed in Table 3, fever was the most common symptom of pulmonary TB present in 90% of the patients in the present study, followed by cough, loss of appetite with weight loss, shortness of breath and haemoptysis present in 85%, 72%, 55%, 26% and 22% of the patients respectively. Cough, fever, weight loss, loss of appetite, dyspnoea and haemoptysis were present in 94%, 86%, 78%, 56%, 14% in Patel et al., study[10] whereas 83.9%, 85.7%, 96.4%, 25% in the study by Christopher et al.,[14] respectively. In the study by Praveen Kumar et al.[11] cough was the most common symptom, which was observed in 97.6% patients followed by fever in 90.4%, anorexia with weight loss in 78.6% and haemoptysis in 31% of patients. It was observed from all the studies that fever, cough, loss of appetite with loss of weight are the main presenting symptoms of TB in PLHIV.
In the study by Praveen Kumar et al.,[11] upper zone infiltrative lesions were observed in 12.5% of patients, bilateral diffuse infiltrative lesions in 21.7%, mid/lower zone infiltrates in 19.2%, cavitations, intrathoracic lymphadenopathy and other atypical features were found in rest of the patients. In the study by Christopher et al.[14] most of the patients (81.8%) had Atypical chest X-ray features. In a comparative study of radiologic findings of pulmonary TB among HIV-seropositive and HIV-seronegative by Ahmadi F et al.[16] 32.35% HIV-PTB had a normal chest X-ray without any radiological pulmonary signs suggestive of TB. 23.52% had pulmonary infiltrates and only 8.82% had cavitary lesions while in PTB patients without HIV, 58.23% had pulmonary infiltrates and 34.11% had cavitary lesions. It is observed from all the above studies that atypical CXR features are very common in PLHIV.
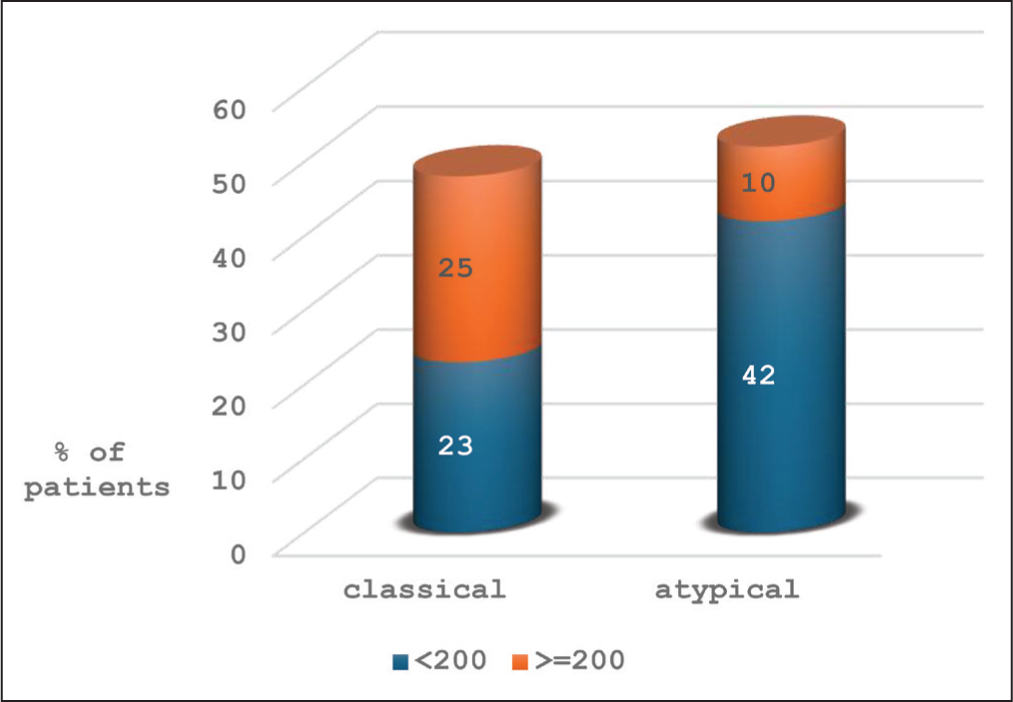
In HIV-PTB co-infected patients with Atypical CXR features of pulmonary TB, the percentage of patients with CD4 count <200 (42%) (p = .0006) was significantly higher when compared to percentage of patients with CD4 count >=200 (10%) as evident from Figure 3. This may be explained by poor cell-mediated immunity resulting in reduced granuloma formation, caseation, liquefaction and cavitation.
Comparison of CXR features with CD4 count
A similar observation was made by Tripathy et al.[17] where patients with higher CD4 counts showed more cavity formation and such cavity formation was commonly observed in patients with intact cell mediated immunity. Higher incidence of mid and lower-zone involvement may also be attributed to poor cell-mediated immunity in PLHIV.
New TB cases were 63% of the total HIV-PTB cases which might be due to, HIV infection increasing the risk of progression of TB infection to active disease. Multidrug-resistant pulmonary TB was present in 7% of the cases of HIV-PTB co-infected cases in the present study. Drug malabsorption in HIV-infected patients has been shown to lead to treatment failure and drug resistance.[18]
MDR-TB cases account for 3% of the New TB cases and 12%–17% of retreatment cases. A consistent finding has been observed on risk factors for multi-drug resistance TB in Europe by Faustini et al.[19] that MDR-TB patients were more likely to be HIV-positive. In a study by Deivanayagam et al.[20] in Chennai, the prevalence of HIV in MDR-TB patients was 4.42%. In a study conducted in an ART centre in Mumbai by Petro et al.,[21] alarming levels of drug-resistant TB of 34% were observed in HIV-co-infected patients. The above study included pulmonary and extra-pulmonary TB among HIV patients, whereas present study included only pulmonary TB patients and in the present study 7% of the HIV-PTB co-infected patients had MDR-TB (pulmonary tuberculosis).
Conclusion
HIV-PTB co-infection affects the nation’s economy adversely as most of the patients are in the working age group. CBNAAT must be indicated as a primary diagnostic modality for detecting TB in PLHIV. Atypical presentations on chest X-rays are common in HIV-TB co-infected patients which are attributed to low CD4 count (<= 200) in the present study. Awareness regarding HIV, safe sex practices and cough etiquette is the need of the hour.
Limitations of the study
Drug resistance profile of TB was not studied in detail.
Patients were examined only when they attended hospital, but were not followed till completion of ATT. So, outcome of treatment of TB could not be studied.
Drug-drug interactions (ART-ATT) were not studied.
As it is a hospital-based study, community profile could not be studied.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional Ethical Committee Approval Number
REG.NO.1/IEC/AMC/2018
Informed consent
Informed consent was taken from all the participants.
Credit author statement
Shanthi Annapurna: Conceptualisation, methodology, investigation and writing.
Shalini Perumal: Data curation, writing and visualization.
Sunil Kumar Raghumanda: Supervision and project administration.
Praveena Sreerama: Validation and supervision.
Data availability
Non digital data curated at AMC.
Use of artificial intelligence
Nil.