
Abstract
This study is to analyze clinical features of 97 AIDS patients received and treated in our hospital. Clinical data of 97 HIV-infected patients who were admitted between September 2004 and September 2018 were analyzed retrospectively. We found that all patients were in AIDS stage, CD4+ T lymphocytes counts were (210.56 ± 79.31)/µL. After the highly active antiretroviral therapy (HAART) regimens, CD4+ cell number is 315.21 ± 187.90, most patients before clinical symptoms are significantly improved. HIV infections were mainly through intravenous drug injection (51 cases, 52.58%) and sex contact (29 cases, 29.90%). In conclusion, the clinical manifestations of AIDS patients are various, and the main infection route is intravenous drug injection. Multiple measures should be taken to prevent and control HIV transmission, patients should undergo effective antiviral treatment, monitor and follow-up, so as to control opportunistic infection and virus replication.
Keywords
Introduction
AIDS is also called acquired immunodeficiency syndrome, which is a severe, fatal, and acquired infectious disease caused by HIV (Human Immunodeficiency Virus). It is spread through sexual contact and body fluid. A series of clinical syndromes appear due to the damage to body immunity function. 1 The first HIV-infected person was found in Xinjiang in 1995, and now fast growth stage of morbidity comes. The author analyzed clinical data of 97 AIDS patients received and treated in our hospital from September 2004 to September 2018.
Objects and methods
Ethical approval
The study was approved by the Institutional Ethics Committee of our hospitals, and written informed consent was obtained from all participants.
Objects of study
Infection Department in the First Affiliated Hospital of Xinjiang Medical University received and treated 97 AIDS/HIV patients from September 2004 to September 2018. Disease Control and Prevention Center of Xinjiang Uygur Autonomous Region (Xinjiang HIV/AIDS Monitoring Center Centers for Disease Control and Prevention (CDC)) applied Western Blot (WB) method to confirm HIV antibody of all cases was positive. They were explicitly diagnosed with AIDS patients, including 64 male patients and 33 female patients. Among them, 25 patients were below 30 years old; 71 patients were 30–60 years old; and 1 patient was above 60 years old, with the average age of 32.92 ± 6.21. HIV infection routes are as follows: 51 patients had drug addiction history (52.58%); 29 patients had promiscuity history (29.90%); 7 patients had blood transfusion history (7.22%); the route of infection was unknown for 9 patients (9.28%); and 2 patients had both promiscuity history and drug addiction history (2.06%).
Diagnostic basis
A definite diagnosis was made for all cases in accordance with State Standard of the People’s Republic of China HIV/AIDS Diagnostic Criteria and Handling Principles as well as patients’ epidemic history, clinical manifestations, HIV antibody serological test results (WB test), and T lymphocyte subpopulation test. 2 WB test was conducted at Center for AIDS/STD (sexually transmitted disease) Control and Prevention, and Disease Control and Prevention Center of Xinjiang Uygur Autonomous Region. A total of 97 patients conformed to AIDS diagnostic criteria. T lymphocyte subpopulation test was carried out by Coulter EPICS (R) XL analyzer flow cytometry at clinical laboratory center of our hospital.
Therapeutic schedule
HAART scheme
According to the recommended scheme of AIDS antiretroviral therapy, 3 highly active antiretroviral therapy (HAART) scheme involved two kinds of nucleoside reverse transcriptase inhibitors (NRTIs) and one kind of non-nucleoside reverse transcriptase inhibitors (NNRTIs). In combination of drugs available in our region, there were two kinds of drug combinations: zidovudine (AZT) + lamivudine (3TC) + nevirapine (NVP) or Stavudine (D4 T) + 3TC + NVP. The drugs were provided by the state for free. CD4+ T lymphocyte count < 200/μL. Those comforting to the conditions received antiviral therapy.
Statistical analysis
SPSS23.0 statistical software was used for analysis. The t-test was applied for mean comparison, and the test value was expressed as mean ± standard deviation. X2 test was adopted for rate comparison. P > 0.05 means the difference has no statistical significance, or else the difference has statistical significance. Inspection level α = 0.05.
Results
General information of HIV/AIDS patients
A total of 97 patients had complete clinical case data. The proportion of cases of HIV/AIDS patients in all ages and the path of HIV infection are shown in Table 1.
General information of HIV/AIDS patients.

In the infection routes of AIDS patients, sexuality accounts for 34% and intravenous drug use accounts for 50%. The patients are mainly young adults with the age of 30–60. This indicates among the young adult patients, sexuality and intravenous drug use are main routes of HIV infection for HIV/AIDS patients.4,5
Clinical analysis
Clinical manifestations
Clinical manifestations of 97 AIDS patients mainly include fever, hypodynamia, night sweat, and so on; the same was true after treatment with HAART.
T lymphocyte subset test
Among five AIDS patients, CD4+ T lymphocyte count before treatment is shown in Table 2. For most AIDS patients, CD4+ T lymphocyte count > 200/μL.
The probability of different levels of CD4+ cell count combined with tuberculosis infection and the proportion of CD4+ cell count in the control group.

The CD4+ T lymphocyte count of most AIDS patients with tuberculosis was less than 200/μL, totaling 86 cases (88.66%), while the CD4+ T lymphocyte count of most non-tuberculosis patients was more than 200/μL and less than 200/μL in 39 cases (40.21%), which indicated that the probability of different levels of CD4+ T lymphocyte count combined with tuberculosis infection was different. There is a very close relationship between the two, that is, when the CD4+ T lymphocyte count is less than 200/μL, tuberculosis infection is more likely to occur.
Treatment
HAART treatment was carried out for 46 HIV/AIDS patients alive, of whom 44 patients were alive, and 2 patients died. The change of total number of CD4+ T lymphocytes after treatment are shown in Table 3.
Changes of total number of CD4+ T lymphocytes before and after treatment.
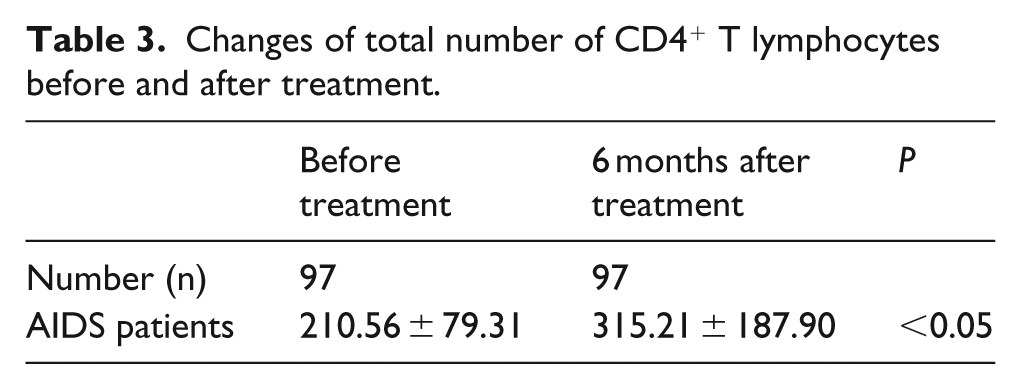
The comparison of the number of CD4+ T lymphocytes of AIDS patients before HAART treatment and after treatment for 6 months had statistical difference (P < 0.05). The number of CD4+ T lymphocytes significantly rose after treatment for 6 months. 6 During the follow-up visit of 44 AIDS patients, clinical symptoms of some patients such as hypodynamia, night sweat, and chest distress disappeared completely, and clinical symptoms of most patients improved obviously. This indicates the effect of antiviral therapy is significant.
Discussions
Sexual activity and intravenous drug use are the main ways for HIV/AIDS patients to acquire HIV infection. A total of 51 cases (52.58%) have history of drug use; 29 cases (29.90%) have history of sexual disorder, 64 cases (65.98%) are male; 71 cases (73.20%) are young and middle-aged; and 71 cases (73.20%) are 30–60 years old. Various measures should be taken to prevent and control the spread of HIV, strengthen anti-virus treatment and monitoring, follow-up, timely control of opportunistic infections and virus replication. The CD4+ T lymphocyte count of most AIDS patients with tuberculosis was less than 200/μL, a total of 86 cases (88.66%), while the CD4+ T lymphocyte count of most non-tuberculosis patients was more than 200/μL and less than 200/μL in 39 cases (40.21%). AIDS was susceptible to tuberculosis infection. The risk of tuberculosis in HIV and tuberculosis co-infected patients was significantly higher than that in tuberculosis-infected patients alone. HIV tuberculosis double infection will produce serious consequences of “1+1>2.” 7 Once infected with tuberculosis, HIV-infected people will greatly shorten the incubation period of the onset, rapidly develop AIDS, and rapidly deteriorate to death. 8 Some studies have shown that the main cause of AIDS complicated with tuberculosis infection is the deficiency of human immune function, which leads to the resurgence of tuberculosis bacteria in the dormant state of the body lesions or the formation of new lesions by the re-infection of tuberculosis bacteria. It can also rapidly develop into tuberculosis through initial infection. At the same time, tuberculosis also has a negative impact on HIV infection. Tumor necrosis factor (TNF) is produced by activated macrophages in granulation after tuberculosis infection, which can activate and promote the proliferation of HIV in CD4+T cells and promote the development of the disease. 9 The lower the level of CD4+T cells, the lower the immune level, the higher the probability of opportunistic infection, and the higher the mortality rate. Therefore, CD4+T cell count is used as an important parameter to detect the progress of AIDS and monitor the occurrence of opportunistic infection and mortality. Tuberculosis infection was more likely to occur when CD4+ T lymphocyte count was less than 200/μL. There was significant difference in CD4+ T lymphocyte count between the two groups (P < 0.05). Tuberculosis is the main cause of AIDS opportunistic infection and death, and the number and dysfunction of CD4+ cells may be the main cause. 10 The CD4+ T lymphocyte counts of AIDS patients with tuberculosis were compared before and 6 months after treatment with anti-tuberculosis therapy and HAART (P < 0.05). CD4+ T lymphocyte count increased significantly after 6 months of treatment compared with that before treatment. Therefore, CD4+ T lymphocyte count as a reference index for the prevention of opportunistic infections is of great significance to improve the quality of life of AIDS patients. Relevant studies have confirmed that anti-tuberculosis and antiviral treatment for AIDS patients with tuberculosis can significantly improve the clinical symptoms of patients, and can gradually improve the condition of patients. In this study, CD4+ T lymphocyte counts were compared before and after treatment. However, due to the limited number of cases in this group, how to correctly treat tuberculosis/HIV patients has not yet rich clinical experience, which needs to be further explored. Therefore, timely detection of AIDS patients with tuberculosis and regular treatment has become an important and practical issue in the control of AIDS patients with tuberculosis. The patients with the above two diseases should be treated together, and the treatment of the two diseases should be strengthened.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.