
Abstract
The introduction of antiretroviral therapy (ART) in 1995 had a dramatic impact on the morbidity and mortality of the HIV population, and subsequently, the natural history of cancer has changed. The purpose of our study was to review the prevalence of AIDS-defining malignancies and non-AIDS defining cancers (NADC), taking into consideration racial and gender variations. After the institutional review board approval, the study was conducted as a retrospective chart review of 279 HIV-infected patients who were treated at the Moffitt Cancer Center between January 1, 2000 and December 31, 2010. The demographic characteristics included gender, ethnicity, race, presence or absence of ART, and the type of malignancy reviewed. Of 233 men, 78 (33.5%) had AIDS-defining malignancies. AIDS-related non-Hodgkin lymphoma (NHL) was detected in 49 (21%) patients and Kaposi sarcoma (KS) in 29 (12%) patients. Two-thirds of male patients had NADC, with anal cancer being the most prevalent (8.5%), followed by Hodgkin lymphoma (6%). AIDS-related NHL was also the predominant malignancy for women with a prevalence of 19.5% followed by invasive cervical cancer (ICC) and breast cancer, both with a similar prevalence of 11%. Kaposi sarcoma and anal cancer were equally detected in 2% of women. The prevalence rates of AIDS-defining malignancies among those of white race were 34%, ranging from 21% for NHL to 13% for KS and 1.5% for ICC. Twenty-one (7.7%) patients had anal cancer. AIDS-defining malignancies were found in 36% of patients of black race and 60% had NHL. Non-AIDS-related NHL was the second most common malignancy, followed by breast cancer and anal cancer with a similar prevalence of 6.5%. Of 279 patients, 53% were taking ART; 39.4% were not taking ART; and in 7.5% of the patients, it was unknown if they were taking ART. In the ART era, our study found NADC to be more prevalent than AIDS-defining malignancies with 60% versus 40%, respectively. Non-Hodgkin lymphoma remained the most common AIDS-related malignancy in both genders. Among the patients with NADC, anal cancer was the predominant malignancy. The increasing incidence of some of the NADC is expected as this population is living longer with chronic exposure of viral replication of virus with oncogenic potential such as Human papillomavirus (HPV), Hepatitis B virus (HBV), Epstein-Barr virus (EBV), and Human herpesvirus 8 (HHV-8). Early ART initiation, aggressive vaccination, and judicious cancer screening are the cornerstone of cancer prevention of this growing population.
Keywords
Introduction
HIV infection is well known to be associated with numerous malignancies. The burden of this relationship was more prominent in the era of pre-highly active antiretroviral therapy (HAART). 1 In the 1980s, it had been suggested that malignancies might have constituted a second “epidemic” within the AIDS epidemic. 2 Kaposi sarcoma (KS) and non-Hodgkin lymphoma (NHL) initially accounted for the majority of malignancy-associated morbidity and mortality in HIV diseases, with KS being the most common neoplasm in the pre-HAART era. 3 Malignancies in HIV-infected patients can be categorized into either AIDS-defining or other. Kaposi sarcoma, intermediate or high-grade B-cell NHL, and invasive cervical cancer (ICC) are AIDS-defining cancers (ADCs) based on the Centers for Disease Control and Prevention definition of AIDS. The advent of effective antiretroviral therapy (HAART) in 1996 resulted in a dramatic decrease in HIV-related morbidity and mortality along with the growth and aging of the population. Multiple studies have reviewed its impact on malignancy trends. In the most recent US-based and Swiss-based cohort trend analyses 4 -7 that ended in 2006 and 2007, a steep increase in the burden of non-AIDS-defining cancers (NADC) has been well reported. For example, non-AIDS-defining entities associated with HIV infection include Hodgkin’s lymphoma, multiple myeloma, anal cancer, lung cancer, hepatocellular carcinoma, renal cancer, skin cancer, neuroendocrine tumors, and others. Unfortunately, patients with NADCs often have more aggressive cancers and present with more advanced stages of the disease. 8 As a result, despite our efforts to emphasize and universalize HIV/AIDS treatment, malignancy still remains an important cause of death. Therefore, the need for targeted and effective screening strategies in the HIV population is needed.
However, the demographic distribution of malignancies in the HAART era have not been extensively investigated. The purpose of our study was to review the prevalence of AIDS-defining malignancies and NADC in the late antiretroviral therapy (ART) period. This was defined as 5 years at least after the widespread availability of potent ART, taking into consideration racial and gender variations.
Methods
After institutional review board approval, the study was conducted as a single-center retrospective observational study at Moffitt Cancer Center (MCC). Moffitt Cancer Center is a nationally recognized, nonprofit cancer treatment and research center located in Tampa, Florida.
Medical charts of 350 HIV infected patients, who were evaluated and/or treated at the MCC between January 1, 2000, and December 31, 2010, were reviewed. After excluding patients with a negative malignancy workup, 279 patients were finally included in the study. We retrospectively reviewed medical records and pathological reports on the diagnosis of malignancies in these 279 HIV infected patients.
Summarized demographic data included gender, race (white, black, or other), and sex. Clinical variables included CD4 cell counts (cells/μl) and plasma HIV-1 RNA (copies/mL) if available, at the time of cancer diagnosis. History of ART at diagnosis was also reviewed. Patients were considered to be taking ART if they were receiving any antiretroviral medication. Standard prevalence percentiles were calculated and assigned to the study end points.
Results
Of 279 patients included, 233 (83.5%) were male and 46 (16.4%) patients were female. Table 1 summarizes the baseline characteristics of HIV-infected patients at diagnosis with the most prevalent cancers noted (225 patients). Other less common cancers included in our study were not illustrated in the table.
Baseline Demographic and Clinical Characteristics of Patients at Cancer Diagnosis.

Abbreviations: AML, acute myeloid leukemia; ART, antiretroviral therapy; KS, Kaposi sarcoma; NHL, non-Hodgkin lymphomal; SCC, squamous cell cancer.
aAfter reviewing medical records, CD4 count and HIV plasma viral load at the time of cancer diagnosis were not available for some patients.
bHistory of ART at diagnosis was not available for all patients.
Among men, 78 (33.5%) had AIDS-defining malignancies. AIDS-related NHL was detected in 49 (21%) patients and KS in 29 (12%) patients. Two-third of male patients had NADC, with anal cancer being the most prevalent (8.5%), followed by Hodgkin lymphoma (6%; Figure 1A).

Gender difference (male and female). A, Distribution of malignancies in men; B, Distribution of malignancies in women.
In females, AIDS-related NHL was also the predominant malignancy with a prevalence of 19.5% followed by ICC (11%) and breast cancer (11%). Kaposi sarcoma and anal cancer were equally detected in 2% of women (Figure 1B). Of 279 patients, 53% were taking ART; 39.4% were not taking ART; and in 7.5% of the patients, it was unknown if they were taking ART.
The prevalence rates of AIDS-defining malignancies among those of white race was 34%, ranging from 21% for NHL to 13% for KS and 1.5% for ICC. Anal cancer was the most prevalent of the NADC in this group of patients, with 21 (7.7%) cases reported (Figure 2A).

Racial difference (white and black). A, Distribution of malignancies in white racial category; B, Distribution of malignancies in black racial category.
AIDS-defining malignancies were found in 36% of patients of black race, 60% of those had NHL. AIDS-defining NHL was followed by non-AIDS-related NHL. Breast cancer and anal cancer had a similar prevalence of 6.5% (Figure 2B).
Figure 3A summarize our results, illustrating the trend of ADC and NADC over the past 10 years. As a group, NADCs were more frequent than ADCs (134 NADC cases vs 68 ADC cases) in all subgroups (Figure 3B); however, individually each NADC cancer type was less common than NHL. Among all cancer cases, the median CD4 count at cancer diagnosis was 244 cells/mm3. CD4 counts at diagnosis were lower for most KS cases (85% CD4 < 200) with a median of 69 cells/mm3, similar to NHL cases which had a median CD4 of 153 cells/mm3 (57.7% CD4 < 200). The majority of patients diagnosed with melanoma, lung cancer, and hepatocellular carcinoma had a CD4 > 350 at the time of diagnosis (100%, 85.7%, and 71.4%, respectively.).
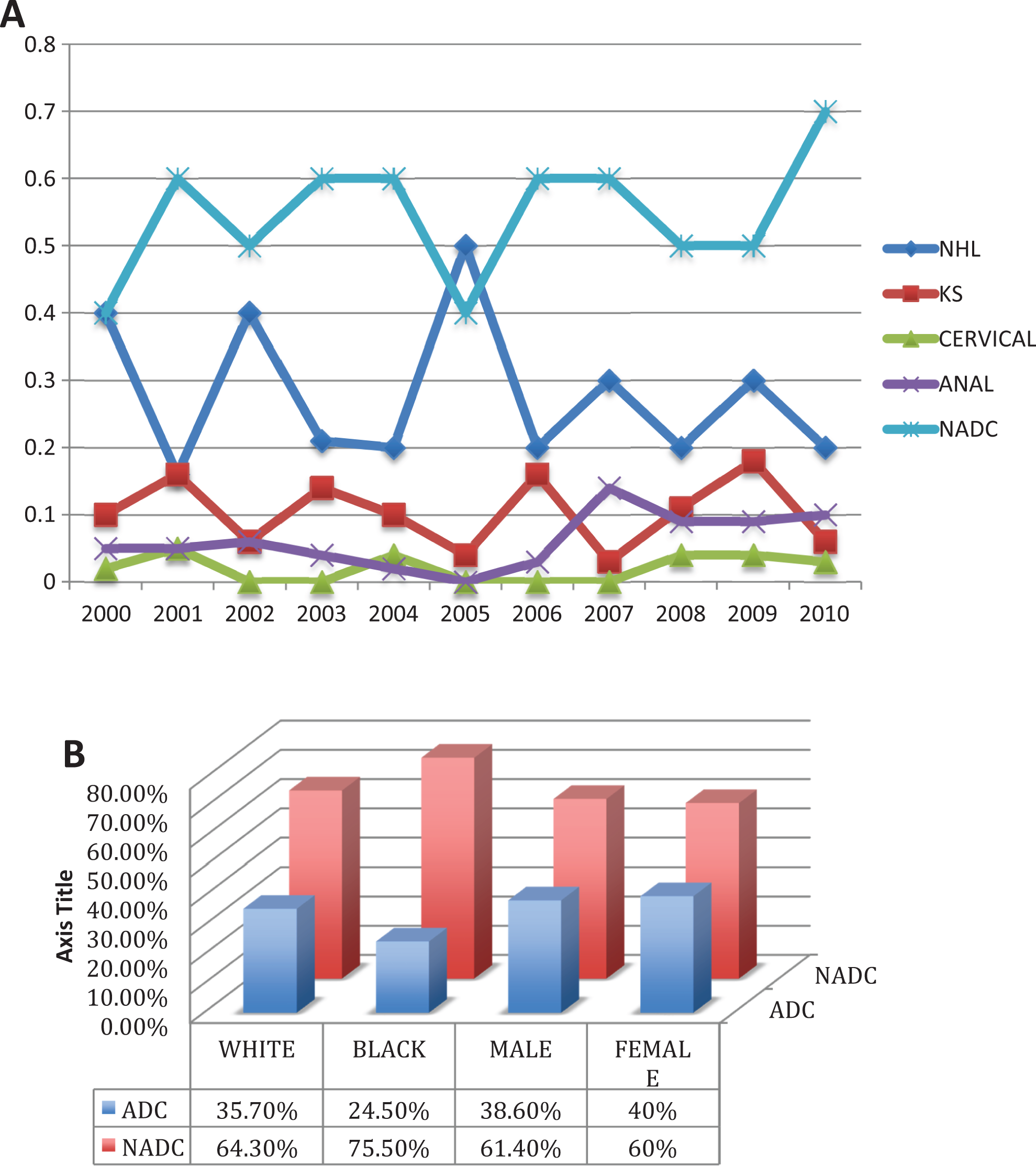
A, Trend of ADC and NADC over the past 10 years; B, NADCs were more frequent than AIDS-defining cancers (ADCs) in all subgroups: In the ART era, our study found NADC to be more prevalent than AIDS-defining malignancies with 60% versus 40%, respectively. Non-Hodgkin lymphoma remained the most common AIDS-related malignancy. Noted increased incidence of NADC, anal cancer was the predominant malignancy. ADC indicates AIDS-defining cancer; ART, antiretroviral therapy; NADC, non-AIDS defining cancers.
Discussion
While a decrease in the predominance of KS has been observed in the women and black racial groups, the HAART era did not show a significant impact on the NHL lymphoma rate in all groups. The overall impact of the introduction of ART was comparable to trends reported in the Swiss cohort. 4 The annual cancer burden in the AIDS population in the United States estimated by Shiels et al 6 and lately by the North Carolina Observational Clinical Cohort Study 9 both indicated a decline in the risk of ADCs as well, although KS and NHL remained the most common malignancies. However, these aforementioned studies didn’t stratify their results by gender or racial variations.
The most important limitation in our study is the relatively modest representation of the nonwhite male HIV population, the small number in each specific cancer type, and also the fact that it is a retrospective single-center study. The lack of detailed information about the ART, CD4 count, and HIV plasma viral load in a significant percentage of our patients limited our ability to conclude any association. The study has much strength mainly because of large number of patients included over 10 years, spanning the last decade (2000-2010), and with its representation of the late ART period (Figure 3A), giving time for malignancy trends to reshape and allow us to compare results with previous observational studies. In addition, we were able to highlight ADC and NADC gender and racial variations.
In a retrospective study in France, studying causality of death among HIV-infected patients in the year 2000, malignancies were found to be the second most common cause of death after AIDS, to which ADC and NADC contributed nearly equally (15% and 13% of all deaths, respectively). 10
The risk of developing lung cancer seems to be 3-fold higher in HIV infected patients than in the general population of the same age, mostly in the form of adenocarcinoma. 11 In a retrospective study conducted in Baltimore studying the impact of HIV on lung cancer incidence and survival, after adjusting for smoking, 12 they noted that HIV was associated with 4 times the risk of death compared to HIV-negative patients after accounting for cancer stages. Given the poor prognosis for HIV-infected patients with malignant disease, we should encourage the need for a high level of suspicion and for routine cancer screening in this population.
Our findings emphasize the need for targeted and effective screening strategies of the aforementioned prevalent cancers in each subgroup. Unanswered questions remain about the factors behind this increased prevalence of NADC in the HIV population in late ART period. Lot of previous reviews contributed to the longevity offered to the patient with HIV with the new potent HAART, leading to prolonged and cumulative exposure to oncogenic viruses and environmental carcinogens.
We should also suspect a possible carcinogenic effect for these potent antiviral meds, as well the role of HAART-associated immune reconstitution that may be contributing to the increased prevalence of NADC. 13,14 Additional research is required to understand these hypotheses. Highly active antiretroviral therapy regimens as well as coinfections with other cancerogenic viruses such as hepatitis C, Human papillomavirus (HPV), and Hepatitis B virus (HBV) should be the highlight of future studies.
National Institutes of Health currently conducting a cancer genomic study in HIV positive patient with NHL, cervical cancer, and lung cancer based on their high rates of incidence and mortality among HIV-positive patients.
This high cancerogenic potential emphasizes the need to implement cancer screening guidelines specific for the HIV population targeting the most prevalent NADC identified in the ART era: anal cancer, skin/oral squamous cell carcinoma, Hodgkin lymphoma, melanoma, and lung cancer. The high incidence of some malignancies in HIV-positive population supports early and sustained ART, lifestyle modification, sunscreen, smoking cessation and judicious cancer screening such as skin exam, cervical and anal Pap test, computed tomography scan chest, and so on.
In conclusion, we were able to identify the malignancy with the highest prevalence in different racial and gender groups in the ART era. Our study found NADC to be more prevalent than AIDS-defining malignancies (33%). As opposed to KS, AIDS-related lymphoma remained the predominant malignancy independent of gender and race. Among NADC, we were able to detect differences in different subgroups; anal cancer was more prominent in white males. However, in the black racial group and in females, anal cancer followed NHL or breast cancer, respectively.
Moreover, KS and NHL continue to be more prevalent in patients with AIDS with a CD4 < 200. However, the majority of NADC, excluding hematologic malignancies (Acute myeloid leukemia [AML], Hodgkin lymphoma) were noted to occur when the CD4 count is above 200.
The increasing incidence of some of the NADC is expected as this population is living longer with chronic exposure of viral replication of virus with oncogenic potential such as HPV, HBV, Epstein-Barr virus (EBV), and Human herpesvirus 8 (HHV-8). Early ART initiation, aggressive vaccination, and judicious cancer screening are the cornerstone of cancer prevention of this growing population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.